1Master in Physiotherapy (Neurology), Combined (P.G) Institute of Medical Sciences & research (CIMSR), Harrawala, Dehradun, Uttarakhand-248160 (India).
2Assistant Professor, Faculty of Pharmacy, Maharaja Agrasen Himalayan Garhwal University, Pokhra, Pauri Garhwal-246169, Uttarakhand (India).
Study Design-A systematic review with meta-analysis. Objective-This study aims to conduct a systematic review and meta-analysis to evaluate the effectiveness of rehabilitation following lumbar fusion surgery (LFS). Background-LFS is increasingly performed for the management of lower back pain, with or without neurogenic leg pain, particularly as the population ages. However, clinical outcomes often lag behind surgical outcomes, and approximately 40% of patients continue to experience significant back-related disability 12 months after surgery. Identifying effective rehabilitation strategies to enhance function and quality of life post-LFS is crucial. Methods-A systematic review was conducted using multiple databases, including MEDLINE, CINAHL, and grey literature sources. Studies were screened for inclusion based on title and abstract, followed by full-text evaluation against predefined eligibility criteria. Included studies underwent critical appraisal and risk of bias assessment. The GRADE approach was used to assess the quality of evidence. A meta-analysis compared "complex rehabilitation" (combining exercise and cognitive behavioral therapy) with usual care, evaluating outcomes related to pain, disability, fear of movement, and mental health at both short-term (<3>12 months) follow-up. Results-Three studies were included in the systematic review, with two eligible for meta-analysis (total participants: 237; female: 62%; mean age: 55 years). Low-quality evidence suggests that "complex rehabilitation" provides short-term improvements in disability (effect size: -0.85, 95% CI: -1.41 to -0.29) and fear-avoidance behavior (-1.07, 95% CI: -1.33 to -0.80) compared to usual care. Similarly, low-quality evidence supports the benefits of "complex rehabilitation" for long-term disability (-0.84, 95% CI: -1.11 to -0.58) and fear-avoidance behavior (-1.40, 95% CI: -1.69 to -1.12)Conclusion-Although limited by the small number of low-quality studies, findings suggest that "complex rehabilitation" may reduce both short- and long-term disability and fear-avoidance behaviour following LFS. However, further high-quality research is needed to confirm the effectiveness of such rehabilitation programs.
Lumbar fusion surgery (LFS) is performed to stabilize adjacent vertebral motion segments rigidly. It is often combined with surgical decompression to relieve back pain and/or neurogenic leg symptoms. ¹?³ Common indications for LFS include spondylolisthesis, disc disease, and spinal stenosis.1 In the UK, the incidence of LFS is rising. In 2009/2010, 4,036 procedures were performed, increasing by over 60% to 6,547 in 2012/2013. A similar trend is observed in the USA, particularly among patients over 60 years of age. As projections estimate that 30% of the UK population will be over 60 by 2037,? the demand for LFS is expected to continue increasing.2 Despite undergoing LFS, many patients experience persistent symptoms. Data from the Swedish National Spine Register indicate that 25% of patients report unchanged or worsening pain, while 40% remain uncertain or dissatisfied with their outcomes 12 months post-surgery. This underscores the need to explore strategies for improving postoperative recovery.3 A recent Cochrane Back Review Group (CBRG) report suggests that rehabilitation, particularly supervised active exercise, improves pain relief and functional outcomes following laminectomy for lumbar stenosis. However, its effectiveness for LFS remains unclear, with no established consensus on postoperative rehabilitation protocols.4,5 A previous systematic review and meta-analysis found inconclusive and very low-quality evidence regarding the benefits of physiotherapy-including exercise, manual therapy, electrotherapy, and cognitive behavioral therapy (CBT)-following LFS. The study emphasized the urgent need for further research in this area.
Objectives
This review aimed to evaluate the evidence on rehabilitation strategies for adults following lumbar fusion surgery (LFS) for degenerative conditions. Eligible trials included randomized controlled designs, an appropriate comparator (e.g., usual care), and validated outcome measures assessing pain and/or disability in both the short term (<6 months) and long term (>12 months).
MATERIALS AND METHODS
Protocol and Registration
A protocol was developed based on the methods described by the Cochrane Back Review Group (CBRG) and the Cochrane Handbook. The study followed PRISMA guidelines6 and was registered with the International Prospective Register of Systematic Reviews (PROSPERO).
Eligibility Criteria
Studies investigating rehabilitation following LFS that met the following criteria were included in the review:
Search Strategy
A three-phase search strategy was employed:
Information Sources
The following databases were searched:
Study Selection
Two independent reviewers (J.G., J.M.) conducted database searches, saved and pooled results, removed duplicates, and integrated findings from grey literature and hand searches.
