
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3 Geeta Institute of Pharmacy, Geeta University, Naultha-132145, Panipat, Haryana
4 Panipat Institute of Engineering and Technology, Samalkha, Panipat-132102, Haryana
The healing process of wounds is a complicated thrust of intercellular and molecular events designed to repair the skin barrier. Conditions such as diabetes, increasing age, malnutrition, and infections can cause wounds to develop into chronic skin sores that refuse to heal. This phenomenon is a major issue in healthcare. Physiological alterations during the healing process, such as hemostasis, inflammation, proliferation, and maturation, as well as recovery-modifying factors, are also addressed. It addresses different categories of wounds, treatment regimens, and assessment tools such as NERDS, STONEES, and TIMES. The review looks at how traditional wound dressings stack up against new technologies like hydrogels, smart hydrogels, scaffolds, nanoparticles, coacervates, and advanced drug delivery systems. It also highlights cutting-edge approaches like stem cell therapy, genetic therapy, nanotechnology, 3D bioprinting, AI-based tools, and bioactive compounds, emphasizing their potential to accelerate healing, enhance tissue regeneration, and provide more personalized treatments. In addition, the review considers complementary therapies involving herbs and nutrients. Ultimately, it demonstrates the need for a patient-centered strategy that blends innovative technologies with conventional methods to achieve more effective wound care and improved outcomes.
Wound healing is a complicated and varied a dynamic mechanism influenced by different cellular functions that need to be accurately coordinated to successfully mend damaged tissue. Interference in cellular functions associated with wounds, as observed in diabetes and aging, may lead to challenges in recovery and the development of chronic, non-healing sores. These injuries present a considerable socioeconomic challenge because of their commonality and tendency to reoccur. Therefore, a better knowledge of the molecular and clinical mechanisms underlying wound healing is desperately needed.
A significant amount of radiation exists in the environment, creating difficulties for our skin and body. This severe external environment frequently leads to skin damage, so it is not surprising that our skin has advanced healing mechanisms that enable it to recover swiftly and effectively. Even with significant inherent healing capacity, various cellular components of a person's injury response may become diminished, jeopardizing wound healing. This reduction is typically caused by systemic pathological alterations, like those linked to aging or unmanaged diabetes. Age and diabetes are undoubtedly significant risk factors for the development of a chronic wound.
(For example, one that takes longer than 12 weeks to recover). Regrettably, these persistent injuries (mainly diabetic foot ulcers, pressure sores, and venous ulcers) represent a significant region with unmet health requirements, rising significantly worldwide. The processes our bodies employ to repair injuries are well comprehended and entail intricate interactions among inflammatory mediators and cells. Injuries have the ability to heal naturally by sutures or staples can be used to bring the edges together, or secondary aim or alternative methods that facilitate healing through primary intention [1].
The injuries can be classified into 2 categories:
a) Open wounds - An open wound refers to a rupture in the skin or tissue that reveals internal organs and tissue to the external environment.
b) Closed wounds - The skin's outer layer is unbroken, but the tissues beneath may be harmed. Stage 1 of pressure injuries. As soon as the injury happens, the recovery process starts. Damaged tissue is fixed, absent tissue is substituted, and the epithelial layer is replaced. Keratinocytes, fibroblasts, immune cells and endothelial cells each significantly contribute to support, inflammation, cellular movement, and blood vessel formation. The difference between open and closed wounds, highlighting tissue exposure in open wounds and intact skin in closed wounds are shown in fig.1.
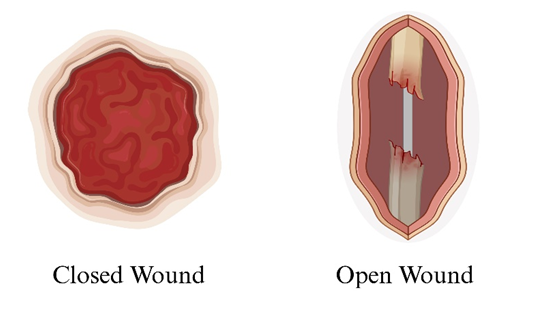
Fig 1: shows closed wound and open wound respectively.
Types of wound healing:
1) Primary healing – The closure of a wound where the edges are closely aligned. For example, surgical incisions.
2) Secondary healing - This stage begins if the wound is affected by infection or low oxygen levels.
3) Tertiary healing - This happens when the healing process by secondary intention is deliberately halted, and the wound is closed with stitches.
Wound healing refers to the procedure the skin undergoes to mend harm inflicted by injuries. Wound healing is categorized into three primary types: primary, secondary, and tertiary healing.
Each injury undergoes multiple phases of recovery, based on the wound type and its extent. Grasping these categories and the phases of the wound healing process can assist individuals in knowing how to properly care for a wound.
Primary Wound Healing:
Primary wound healing, also known as healing by primary intention, occurs when a wound is closed directly by medical techniques such as stitches, staples, or adhesives. This approach reduces tissue damage and enables the body to concentrate on healing a smaller, confined region instead of the entire area of the original wound. For example, a physician could sew a significant laceration instead of permitting the body to mend across the whole wound.
Secondary Intention Wound Healing:
Also known as secondary intention wound healing, secondary intention wound healing, occurs when a non- suturable wound leads to substantial tissue loss. In such cases, physicians will permit the injury to mend naturally.
This might be more common for wounds with a rounded border, impact irregular regions, or happen on body parts where movement obstructs stitches or other fastening techniques.
Healing of secondary wounds relies on the body's inherent healing mechanisms. This procedure requires extra time, likely due to a larger wound size, the possibility of infection and contamination, as well as other elements, including the administration of specific medications.
Tertiary Wound Healing:
This kind of wound healing, often referred to as healing by delayed primary closure, occurs when the wound closure process needs to be prolonged.
