We use cookies to make sure that our website works properly, as well as some ‘optional’ cookies to personalise content and advertising, provide social media features and analyse how people use our site. Further information can be found in our Cookies policy
Ocimum sanctum L., commonly known as Tulsi or Holy Basil, is a sacred medicinal plant in Ayurveda and other traditional systems of medicine. Its wide-ranging pharmacological properties, particularly its anticancer potential, have become a subject of modern biomedical interest. This review offers a detailed examination of Tulsi’s bioactive phytochemicals, mechanistic actions in inhibiting cancer progression, synergistic effects with chemotherapy, and current limitations and opportunities in therapeutic development. By compiling extensive preclinical data and existing clinical observations, we aim to present a clear understanding of Tulsi’s role in integrative oncology.
Cancer continues to be a major global health burden, causing millions of deaths annually. While modern treatments like chemotherapy, radiation, and immunotherapy have improved survival, side effects and resistance remain significant concerns. Natural products, especially medicinal plants, are gaining momentum as complementary approaches in oncology. Among these, Ocimum sanctum (Tulsi), revered for centuries in Indian households and Ayurvedic texts, shows considerable promise. Traditionally used to treat respiratory, cardiac, metabolic, and infectious conditions, Tulsi has demonstrated emerging efficacy in preclinical cancer models [1–3].
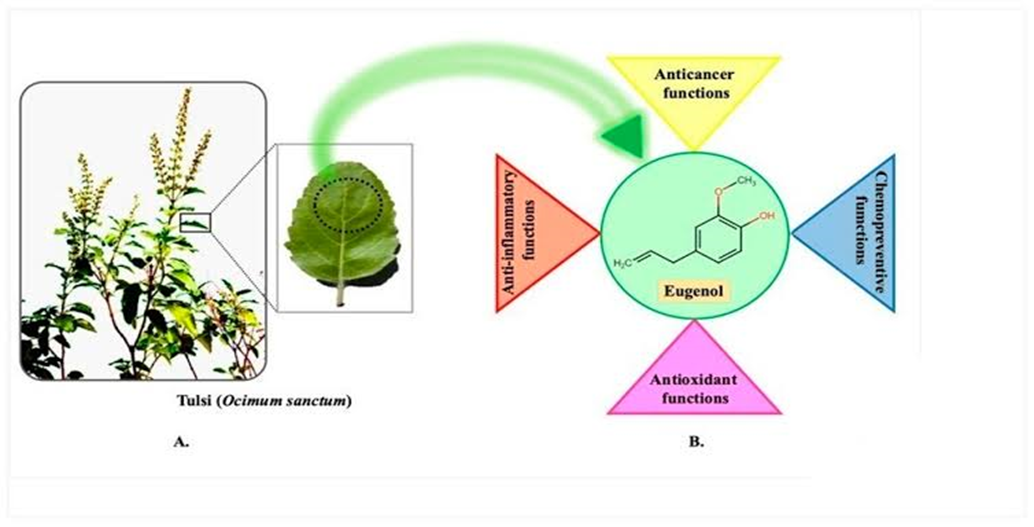
Cancer continues to be one of the leading causes of death globally, prompting the search for safer and more effective therapeutic strategies. In recent years, medicinal plants have garnered attention for their potential role in cancer prevention and treatment. Ocimum sanctum L., commonly known as Tulsi or Holy Basil, is a revered herb in traditional Indian medicine, particularly Ayurveda. Renowned for its adaptogenic, antioxidant, and anti-inflammatory properties, Tulsi has recently shown promising anticancer activity in both in vitro and in vivo studies. Its rich phytochemical profile, including compounds like eugenol, ursolic acid, and rosmarinic acid, contributes to its ability to modulate multiple cancer-related pathways, offering a natural and multi-targeted approach to cancer therapy.
2. Phytochemical Composition of Ocimum sanctum Tulsi's anticancer effects stem from a diverse array of phytochemicals, each with specific molecular targets:
Eugenol: The most studied component, eugenol induces apoptosis in cancer cells by disrupting mitochondrial function and modulating gene expression related to cell survival and inflammation [4–5].
Ursolic Acid: A pentacyclic triterpenoid that inhibits cell proliferation, metastasis, and angiogenesis through regulation of NF-κB and STAT3 pathways [6–7].
Rosmarinic Acid: Known for antioxidant activity, it reduces DNA damage and has been shown to inhibit cancer cell invasion and migration [8–9].