Disagreements and Consensus Resolution
Disagreements between authors were resolved through a third-party mediator (A.M.) to ensure consensus.
Data Extraction
A data extraction form, based on the "Characteristics of Included Studies" table from the Cochrane Handbook,7 was developed in parallel with the search strategy and adapted to suit the needs of this review. Two independent reviewers (J.G., J.M.) performed data extraction, while a third reviewer (M.H.) verified the form against selected studies to ensure accuracy. Authors of the included studies were contacted for raw data, which was successfully obtained from one study.8
Extracted Data Items
The extracted data included study design, participant characteristics (including surgical indications), intervention details, comparators, and both primary and secondary outcome measures. These outcomes were assessed at short-term and long-term follow-ups and covered aspects such as disability, pain, mental health, and fear-avoidance behavior. No assumptions or data simplifications were made.
Summary Measures and Data Synthesis
The review protocol allowed only for the inclusion of studies with comparable participants, interventions, comparators, and outcome measures. Short-term and long-term outcomes for disability, pain, mental health, and fear-avoidance behavior were identified as suitable for pooled analysis. A meta-analysis was conducted using RevMan9 software, applying the inverse variance model for continuous data (change in mean values from baseline). The DerSimonian and Laird10 random-effects model was used to account for variations across studies while assuming related intervention effects.
Risk of Bias Assessment
Within Individual Studies
The Cochrane Risk of Bias Assessment Tool was used to evaluate internal validity and potential sources of systematic error.
Across Studies
A formal risk-of-bias assessment across studies was not conducted due to the limited number of studies. Funnel plots were deemed unnecessary. The GRADE13 criteria were used to assess the quality of evidence.
Additional Analyses
Due to the small number of studies, additional analyses were not feasible.
RESULTS
Study Selection Process
Database searches were conducted on October 13 and October 20, 2014, by J.G. and J.M., respectively. This process identified 1,006 studies, which were screened by title, leading to the removal of 972 irrelevant or duplicate papers. The remaining 34 abstracts were retrieved and reviewed by J.G. and J.M., resulting in 12 papers classified as eligible or potentially eligible for full-text review. The inter-reviewer reliability was strong (Cohen’s k = 0.78). After full-text review, five papers reporting data from three original studies met the inclusion criteria. The agreement between authors was very strong (Cohen’s k = 0.88). (See Figure 1 for study selection flowchart).
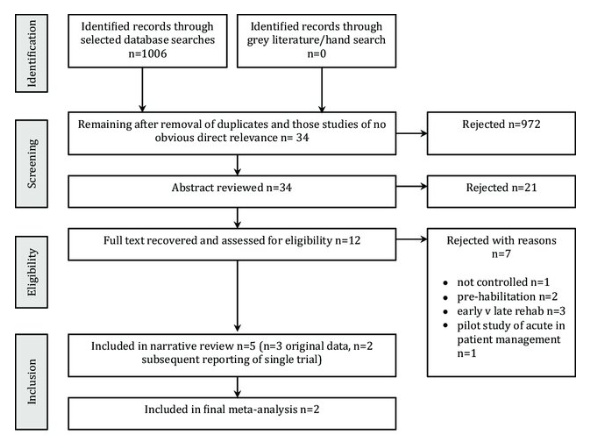
Figure 1. A Flowchart Depicting the Study Selection Process Along with Reasons For Rejection
Introduction
Three papers met the eligibility criteria for inclusion in this review.¹4 All three studies compared usual care with innovative forms of rehabilitation. Christensen et al.15 compared usual care with a "back café" group and a physical training group, Abbott et al.16 with "psychomotor therapy," and Monticone et al.¹? with a combination of exercise and cognitive behavioral therapy (CBT). Rehabilitation sessions lasted 60 minutes, twice per week, for four weeks. Rehabilitation commenced after LFS; however, the exact timing was not well described. The primary outcome measured was post-rehabilitation change in the Oswestry Disability Index (ODI) score. Secondary outcomes included the Tampa Scale of Kinesiophobia (TSK), pain levels (Numerical Rating Scale - NRS), and quality of life (QoL), including mental health (SF-36). Outcomes were recorded pre-treatment, immediately post-rehabilitation, and 12 months after LFS.
Study Details
This study included 90 participants (mean age: 45 years) randomized into three intervention groups:
No primary outcome measure was explicitly identified, but the Low Back Pain Rating (LBPR) Scale²³ was used for evaluations at 3, 6, 12, and 24 months post-LFS.