This may be necessary if a doctor believes that sealing a wound might entrap harmful bacteria inside. In these circumstances, they could wait for the outcome of additional treatments or let the wound heal before suturing it. Various kinds of wounds exist, determined by elements like the origin of the injury and any underlying conditions that might contribute to it. The type could change how physicians manage the injury or other elements in the recovery process.
Wounds can generally be classified as open or closed. A closed wound is a type of injury that doesn't penetrate the skin's surface but harms the tissues beneath it. A bruise serves as a typical illustration of this. Conversely, open wounds pierce the skin's surface and can also harm the tissues beneath [2].
Varieties of Injuries:
1) Abrasions: These occur due to the skin being rubbed or scraped in opposition to a firm surface.
2) Cuts: These are more profound wounds created by sharp items, like a knife, or pointed edges.
3) Holes: These are slight, but profound openings created by a sharp, elongated item, like a spike.
4) Burns: These occur due to exposure to open flames, extreme heat, harsh cold, specific chemicals, or electrical sources
5) Avulsions: This term describes the total or partial separation of skin and tissues.
Chronic wounds can lead to skin openings that require healing. These include pressure sores, different types of pressure injuries, and diabetes-related ulcers.
PATHOPHYSIOLOGY OF WOUND RECOVERY
MECHANISM:
Tissue reconstitution happens through a systematic sequence of overlapping phases during the healing of wounds.
This procedure involves: ~
1) Blood clotting
2) Swelling
3) Expansion and concludes with the development of fully formed tissue damage.
HEMOSTASIS:
Hemostasis commences right after an injury takes place. Hemorrhaging from the injury is managed by narrowing blood vessels, forming a platelet plug, ongoing activation of the coagulation cascade, stopping clot creation, and finally, the dissolution of via fibrinolysis of the clot. When the vascular endothelium is damaged, blood flows to the damaged area, exposing the basal lamina. Platelets that have been activated then bind to the exposed collagen, initiating the release of various growth factors, inflammatory mediators, and cytokines [3].The intrinsic and extrinsic pathways of coagulation initiate, leading to the formation of a fibrin clot that closes off and stops additional blood loss.
The production of the extracellular matrix, chemotaxis, epithelialization, and angiogenesis are all aided by the cytokines produced during the hemostatic phase. These consist of platelet-derived growth factor, fibroblast growth factor, epidermal growth factor, transforming growth factor-beta, and vascular endothelial growth factor.
INFLAMMATION:
After platelets are activated in the first few days following an injury, inflammatory cells go to the site of the damage. Prostaglandins and histamine are two examples of the vasoactive cytokines secreted by mast cells that improve capillary permeability and promote local dilatation to aid in migration.
Initially, the predominant kind is neutrophils and are attracted to the wound area by bacterial components. Neutrophils engulf the bacteria and decay tissue, leading to the pus observed in injuries following the initial 48 to 72 hours. Monocytes then develop into macrophages, which go on cleaning the wound by eliminating the matrix and other cellular waste products, including fibrin and dead neutrophils. Macrophages are essential for the release of transforming growth factor- beta, platelet-derived growth factor, fibroblast growth factor, and epidermal growth factor, among other inflammatory cytokines. Because of these functions, macrophages are essential for efficient wound healing; preventing macrophage activity results in a longer healing time.
PROLIFERATION:
The proliferative phase, which occurs three to twenty-one days after the injury, includes activities such as angiogenesis, granulation tissue creation, collagen build-up, and epithelialization.
The main goal of this stage is to close the imperfection in the wounds. Low oxygen circumstances inside the wound bed stimulate endothelial cells to produce nitric oxide (NO), prompting the secretion of growth factor for vascular endothelium and promoting angiogenesis.