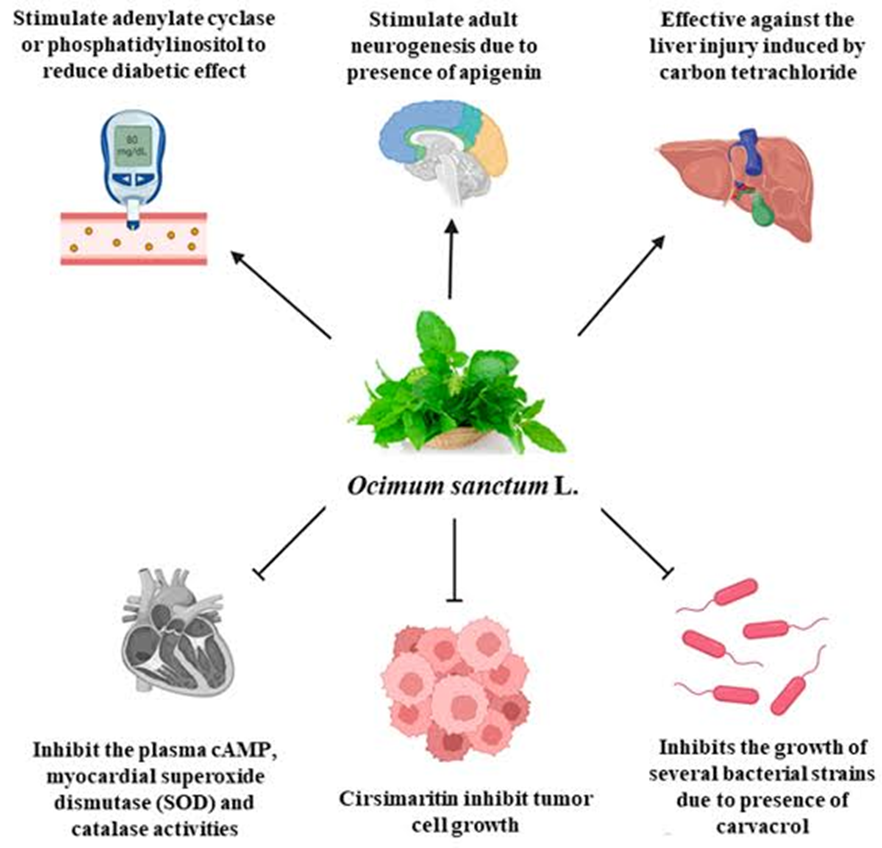
Apigenin: A flavonoid that arrests the cell cycle and promotes apoptosis via caspase activation and inhibition of PI3K/Akt signaling [10].
β-Caryophyllene: A sesquiterpene with anti-inflammatory and anticancer properties, particularly through CB2 receptor agonism [11].
These compounds work synergistically to enhance Tulsi’s overall therapeutic index.
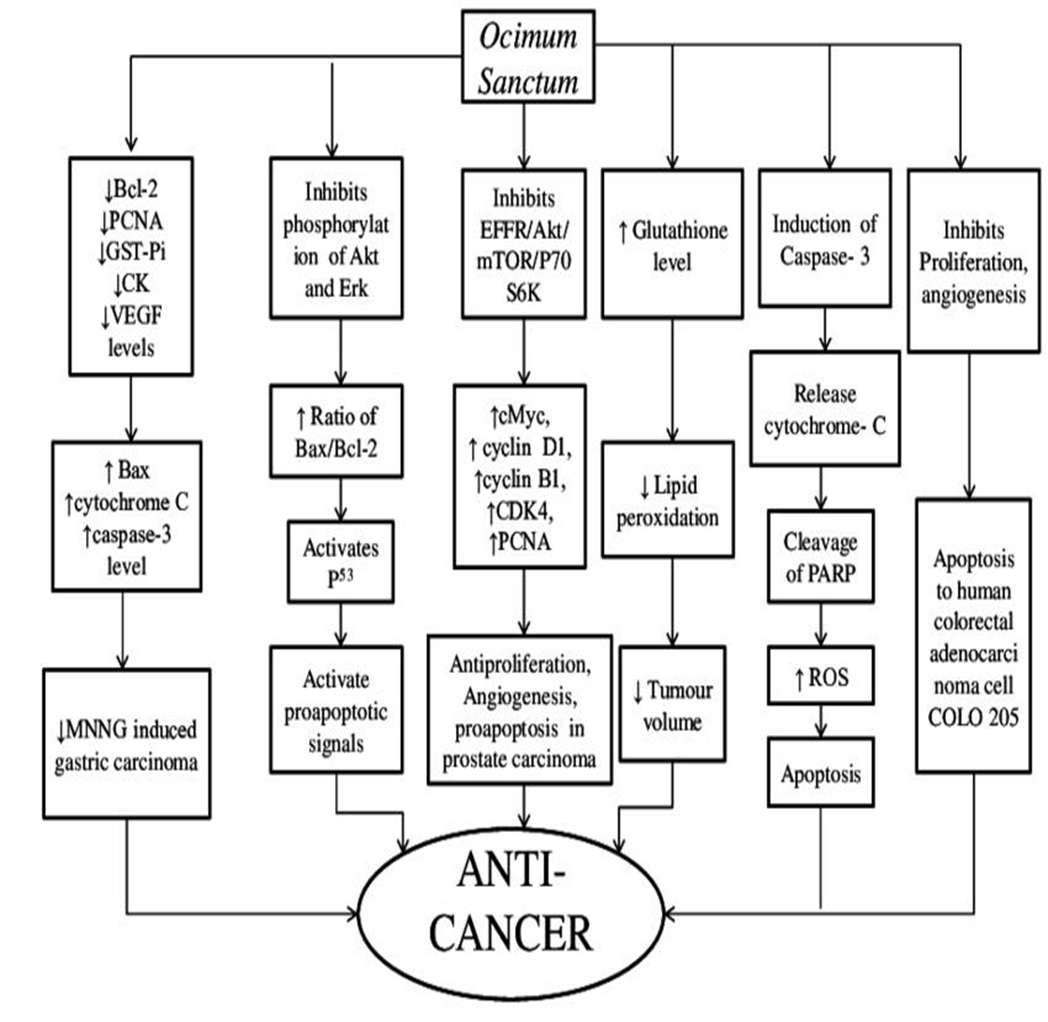
3. Mechanisms of Anticancer Action Tulsi targets several hallmarks of cancer, making it a multi-faceted anticancer agent:
Apoptosis Induction: Tulsi compounds activate both intrinsic and extrinsic apoptotic pathways. This includes mitochondrial depolarization, increased Bax/Bcl-2 ratio, and caspase activation [12].