This study randomized 107 participants (mean age: 51 years) into two groups:
This rehabilitation approach, combining physical therapy (based on Richardson and Hides²?) and CBT (based on Linton²?), was termed "psychomotor therapy". Rehabilitation began within three weeks of discharge following LFS. The primary outcome measure was the Oswestry Disability Index (ODI), assessed at 3, 6, 12, and 24–36 months post-LFS. Secondary outcomes included:
This study randomized 130 participants (mean age: 57 years) into two groups:
Risk of Bias Assessment
Inter-reviewer agreement on risk-of-bias assessment was good (Cohen’s k = 0.72).
Synthesis of Results
For the purpose of this review, the combined approach of exercise + CBT was termed "complex rehabilitation." Data from both studies were pooled to compare complex rehabilitation versus usual care across comparable outcomes.
Consensus among review authors led to pooling data for:
Pooled Results from Abbott et al.16 and Monticone et al.17
Key Findings
Meta-Analysis Results
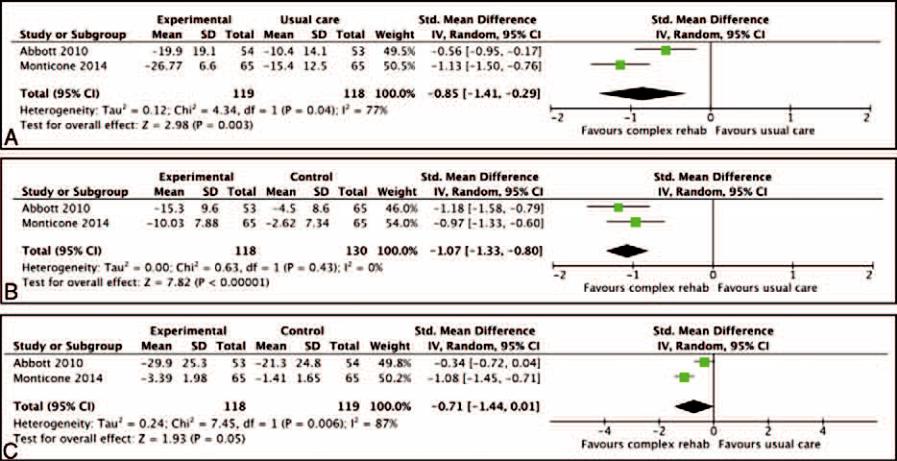
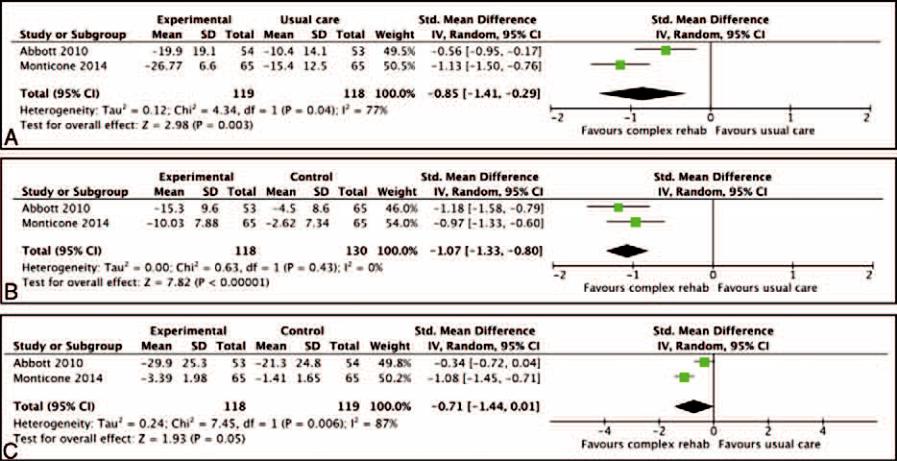
Pooled data from Abbott et al.16 and Monticone et al.17 indicated significant short-term effects favoring complex rehabilitation:
These findings suggest that complex rehabilitation (exercise + CBT) significantly improves disability and fear-avoidance behavior compared to usual care.
Pooled Analysis and Heterogeneity
The pooled analysis for short-term low back pain (LBP) narrowly failed to reach statistical significance (0.71, 95% CI: -1.44 to 0.01). Heterogeneity (I²) was high in the pooled analysis for disability (77%) and LBP (87%), which may have contributed to the lack of observed effect. In contrast, heterogeneity for fear-avoidance behavior was low (0%). In the long term (12 months), one study reported significant improvements in disability and fear-avoidance behavior, while another study found significant improvements in disability, pain (both back and leg), fear-avoidance behavior, and mental health. In all cases, the results favored "complex rehabilitation." Pooled analysis demonstrated statistically significant effects for disability (effect size: 0.84, 95% CI: -1.11 to -0.58) and fear-avoidance behavior (-1.40, 95% CI: -1.69 to -1.12), both in favor of "complex rehabilitation." Heterogeneity was within acceptable limits for both meta-analyses. However, the long-term meta-analysis for LBP did not support any positive effect of "complex rehabilitation" over usual care.