Secretion of platelet-derived growth factor and fibroblast growth factor also promotes angiogenesis, supplying oxygen, glucose, and other vital components required for appropriate wound healing. In this setting, the newly generated extracellular matrix serves as the foundation for the endothelium, which protrudes from existing blood vessels.
Oxygen levels return to normal once blood flow has been restored to the area, while levels of nitric oxide and vascular endothelial growth factor decline to hinder angiogenesis progression. This self-regulation system helps avoid the creation of aberrant scars and excessive collagen synthesis. The Wound Healing Foundation (WHF) classifies chronic wounds into different types according to their causes as illustrated in fig.2. Elastin and collagen are produced by migrating fibroblasts to form the new extracellular matrix needed for granulation tissue and vascular support. Granulation tissue is a kind of connective tissue with a rich supply of blood vessels that plays a crucial role in the final phases of wound healing and maturation and remodeling. Various types of wounds that don't heal easily are illustrated in fig.3
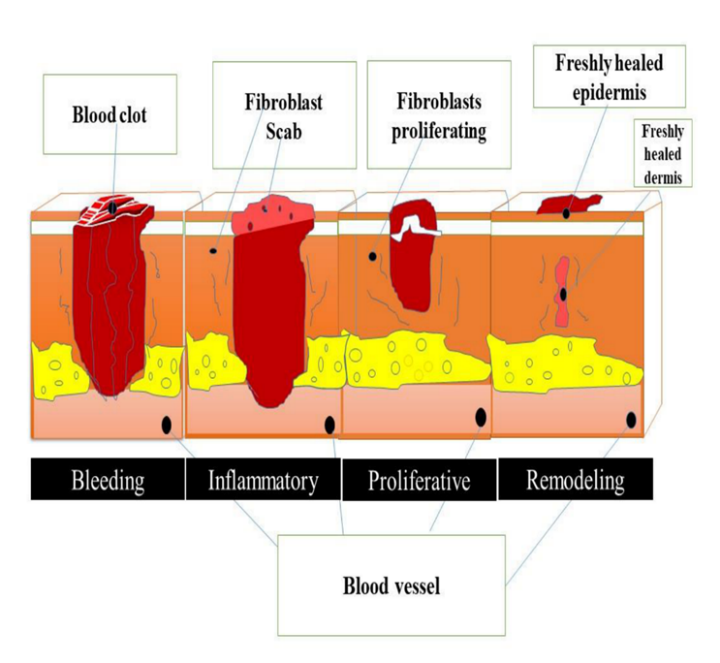
Fig 2: The Wound Healing Foundation (WHF) categorizes chronic wounds according to their causes: arterial insufficiency ulcers, diabetic ulcers, venous ulcers, and pressure ulcers, and wounds caused by radiation, surgery, and infections
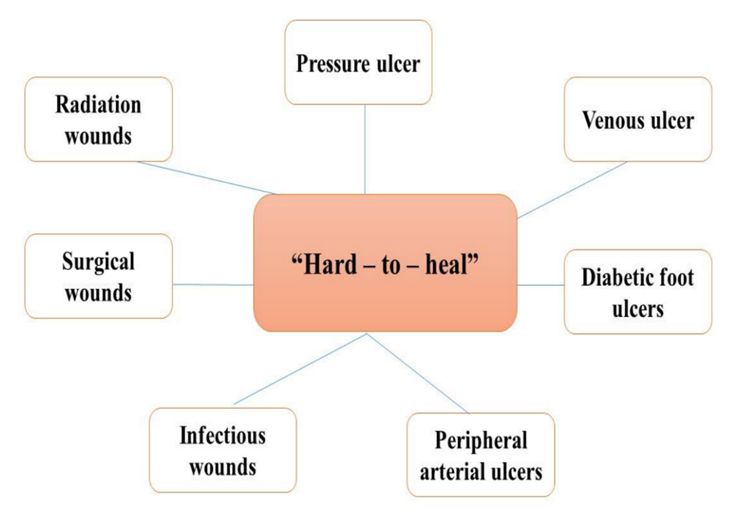
Fig 3: Types of wounds occurs in body which are Hard-to-heal.
MATURATION:
The maturation phase, which is the last stage of wound healing, includes collagen cross-linking, wound remodeling, and contraction. First produced by fibroblasts, type 3 collagen is thinner than mature type 1 collagen, which is often present in healthy skin. Scar development occurs when type 1 collagen replaces type 3 collagen found in granulation tissue during the maturation phase. The increased type 1 collagen is linked to the stronger wounds that are seen four to five weeks after they have healed. 80% of the initial strength of a wound will be restored three months after the damage [4].
MULTIPLE ELEMENTS CAN AFFECT WOUND RECOVERY:
WOUND MANAGEMENT CARE PROTOCOL:
Considering the range of reasons, types of injuries, and the distinct characteristics of comorbidity. Consequently, it is essential to record a comprehensive medical history regarding the onset of the wound, any prior treatments and therapies, its progression leading to the visit to the medical facility, associated illnesses and their treatments, along with other pertinent details concerning the patient’s condition (e.g., nutritional assessment). It is crucial to understand that a compromised wound can promote the onset of systemic conditions, creating a detrimental cycle for the process of rehabilitation.
The primary method of assessing a wound is visual inspection, which emphasizes the location, size, and extent of the lesion, fluid output, and the tissue type in the affected region.
Secondly, it is necessary to evaluate the injuries for microbial contamination. Common infection symptoms including fever, discomfort, swelling, and redness may not always be apparent. For identifying chronic wounds that are infected, two mnemonics are suggested: NERDS, which has a sensitivity of 73% and a specificity of 80.5% when three criteria are satisfied, and STONEES, which has a sensitivity of 90% and a specificity of 69.4% when at least three indications are present. The wound is extensively colonized or has biofilm when NERDS criteria are met. The existence of STONEES signifies that the chronic wound has an infection as shown in fig.4.
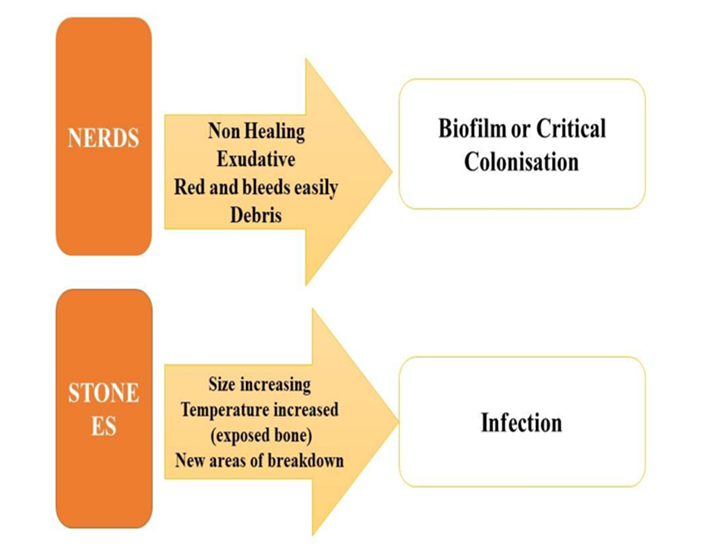
Fig 4: To aid medical treatment providers, twenty years ago, the TIMES acronym was first used and continues to be utilized. It provides information to create a treatment plan and standardizes the metrics used in wound assessment.
TYPES OF DELIVERY SYSTEM IN WOUND HEALING
An effective wound care regimen needs to integrate a comprehensive method with localized treatments and adequate nutritional assistance to promote effective recovery. Systemic treatment primarily addresses comorbidities or the risk of septicemia, whereas topical therapy focuses on adjusting the molecular reactions taking place in the pathological pathways at the area of injury. The ultimate goal of a topical approach is to restore skin integrity while minimizing scar damage (including fibrosis, hypertrophy, keloids, red fibrous growths, and contractures).