Cell Cycle Arrest: Tulsi extracts downregulate cyclins D1 and E and inhibit CDK4/6, leading to G1 phase arrest in various cancer cell lines [13].
Anti-angiogenesis: Tulsi suppresses VEGF expression, inhibits endothelial cell tube formation, and reduces MMP-9 expression, all critical for tumor vascularization [14].
Antioxidant and Anti-inflammatory Activity: Tulsi neutralizes ROS and suppresses inflammation through COX-2 and IL-6 inhibition, thereby modulating the tumor microenvironment [15].
Signal Transduction Modulation: Tulsi inhibits PI3K/Akt, MAPK, and NF-κB signaling, which are central to cell survival, proliferation, and metastasis [16–18].
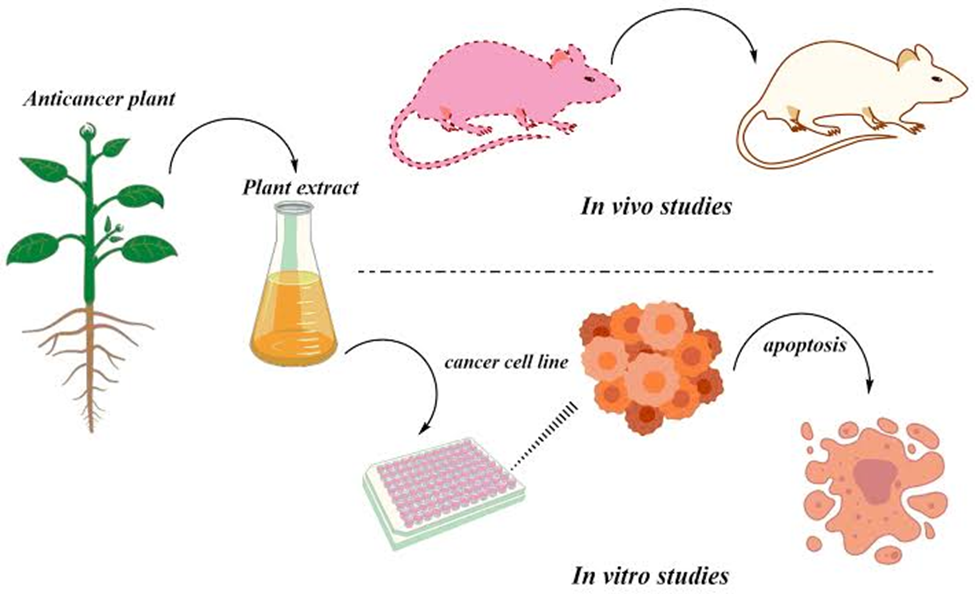
4. Evidence from Preclinical Studies
4.1 In vitro Studies:
In MCF-7 breast cancer cells, Tulsi induced DNA fragmentation and apoptosis in a dose-dependent manner [19].