Risk of Bias Across Studies
Two studies were included in the meta-analysis.18,19 Both had one high-risk domain related to blinding participants, while one study also had an unclear risk of bias concerning blinding of outcome assessment. Overall, the majority of data comes from studies with a low or unclear risk of bias, making the overall risk of bias across studies uncertain (Fig. 2).

Figure 2. Summary Table of Risk of Bias. R (Green) Indicates A Low Risk of Bias, - (Red) Indicates A High Risk of Bias, And? (Yellow) Indicates an Unclear Risk of Bias.
DISCUSSION
Summary of Evidence
Findings from this systematic review and meta-analysis suggest that patients undergoing "complex rehabilitation" experience lower levels of self-reported disability and reduced fear-avoidance behavior compared to those receiving usual care for up to 12 months following LFS. This suggests that the current standard of usual care may contribute to some patients’ dissatisfaction with LFS outcomes. These results contrast with a previous review that found no significant effect of physiotherapy following LFS. This discrepancy is likely due to the exclusion of the study by Christensen et al. and the inclusion of a more recent study by Monticone et al17. The broader study selection in this review allowed for a wider comparison and increased the sample size in pooled analyses. A minimally important clinical difference in the Oswestry Disability Index (ODI) has been estimated at 12.4%. Both Abbott et al16. and Monticone et al17. demonstrated that "complex rehabilitation" can lead to a clinically meaningful reduction in disability in both the short and long term. Monticone et al. reported the largest reduction in disability (ODI), potentially due to the more intensive nature of the intervention in the "experimental group." However, dose-response relationships in pain rehabilitation programs for chronic LBP remain a topic of debate. Additionally, the specialized, multi-professional rehabilitation center setting may have contributed to the greater effect size observed.
Limitations
The primary limitation of this review is the limited number of studies available for inclusion in the meta-analyses. The strength of evidence, assessed using the GRADE framework, was classified as low, indicating that further research is highly likely to impact the estimated effect sizes. Findings from the meta-analysis should also be interpreted in light of potential risks of bias, which remain unclear across the two included studies. This is an important consideration for both service users and healthcare providers. Another limitation is the variability in both the "usual care" and "complex rehabilitation" interventions across studies. Although both included a cognitive behavioral therapy (CBT) component alongside exercise therapy, the intensity of "complex rehabilitation" varied significantly. Monticone et al17. reported a maximum of 38 hours of intervention, whereas Abbott et al. provided only 4.8 hours. Similarly, the composition of usual care differed across studies. Abbott et al. and Christensen et al. primarily utilized self-directed home exercise programs following a single physiotherapy consultation. In contrast, Monticone et al17. included up to 30 hours of supervised exercise over one month. These variations likely contributed to the heterogeneity observed and the lack of significant effects in some comparisons.

CONCLUSION
"Complex rehabilitation," which integrates exercise and cognitive behavioral therapy (CBT), provides both short- and long-term functional benefits for patients following LFS. However, high-quality research in this area remains limited. To ensure that LFS continues to be a viable treatment option, further research is essential to better understand patients' postoperative needs and identify optimal rehabilitation strategies. Future research should prioritize higher methodological quality, with clearer reporting on key factors such as patient compliance an issue that has been problematic in similar studies. Mixed-method evaluation, now considered the gold standard in clinical research, should be employed alongside robust economic assessments to evaluate cost-effectiveness. Additionally, recent guidelines on process evaluation for complex interventions should be taken into account. Studies should explore the underlying mechanisms of rehabilitation interventions and identify the "active" components driving their effectiveness. This review demonstrates significant and meaningful improvements in physical function and fear-avoidance behavior, independent of pain. However, it remains unclear whether these benefits stem primarily from enhanced physical conditioning, psychological improvements, or a combination of both. Further research is needed in this area, and at least one protocol and one study published since this review was conducted have contributed to expanding the evidence base.
REFERENCES


Mohit Saklani, Saurabh Saklani, Evaluating Rehabilitation Outcomes After Lumbar Fusion Surgery: A Systematic Review and Meta-Analysis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 31-41 https://doi.org/10.5281/zenodo.15315516
 10.5281/zenodo.15315516
10.5281/zenodo.15315516