Wound dressings have progressed through history, starting with clay tablets (2500BC) and cotton gauze (initially created in 1891) to modern dressings, which started evolving after showing (in 1948) the benefits of humid environments for venous ulcers. At present, more than 2000 medicinal goods are included in dressings, ranging from topical ointments, lotions, and gels to advanced technology like 3D stem cell printers and bacteria-fighting lasers. About 30% of the market for injury management products is made up of wound cleansers, with dressings closely trailing.
An ideal wound dressing necessitates a balance between its advantages, patient safety, and economic viability. An ideal wound dressing should be biocompatible, biodegradable, and have ideal permeability for water vapor to create and sustain a conducive atmosphere throughout the recovery procedure. Moreover, it must conform precisely to the shape of the injury without sticking to the wound surface, provide a barrier against microbial infiltration, physical and thermal stress, and aid in maintaining moisture balance in the affected region. The handling of chronic wounds through topical therapies incurs significant expenses for the healthcare system.
Wound dressings are classified into traditional or conventional types (like cotton gauze, dressings, lint, adhesive strips) and contemporary multifunctional varieties (such as foams, membranes, hydrocolloids, hydrogels, nanocomposites). Traditional dressings, referred to as passive wound dressings, are effective in offering coverage and support to contemporary dressings. The dressings mentioned earlier are characterized as interactive components that influence the overall healing process by regulating the microenvironment of the injured tissue (pH, temperature, and moisture), encouraging granulation and reepithelization, and inhibiting the growth of microorganisms [5].
ADVANCEMENTS IN WOUND HEALING: PROGRESSING PAST CONVENTIONAL TECHNIQUES
Biological Bandages: Imitating Nature's Framework
Natural materials such as chitosan, collagen, and hyaluronic acid create biological dressings that foster an ideal setting for wound healing. Serving as scaffolds, they facilitate cell proliferation, angiogenesis, and regulated release of therapeutic agents, improving tissue regeneration.
Stem Cell Treatment: Utilizing Regenerative Capabilities
For wound healing, stem cells, including mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs)—offer promising alternatives. Their capacity to transform into different cell types and influence the inflammatory response speeds up wound healing and tissue regeneration, providing hope for difficult wounds.
GENE Treatment: Focusing on Molecular Mechanisms
Gene therapy delivers therapeutic genes to activate particular molecular pathways related to wound healing. Elevated amounts of growth factors like vascular endothelial growth factor (VEGF) encourage angiogenesis, collagen accumulation, and tissue regeneration, providing a focused method to improve healing results.
Nanotechnology: Engineering Healing at the Nano Level Nanotechnology allows for exact manipulation of materials on the nanoscale for wound treatment. Nanoparticles, nanofibers, and nanogels transport drugs, growth substances, and antimicrobial compounds directly to the location of the wound, improving therapeutic effectiveness while reducing systemic side effects.
3D Bioprinting: Tailored Tissue Structures
3D bioprinting transforms tissue engineering by producing intricate structures with exact spatial accuracy. Personalized skin grafts, tissue scaffolds, and wound dressings replicate natural tissue structure, facilitating cell adhesion, growth, and differentiation to improve wound healing results.
Intelligent Wound Bandages: Continuous Tracking for Accurate Treatment
Intelligent wound coverings featuring sensors and microelectronics provide immediate tracking of the healing process. Recognizing alterations in pH, temperature, moisture content, and biomarker levels allows for timely actions, enhancing treatment approaches and elevating patient care.
Immunomodulation: Harmonizing Inflammation and Regeneration
Immunomodulation aims to influence immune responses to enhance tissue regeneration while reducing inflammation and infection. Altering immune cells, cytokines, and signaling pathways establishes a pro-regenerative atmosphere, promoting wound healing and tissue restoration.
Extracellular Vesicles (EVs): Communication for Repair
Extracellular vesicles (EVs) are essential for cell communication and tissue repair. Rich in bioactive compounds, they influence cellular reactions, stimulate angiogenesis, and improve tissue repair, presenting opportunities as regenerative therapies for wound healing.
Sophisticated Imaging Methods: Improving Diagnosis and Surveillance
Sophisticated imaging methods like computed tomography (CT), magnetic resonance imaging (MRI), and optical coherence tomography (OCT) offer in-depth visualization of wound structure and healing processes. These non-invasive techniques provide information on tissue blood flow, oxygen levels, and cellular function, aiding in precise diagnosis, treatment strategy development, and tracking of wound healing.
Bioactive Compounds: Utilizing Nature's Medicinal Tools
Bioactive compounds, such as growth factors, cytokines, and extracellular matrix elements, are vital to the process of wound healing. Utilizing the regenerative capabilities of these molecules via targeted delivery systems like hydrogels, nanoparticles, and microparticles enhances tissue repair, angiogenesis, and remodeling activities.
Artificial Intelligence (AI) and Machine Learning: Forecasting Analytics for Ideal Care
AI and machine learning techniques evaluate extensive clinical data to forecast wound healing results, pinpoint risk factors, and enhance treatment approaches. Incorporating patient-specific elements, including demographics, comorbidities, and genetic information, AI-powered decision support systems facilitate tailored wound care management and enhance clinical results.
Regenerative Medicine: Tissue Engineering for Enduring Solutions
Regenerative medicine techniques, including tissue engineering and organoid culture, seek to repair injured tissues and organs by transplanting bioengineered constructs. Regenerative therapies provide lasting solutions for chronic wounds and tissue defects by merging cells, biomaterials, and growth factors in a biomimetic setting, signaling a new chapter in regenerative medicine.
Patient Involvement and Learning: Enabling Self-management and Prevention
Programs focused on patient engagement and education enable individuals to take an active role in managing and preventing their wound care. Healthcare providers enhance treatment plan adherence, minimize complications, and boost patient outcomes in acute and chronic wound situations by offering access to educational materials, self-care resources, and remote monitoring technologies.