In AGS gastric cancer cells, the extract caused mitochondrial dysfunction and increased oxidative stress markers [20].
In K562 leukemia cells, Tulsi promoted apoptosis through Fas receptor upregulation [21].
In oral squamous carcinoma cells, Tulsi extract inhibited proliferation, migration, and MMP-2 activity [22].
4.2 In vivo Studies:
Tulsi extract significantly suppressed tumor growth in mice bearing Ehrlich ascites carcinoma, with enhanced survival rates [23].
In chemically induced lung and skin carcinogenesis models, Tulsi reduced tumor incidence and multiplicity [24].
Histological analyses from these studies consistently showed reduced neovascularization and mitotic index in Tulsi-treated groups.
5. Synergistic Effects with Chemotherapy Combining Tulsi with standard chemotherapeutics (e.g., doxorubicin, cisplatin) has shown promising results:
Enhanced efficacy: Co-treatment resulted in higher apoptosis rates and reduced drug doses needed to achieve similar outcomes [25].
Reduced toxicity: Tulsi’s antioxidant properties help mitigate organ damage (e.g., hepatotoxicity, nephrotoxicity) often associated with chemotherapy [26].
Clinical investigations on Tulsi in oncology are limited but encouraging:
In small cohort studies, patients receiving Tulsi supplements alongside chemotherapy reported reduced fatigue, nausea, and improved appetite [28].
Tulsi formulations have demonstrated immunomodulatory effects, including increased NK cell activity and cytokine balance [29].
However, larger randomized clinical trials with standardized extracts and well-defined endpoints are needed.
7. Challenges and Future Directions
Standardization and Quality Control: Variability in Tulsi chemotypes, growing conditions, and extraction methods hampers reproducibility.
Bioavailability: Many of Tulsi's active components suffer from low oral bioavailability. Nanoformulations and phytosome delivery systems are being investigated to enhance therapeutic levels.
Regulatory Hurdles: Tulsi remains categorized as a dietary supplement in many countries, limiting its pharmaceutical development. Robust clinical data will be essential for repositioning it as an approved adjunct therapy.
Future research should prioritize pharmacokinetic profiling, formulation innovations, and controlled clinical trials.
8. CONCLUSION
Tulsi (Ocimum sanctum) represents a compelling candidate for cancer chemoprevention and adjunct therapy. Its pleiotropic effects—ranging from apoptosis induction and angiogenesis inhibition to immunomodulation—support its integration into holistic cancer management strategies. With improved formulation, standardization, and clinical validation, Tulsi could become a cornerstone of plant-based oncologic therapeutics.
REFERENCES
Baliga MS, et al. J Ayurveda Integr Med. 2013;4(4):198–205.
Cohen MM. J Ayurveda Integr Med. 2014;5(4):251–259.
Mondal S, et al. Evid Based Complement Alternat Med. 2011;2011:527351.
Prakash P, Gupta N. Indian J Physiol Pharmacol. 2005;49(2):125–131.
Manikandan P, et al. Pharmacol Rep. 2010;62(3):564–576.
Yoon Y, et al. Cancer Lett. 2010;297(2):128–136.
Kashyap D, et al. Anticancer Agents Med Chem. 2016;16(10):1235–1244.
Aherne SA, O’Brien NM. Cancer Lett. 2002;177(1):33–38.
Russo M, et al. Nutrients. 2016;8(9):539.
Shukla S, Gupta S. Int J Oncol. 2010;36(6):1335–1342.
Gertsch J, et al. Proc Natl Acad Sci U S A. 2008;105(26):9099–9104.
Das S, et al. Biomed Pharmacother. 2020;128:110259.
Hibasami H, et al. Oncol Rep. 2006;15(1):267–271.