Worldwide Cooperation and Access: Closing Gaps in Healthcare Inequities
Worldwide collaboration efforts seek to tackle inequalities in access to wound care and available resources. Collaborations among governments, non-profit entities, and industry participants enhance the wound care infrastructure, training, and technology distribution, thereby increasing access to quality care, especially in underserved areas and low-resource environments [6].
Wound Care APPROACHES:
Hydrogels as Contemporary Wound Dressings
Hydrogel treatments for wounds are truly contemporary wonders! They create a wet setting that promotes recovery, reduces discomfort, and could help with debridement. Additionally, they are adaptable enough to handle several types of injuries, ranging from persistent sores to burns. They are highly useful in wound care because of their capacity to absorb excess exudate and keep moisture in the wound bed.
Water-attracting polymers soaked in glycerine or water from the structure of hydrogel wound dressings. This framework provides them with a considerable amount of moisture, usually between 80% and 99%. This elevated moisture content enables them to produce a damp setting that replicates the body's natural method of healing.
Below is a detailed overview of their characteristics and advantages:
Moist Environment: A moist wound environment is created using hydrogel dressings, which is essential for boosting the body's inherent mechanisms for healing. This humidity supports cell movement, development, as well as tissue repair.
Debridement of the Wound: Certain hydrogel dressings have agents or enzymes that help scrub away debris and necrotic tissue from the wound bed. This aids in establishing a sterile wound environment that promotes healing.
Pain alleviation: The ability of hydrogel dressings to cool may assist in reducing soreness and unease related to wounds. For those who have burns or extremely sensitive wounds, this is especially helpful.
Exudate Management: Hydrogel dressings moisturize the wound bed while also removing excess exudate from the wound. This keeps the wound from being overly wet or too dry and helps maintain the ideal moisture balance.
Adaptability: Hydrogel dressings can be used in many ways and are appropriate for various kinds of wounds, including surgical wounds, diabetic ulcers, pressure sores, burns, and abrasions. They are simply cut and adapted to the shape of the wound, making them appropriate for various sizes and forms of wounds.
Non-Adherent: Hydrogel dressings do not adhere to the wound bed, reducing trauma and discomfort when changing dressings. This function additionally aids in safeguarding newly created tissue and encourages uninterrupted wound recovery.
Biocompatibility: Hydrogel dressings are typically accepted by the body and are appropriate for application on delicate or sensitive skin. They are unlikely to cause allergies and typically don't irritate the skin or provoke allergic reactions in the majority of people.
Ingenious Hydrogels as Advanced Wound Bandages
Comprehensive hydrogel applications have been broadened by research to include interesting substances that can affect each stage of the healing process in addition to protecting wounds. In 1949, Kunh et al., introduced the notion of smart in their study on three-dimensional networks made of polyacrylic acid which are able to absorb and simulate muscle contractions in acidic environments significant amounts of water in an acid environment when interacting with alkaline materials.
In the treatment of wounds, SHs offer significant advantages, including reduced healing duration and enhanced prevention of complications, resulting in improved outcomes and a higher well-being of patients.
Using physical or chemical gelation techniques, for the creation of SHs, natural and semisynthetic/synthetic polymers can be utilized with success. Chemical cross-linking methods include the widely utilized Schiff-base reactions, Michael addition reactions, free-radical polymerization of terminally functionalized macromers, high-energy radiation, and enzyme processes. Structures that are extremely stable are produced via chemical cross-linking, and the matrices' pore diameters, pore density, degree of cross-linking, and gelation length can all be altered. These techniques' primary disadvantage is the possibility of toxicity brought on by the byproducts of cross-linking processes. Furthermore, the cross-linkers may alter the hydrogel matrix's therapeutic goal by interacting with bioactive components (cells, active pharmacological proteins, such as growth factors, hormones, and enzymes).
Weak interactions including hydrogen bonds, van der Waals forces, ionic and hydrophobic contacts, crystallization, chain entanglements, coordination bonds, protein connections, and cycles of heating and cooling as well as freezing and thawing are all involved in physical cross-linking. The primary drawback of these techniques stems from the reversible nature of gelation under different conditions, which can be tailored for particular uses of the end product or, on the other hand, might cause stability challenges over time.
The purpose of multifunctional SHs are used in wound care to improve treatment and get beyond the limitations of conventional hydrogels effectiveness by leveraging their capacity to change their 3D structure reversibly when exposed to various external stimuli [7]. The cellulose derivative-based hydrogels as drug delivery systems to enhance drug bioavailability and treatment effectiveness are shown in table1.
Table1: An overview of studies on hydrogels made from cellulose derivatives as drug delivery mechanisms to improve drug bioavailability and treatment efficacy.
|
Cellulose Compounds |
Drug |
Treatment |
|
CMC (Critical Micelle Concentration) |
Diclofenac (NSAID) |
Cut and grazes |
|
HPMC (Hydroxypropyl methylcellulose) |
Etoricoxib (NSAID) |
Ongoing or sudden health condition |
|
HPC (Hydoxypropyl Cellulose) |
Lidocaine (local anesthesia) |
Encourage a systematic and regulated approach to medication |
|
HPMC (Hydroxypropyl methylcellulose) |
Mepivacaine (local anesthesia) |
Alleviate localized discomfort and execute a regulated medication distribution |
|
CMC (Critical Micelle Concentration) |
Berberine (natural anti-inflammatory) |
Safeguard postsurgical tissue and execute regulated drug delivery |
|
HPMC (Hydroxypropyl methylcellulose) |
Propanolol (non-selective beta-blocker) |
Enhance transdermal absorption |
|
HPMC (Hydroxypropyl methylcellulose) |
Propanolol (non-selective beta-blocker) |
Enhance medication discharge |
Scaffold:
Structures that are implanted rather than injected or polymerized in situ, as hydrogels might be, are referred to as ‘Scaffolds’. This usually does not pose a barrier to wound healing because most wounds are superficial and reasonably accessible for medical attention. Certainly, when better mechanical qualities or a longer deterioration period are required, a scaffold can be the best option. Their three-dimensional structural arrangement improves cell infiltration as well as facilitates the precise organization of stimuli to effectively direct tissue regeneration.
These sheets showed promise in a number of individuals with persistent wounds that don't heal, but a randomized controlled clinical trial is essential to fully evaluate the therapy's advantages.
An advanced dressing for wounds was developed using FGF-1-infused chitosan cross-linked collagen, demonstrating improved wound healing in rats with diabetes. Using a collagen-gelatine scaffold, FGF-2 was administered and evaluated in standard wounds, in addition to mice with diabetes that have pressure ulcers. In another investigation, the discharge of platelet lysate from the same scaffold was evaluated, which revealed that lysate levels had an effect on results of wound healing that was concentration-dependent. A collagen-chitosan sponge was used to produce a gene that activates bilayer dermal equivalent (BDE), which included plasmid DNA expressing VEGF, along with a mechanism of transmission of genes without the use of viruses. In both full-thickness excisional wounds and burn wounds in pigs, the BDE improved the vascular density and overall tensile strength of newly formed dermal tissue.
Particles:
Nano- and micro particles represent a thoroughly studied class of drug delivery systems that provide distinct benefits over scaffolds and hydrogels. For applications in using a tiny needle, particles can be introduced into the surrounding healthy tissue to aid in wound healing in order to avoid obstructing the wound bed's healing process. They can be modified via different parameters to achieve intricate release profiles that are inadequate for gels and scaffolds.
The most popular polymer for making particles with controlled release is poly (lactic-co-glycolic acid) (PLGA). One of the causes is the lactic acid generated when PLGA breaks down may actively promote angiogenesis and collagen formation to aid in the healing process [8].
The nanoparticles of PLGA were formulated to safeguard the curcumin's effectiveness and to deliver it gradually over a period of eight days. When tested on mice with excisional wounds that were fully splinted, the combined effects of lactate and curcumin encouraged the growth of granulation tissue and angiogenesis while reducing the inflammatory response. To administer EGF, similar nanoparticles were used, but at a significantly faster rate, with a duration of merely one day. However, when applied to diabetic rats excisional wounds, the treatment produced the most proliferating cells and, in contrast to free EGF solution, somewhat accelerated wound closure. Additionally, particles have been created to transport plasmids or genes. An instance is nanoparticles of biodegradable poly (β-amino esters) (PBAE) employed for the transport of plasmid Sonic, a morphogen known for its diverse contributions to tissue regeneration. There was an increase in several growth factors after the particles were injected intradermally close to the wound borders. An innovative approach utilizes nanoparticles composed of chitosan, silica, and PEG to efficiently deliver a gradual and consistent release of NO to wounds. NO is acknowledged for its functions in immune regulation and enhancing wound healing. The nanoparticles applied to the surface accelerated the healing process of wounds in mice, whether they were infected or uninfected. Moreover, they were contrasted with the typical NO-donor, Diethylene -triamine, showing better outcomes in a diabetic mouse wound model using immune deficiency, which is of great clinical importance. Nanoparticles do not have to be polymeric; indeed, lipids have the benefit of fast self-assembly without the use of organic solvents. A team created 2 forms, nanostructured lipid carriers (NLCs) and solid lipid nanoparticles (SLNs), for the transport of EGF. The NLCs' loading efficiency exceeded the effectiveness of SLNs, which are frequently used to enclose goods in a shell instead of confining it within a matrix.
Conjugates and Complexes:
The fourth category of delivery mechanisms consists of conjugates and complexes. Chemical bonds are usually used to form conjugates, although complexes are usually established through physical exchange. Both strategies aim to extract soluble medications in order to either help target and enhance their interactions with cellular receptors or preserve and prolong their half-life. In a simple conjugation scenario, FGF-1 was bonded to PEG to increase its structural and thermal stability within the body. In diabetic rat wounds, PEGylated FGF-1 closed four days ahead of free FGF-1 and seven days ahead of the control group. Additionally, complexes can be used to increase skin permeability, which is crucial for wounds with a protective scab, or to address deep tissue injury prior to the development of a pressure ulcer. Protamine, a cation-rich protein with a low molecular weight, was modified to bind to the N-terminus of EGF. In both healthy and diabetic mice, as well as in a mouse burn wound model, proteamine-EGF complexes were effective when full-thickness wounds are being healed and exhibited 11 times higher transdermal absorption than free EGF.
Coacervates:
Coacervates are a novel class of drug delivery technology that was created lately to control the release of small-molecule medications and proteins. Coacervates are nanoscale liquid droplets that are separated from their surroundings and kept together by hydrophobic forces. They demonstrate quick preparation through self-assembly as delivery vehicles without the need for organic solvents and have a significant loading capacity. Using a water-based solution for preparation is practical and eliminates the chances of organic solvent residues from traditional particle production or denaturation of proteins.
Coacervates have different mechanical characteristics than polymeric particles; they are soft and malleable, it makes them ideal for a wound setting in which they may remain without significantly obstructing the influx of cells. In tissue engineering applications, this versatile characteristic facilitates rapid adsorption and diffusion to encapsulate polymeric scaffolds and assist drug release. Despite being a relatively new technology, with only ten years of experimental proof, the benefits of various coacervate systems in comparison to traditional delivery techniques offer significant potential for their upcoming use.