Lin CW, et al. J Cell Biochem. 2005;94(2):307–318.
Pattanayak P, et al. J Ayurveda Integr Med. 2010;1(4):241–249.
Ahmed M, et al. Phytother Res. 2016;30(3):479–490.
Bhattacharyya P, Bishayee A. Curr Drug Targets. 2013;14(12):1199–1216.
Sharma M, et al. Anticancer Res. 2016;36(12):6365–6370.
George J, et al. J Pharm Pharmacol. 2011;63(2):231–239.
Roy A, et al. Toxicol In Vitro. 2011;25(4):699–707.
Singh S, et al. J Ethnopharmacol. 2007;109(1):27–34.
Magesh V, et al. Phytother Res. 2009;23(6):817–824.
Shetty S, et al. J Exp Ther Oncol. 2012;9(1):47–56.
Anbarasi K, et al. Life Sci. 2006;78(12):1371–1377.
Nagini S. Curr Med Chem Anticancer Agents. 2005;5(5):393–399.
Banerjee S, et al. Cancer Lett. 2005;223(2):145–153.
Sumbul S, et al. Biomed Pharmacother. 2011;65(7):489–497.
Gupta S, et al. Indian J Exp Biol. 2002;40(7):765–773.
Rastogi RP, Mehrotra BN. Compendium of Indian Medicinal Plants. 1999.
Goyal PK, et al. J Radiat Res. 2007;48(5):367–376.
Reference
Baliga MS, et al. J Ayurveda Integr Med. 2013;4(4):198–205.
Cohen MM. J Ayurveda Integr Med. 2014;5(4):251–259.
Mondal S, et al. Evid Based Complement Alternat Med. 2011;2011:527351.
Prakash P, Gupta N. Indian J Physiol Pharmacol. 2005;49(2):125–131.
Manikandan P, et al. Pharmacol Rep. 2010;62(3):564–576.
Yoon Y, et al. Cancer Lett. 2010;297(2):128–136.
Kashyap D, et al. Anticancer Agents Med Chem. 2016;16(10):1235–1244.
Aherne SA, O’Brien NM. Cancer Lett. 2002;177(1):33–38.
Russo M, et al. Nutrients. 2016;8(9):539.
Shukla S, Gupta S. Int J Oncol. 2010;36(6):1335–1342.
Gertsch J, et al. Proc Natl Acad Sci U S A. 2008;105(26):9099–9104.
Das S, et al. Biomed Pharmacother. 2020;128:110259.
Hibasami H, et al. Oncol Rep. 2006;15(1):267–271.
Lin CW, et al. J Cell Biochem. 2005;94(2):307–318.
Pattanayak P, et al. J Ayurveda Integr Med. 2010;1(4):241–249.
Ahmed M, et al. Phytother Res. 2016;30(3):479–490.
Bhattacharyya P, Bishayee A. Curr Drug Targets. 2013;14(12):1199–1216.
Sharma M, et al. Anticancer Res. 2016;36(12):6365–6370.
George J, et al. J Pharm Pharmacol. 2011;63(2):231–239.
Roy A, et al. Toxicol In Vitro. 2011;25(4):699–707.
Singh S, et al. J Ethnopharmacol. 2007;109(1):27–34.
Magesh V, et al. Phytother Res. 2009;23(6):817–824.
Shetty S, et al. J Exp Ther Oncol. 2012;9(1):47–56.
Anbarasi K, et al. Life Sci. 2006;78(12):1371–1377.
Nagini S. Curr Med Chem Anticancer Agents. 2005;5(5):393–399.
Banerjee S, et al. Cancer Lett. 2005;223(2):145–153.
Sumbul S, et al. Biomed Pharmacother. 2011;65(7):489–497.
Gupta S, et al. Indian J Exp Biol. 2002;40(7):765–773.
Rastogi RP, Mehrotra BN. Compendium of Indian Medicinal Plants. 1999.
Goyal PK, et al. J Radiat Res. 2007;48(5):367–376.
Ashvini Dhurandar
Corresponding author
Collage Name. Samarth Collage Of Pharmacy Deulgaon Raja
Ashvini Dhurandar*, Pranjal Salunke, Dr Gopalkrishna Sithaphle, Dr. Prafulla Tathe, Effect Of Sanctum on Cancer Progression and It’s Effective Therapeutic Activity, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 1693-1698. https://doi.org/10.5281/zenodo.15619519
 10.5281/zenodo.15619519
10.5281/zenodo.15619519