A well-characterized, the elastin-like peptides (ELPs) make up the coacervate system. When these recombinant proteins transcend a settable transition temperature, they spontaneously coacervate because they mimic the hydrophobic areas of trophoblasts. ELPs and KGF were combined to create fusion proteins, which, at body temperature, formed coacervate particles via self-assembly. A diabetic mouse strain with insulin resistance was used to create a chronic wound model, and the fusion peptide significantly improved granulation and re-epithelialization.
An additional polycation: a heparin combination known as the coacervate system was developed especially for the regulated release of growth hormones that bind to heparin. Initially, Heparin has the growth factor connected to it, followed by the introduction of a synthetic poly-cation, leading to the rapid creation of liquid coacervate droplets through complexation dependent on charge. The proteolytic environment of the wound is protected from growth factor within the coacervate and interactions with the skin increase its bioactivity following the release of heparin sulfate proteoglycans. Using this coacervate, Heparin-binding epidermal growth factor (HB-EGF) release was maintained for at least 10 days with nearly zero-order release kinetics. Full-thickness excisional mouse wounds treated with the HB-EGF coacervate showed faster healing by increased granulation, re-epithelialization, keratinocyte proliferation, and angiogenesis.
CURRENTLY INNOVATIVE TECHNIQUES IN SKIN REJUVENATION AND WOUND HEALING:
Skin tissue engineering is an intricate process that entails the careful selection of biomaterials, choosing the right cells, and creating an appropriate platform that replicates both the skin's functional and structural properties.Over the past five years, research on wound healing and regeneration has placed a significant emphasis on creating a pro-regenerative framework. The primary goal is to create scaffolds that combine cells to successfully regenerate skin injury.
Immunomodulation and vascularization-focused strategy:
Key objectives in wound care focus on promoting vascularization inside the newly formed tissue to encourage quick skin regeneration and healing. Numerous innovative methods have employed cellular and the use of molecular biology in the last ten years to create pre-vascularized skin transplants. In recent years, researchers have focused on gaining a deeper understanding of fundamental biology while developing advanced cellular therapies.
SiRNA-focused skin treatments:
The use of siRNA and miRNA in nucleic acid-related wound healing techniques has grown in popularity recently. By destroying the messenger RNA (mRNA) associated with the target gene, certain genes can be specifically silenced by small interfering RNA, a short synthetic RNA of 21–25 nucleotides.
MicroRNA-based treatments for skin conditions:
If the significance of miRNAs is not taken into consideration, the discussion of nucleotide-based treatments for wound healing is inadequate. Despite the fact that siRNA and miRNA have similar structures (around 25 nucleotide RNA double strands with two nucleotides at the 3' end), their mechanisms of action differ. In contrast to siRNAs that are crafted with a focus on binding specificity, miRNAs are less precise regarding complementarity to their targets, allowing them to potentially affect multiple genes.
A progress report regarding the clinical trials:
For pre-clinical research on animal models and proof of concept to be validated, technology must be applied in clinical settings. Clinical research provides important information on treatment costs, patient safety, and possible hazards associated with a certain therapy, in addition to revealing treatment outcomes. Over time, controlled clinical trials involving patients in various clinical settings have routinely assessed the effectiveness of skin transplants and wound dressings [8].
SELECTIONS FOR WOUND HEALING MEDICATIONS:
Prevention
The majority of injuries result from accidents. Ensure your home is secure by eliminating items that could result in slips or tumbles, keep hot pots and knives away from the edges of counters and set the water heater to 120 degrees, and be cautious when handling knives. When you sustain carefully cleaning and treating a cut or injury, it may frequently prevent infection and associated issues.
Strategy for Treatment
The best conditions for wound healing are ones that are warm, humid, and clean. Certain injuries, like small cuts and abrasions, can be managed at home. Apply direct pressure to halt the bleeding and rinse the wound with water. Soap and hydrogen peroxide are not necessary. Use an antibiotic ointment, and then secure the injury with a sticking plaster. Replace the bandage daily, or whenever it becomes wet. If any redness spreading from the wound after two days, or notice yellow fluid draining from it, reach out to your doctor immediately.
Drug Therapies
The provider might recommend the subsequent medications:
Surgical and Other Procedures:
Serious injuries might require surgical intervention. This could entail excising charred tissue and eliminating infected tissue, applying skin grafts, and draining abscesses in injuries encircled through irritated tissue.
Alternative and Complementary Therapies:
1) Zinc: Zinc can be used topically as a lotion to hasten the healing process of wounds. Avoid using it on open wounds. If you use zinc over an extended period, consult your doctor about whether you should also take copper. Excessively high levels of zinc can dampen your immune response. Certain research has indicated that elevated amounts of zinc are associated with an increased likelihood of specific cancers.
2) B Complex Vitamins: Comprising B1 (thiamine) and B5 (pantothenate), might support skin health and assist in wound healing.
3) Bromelain: An enzyme derived from pineapple that has been shown in certain studies to decrease swelling after surgery, bruising, recovery time, and discomfort. Bromelain might increase the likelihood of haemorrhaging. If anyone taking anticoagulant medications such as warfarin (Coumadin) or taking aspirin, speak with a doctor before using bromelain. People allergic to pineapple ought to refrain from using bromelain.
4) Glucosamine and Chondroitin sulfate might assist in healing wounds by promoting the repair of bodily connective tissue, though further research is necessary for confirmation. Before using glucosamine, speak with a doctor if anyone has diabetes or asthma. Glucosamine and chondroitin may increase the risk of bleeding, especially if anyone is using blood thinners like clopidogrel (Plavix) or warfarin (Coumadin). Certain physicians believe the glucosamine could affect the effectiveness of some cancer treatment medications. It might also affect acetaminophen (Tylenol) and certain diabetes medications. Consult with a physician prior to using glucosamine along with chondroitin.
5) L-arginine has been used to speed up the healing process after surgery. It has also been applied to the skin to help the healing of wounds. Exercise care, if anyone is susceptible to herpes outbreaks, consult with a physician for guidance. If anyone suffers from asthma, before using arginine, speak with a doctor if using Viagra or blood pressure medicine.
6) Honey has been used as a skin dressing following surgery, and several studies show, it aids in wound healing while preventing infection. It is intended for use on small injuries only. Consult with a doctor prior to applying honey to small injuries, and avoid putting honey on an open wound.
HERBS:
Some plant-based remedies might provide symptom relief and promote quicker wound healing. Herbs are generally found in the form of dried extracts (capsules, tablets, or pills), teas, or tinctures (unless specified differently, alcohol-based extraction). Individuals with a background of alcohol dependency ought to stay away from tinctures. The recommended amount for teas is using 1 generous teaspoon for each cup of water, steeping for 10 minutes, whereas roots require 20 minutes unless stated otherwise.
Put onto the skin:
Avoid applying using herbs to open wounds without the guidance of a doctor.
1. Aloe (Aloe vera), in the form of cream or gel. Aloe has historically been applied for minor injuries and burns, yet scientific research on its efficacy shows varying results. In a study, aloe appeared to prolong the duration required for the healing of surgical wounds.
2. Calendula (Calendula officinalis), commonly known as marigold pot, employed as a topical ointment or infusion. To prepare tea with a tincture, mix 1/2 to 1 tsp. in 1/4 cup of water. Take steep 1 tsp. of blossoms in a cup of boiling water for 15 minutes, then strain it and let it cool. Conduct a preliminary skin test to check for potential allergic responses.
3. Marshmallow (Althaea officinalis) is employed in the form of a localized cream to enhance wound recovery and address swelling.
4. Tea tree oil (Melaleuca alternifolia) in liquid and buttery consistency. Use twice daily to minimize inflammation. Avoid using tea tree oil for burn treatment.
5. Gotu kola (Centella asiatica) in a cream formulation containing 1% of the plant, promotes wound healing.
6. Chamomile (Matricaria recutita or Chamaemelum nobile), applied as an ointment or cream, promotes the healing of wounds.
7. Sesame oil (Sesamum indicum L.) facilitates wound healing through its antioxidant, anti-inflammatory, and antimicrobial properties that aid in tissue repair. According to existing preclinical studies, sesame oil at around 30–40% might be the most effective for enhancing wound healing when applied topically in an ointment or preparation.
8. Echinacea or coneflower (Echinacea spp.) in the shape of a gel or cream containing 15% of the plant's extract.
9. Slippery elm bark (Ulmus rubra or fulva) as a compress, combine 1 teaspoon of the dried powder with a cup of boiling water. Unwind and use a gentle, fresh substance. Apply to the impacted region [9, 10] .The different Wound Healing properties with medicinal herbs and oils are shown in table 2.
Table 2: Medicinal Herbs and Oils with Wound Healing Properties.
|
Sr. No. |
Herb |
Scientific Name |
Key Properties |
References |
|
1 |
Aloe |
Aloe vera |
Used in scar- reduction creams due to high Vitamin E content. |
[20] |
|
2 |
Lavender |
Lavandula angustifolia |
Essential oil is antiseptic; applied topically to stimulate skin repair. |
[16] |
|
3 |
Tea Tree |
Melaleuca spp. |
Essential oil has antiseptic and anti-inflammatory properties. |
[15] |
|
4 |
Mallow |
Althaea officinalis |
Flowers and crushed leaves useful for facial scarring and acne. |
[13] |
|
5 |
Pineapple |
Ananas comosus |
Contains bromelain (anti-inflammatory); best combined with turmeric. |
[18] |
|
6 |
Echinacea |
Echinacea purpurea/ spp. |
Prevents wound infection; gels/creams may contain 15% extract. |
[14] |
|
7 |
Chamomile |
Matricaria recutita or Chamaemelum nobile |
Used as a cream/ ointment; promotes healing of wounds. |
[17] |
|
8 |
Sesame Oil |
Sesamum indicum L. |
Facilitates wound healing via antioxidant, anti-inflammatory and antimicrobial properties. |
[19] |
|
9 |
Slippery Elm Bark |
Ulmus rubra or Ulmus fulva |
Used as a compress; dried powder mixed with hot water and applied to the affected area for wound relief. |
[10,21] |
CONCLUSION
Wound healing is a complex process that includes precisely coordinated and timed reactions to skin injury. Alterations in any of these phases can result in chronic wounds and may impede the healing process. Recognizing and improving modifiable risk factors is essential in wound care. The occurrence of acute and chronic wounds rises annually due to the elderly population and the rising prevalence of wound-associated comorbidities, posing an ongoing challenge for healthcare systems globally. Over time, medical experts have created and utilized different protocols and instruments to tackle misunderstandings in evaluating wounds, resulting in slower healing and additional issues. The formation of new tissue and wound closure are the final phases of wound healing, and the following remodeling stages.
There are several biomaterial-based delivery strategies for genes, proteins, and small molecule medications involved in wound healing. In a variety of in vivo models, hydrogels, scaffolds, particles, complexes, and coacervates have all demonstrated efficacy; each may be appropriate for a particular use or situation. The process of wound healing is quite complex, which makes it crucial to understand the reasons behind each type of wound and to develop correspondingly sophisticated delivery systems for personalized treatment. To achieve this aim, it is essential to integrate various biomaterials to create composite systems that can release multiple factors with accurate kinetics [11, 12].
REFERENCES

Pragati Kumari, Sunil Jawla, Seema Rohilla, Daisy Arora, Emerging Therapeutic Approaches for Effective Wound Healing Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1299-1317. https://doi.org/10.5281/zenodo.18547423
 10.5281/zenodo.18547423
10.5281/zenodo.18547423