Dr. Kolpe Institute of Pharmacy, Kolpewadi, Tal- Kopargaon, Dist- A. Nagar
Mouth-dissolving films (MDFs) are an innovative drug delivery system designed to disintegrate rapidly in the oral cavity without water, offering a convenient alternative to traditional oral dosage forms. They enhance bioavailability by bypassing the gastrointestinal tract and first-pass metabolism, making them ideal for pediatric, geriatric, and dysphagic patients. MDFs provide quick drug action, ease of administration, and cost-effective production, with applications across various therapeutic areas. This study focused on the formulation and evaluation of a captopril-based MDFs, which demonstrated rapid disintegration, robust mechanical properties, and efficient drug release. The results confirm its suitability for populations with swallowing difficulties, supporting improved compliance and therapeutic outcomes. This study aimed to formulate and evaluate captopril-loaded mouth dissolving films (MDFs) for rapid antihypertensive action. Films were prepared using the solvent casting method with HPMC as the film-forming polymer and PEG-400 as the plasticizer. The formulations were assessed for physical characteristics, disintegration time, drug content, and in vitro drug release. The optimized film showed rapid disintegration (under 30 seconds) and over 90% drug release within 5 minutes, indicating its potential for fast onset of action. The results suggest that captopril MDFs are a promising approach for immediate blood pressure control with improved patient compliance.
Oral route of drug administration is a most preferred route. Due to its ease of administration, non-invasiveness, Adaptability, patient compliance and acceptability. Many alternatives to the oral route of drug delivery have consistently been introduced employing new and innovative technology for nauseated patients, elderly patients, and children. And patients who do not comply. Technological advancements have led to the introduction of bio adhesive mucosal dosage forms, such as adhesive tablets, gels, and patches. The use of polymeric films to deliver medication into the buccal cavity has shown a lot of promise among different dose forms in the recent past, when applied on the tongue, oral disintegrating films (ODFs) instantly hydrate by absorbing saliva after dissolving and/or disintegrating, releasing active ingredients. Medication from the dose container, ODFs are a type of formulation that is frequently made using hydrophilic polymers that allow for quick dissolving upon Coming into touch with saliva. The most common types of oral disintegrating drug delivery methods are oral disintegrating tablets (ODTs) and oral disintegrating films (ODFs). The most common types of oral disintegrating drug delivery methods are oral disintegrating tablets (ODTs) and oral disintegrating films (ODFs). These systems were created in late 1970 as a substitute for traditional dosage forms, such as rapidly dissolving Capsules and pills for children and elderly patients having trouble swallowing standard dose forms. An ODF is the size of a postage stamp. When ODF as introduced to the market, it was highly connected to patient counselling regarding the proper Administration by providing guidance such as “do not chew/do not swallow. However, in spite of these instructions, incidents regarding chewing and swallowing were often reported. But ODFs untied the masses from these adverse events. Mouth Dissolving Films (MDFs) is an innovative and impressive drug delivery system which increases patient compliance. MDFs deliver the drug systematically via sublingual or buccal route of administration and additionally for local action1. MDFs constitute a thin film which when positioned on the tongue gets wet by saliva and moistens rapidly and then film dissolves and disintegrates within seconds to supply the drug for absorption. When compared to capsules and different dosage forms, MDFs are advantageous because film dissolves within seconds and shows onset of action. MDFs increases bioavailability, shortens the onset of time, prevents first pass metabolism. Fast dissolving drug delivery is the maximum advanced form as it improves efficacy of drug, flexibility, disintegration and dissolution. Special future of mouth dissolving Films:
Advantages
Fast dissolving oral Films being an advanced evolution of fast dissolving drug delivery systems have some outstanding advantages over conventional dosage form and orally disintegrating tablets they are.
Disadvantages
1.2 Biopharmaceutical Classification System
The Biopharmaceutics Classification System or BCS is a system which classifies bioactive molecules based on solubility and permeability which is widely used to guide new drug development and drug formulation, as well as predict pharmacokinetics under prescribed conditions. Established by Gordon Amidon etc. All the original purpose of the system was to aid in the regulation of post-approval changes and generics, providing approvals based solely on in vitro data when appropriate. Importantly, since the majority of drugs are orally dosed, the system was designed around oral drug delivery via passive diffusion process through the small intestine where major extent of oral absorption is largely influenced by drug’s membrane permeability and solubility. Currently it is used to predict the bioavailability of the drug, used in in-vivo & in vitro correlations and bioavailability studies.
Table No.1: Biopharmaceutical Classification system
|
Class |
Permeability |
Solubility |
|
I |
High |
High |
|
Ii |
High |
Low |
|
Iii |
Low |
High |
|
Iv |
Low |
Low |
According to the Biopharmaceutical Classification System (BCS) drug substances/APIs are classified to four classes Upon Their High/Low Solubility and Permeability:
Class I Drugs
The drugs belonging to BCS class 1 are highly soluble and highly permeable, so they can be formulated as a suitable conventional dosage forms. Well absorbed orally. They exhibit a high absorption number and a high dissolution number they do not have solubility nor permeability limitation therefore they generally represent a low risk group of compounds in terms of the potential for excipients to affect absorption, compared to other BCS classes
? Example: Captopril, Metoprolol, Paracetamol
These compounds are well absorbed, and their absorption rate is usually higher than excretion.
Mouth-Dissolving Film’s Composition
To prepare Mouth Dissolving Film we need, API which should be in concentration range between 1-25%, Plasticizer in concentration range between 0-20%, flavoring agent in concentration between 2-10%, Sweetening agents in concentration between 3-6%, hydrophilic polymer/film former in concentration between 40-50%, saliva stimulation agent in concentration between 2-6%, colour 01%, surface active agent used as Quantity sufficient.
Hydrophilic Polymer/Film Former
The breakdown time of a movie is greatly influenced by the properties of polymers. Hydroxypropyl Methylcellulose, methylcellulose, pullulan, carboxymethyl cellulose, polyvinylpyrrolidone, etc. are a few Examples of frequently used water-soluble polymers/film formers. Polymerized resin is one example of a Novel film-forming substance
Plasticizer
This stops the membrane from rupturing. It must get along with the other ingredients. Several excipients, including castor oil, phthalates, polyethylene glycol, and phthalates.
Sweetening Agent
Mouth-melting films need to taste good in order to be accepted and appreciated by patients because they must be consumed dry and without water in order to dissolve and disintegrate in the oral cavity. Sucrose, Fructose, aspartame, sorbitol, acesulfame-K, and sucralose are some examples of sweeteners.
Saliva Stimulating Agent
These are helpful in increasing saliva production in the mouth, which promotes quick breakdown. Acids like Tartaric, lactic, malic, ascorbic, and citric are used as examples.
Flavouring Agent
Common Flavors include citrus, vanilla, coffee, cocoa, and chocolate.
Surfactant
They function as wetting, dispersing, or dissolving agents. Poloxamer, sodium lauryl sulfate, and minor are a Few examples. Surfactants are used to make poorly soluble medications more soluble as well as to Moisten, disperse, and solubilize the membrane and make it easier to release the active ingredients Benzethonium chloride and cadence are other few examples.
AIM AND OBJECTIVES:
To develop a novel drug delivery system in the form of mouth-dissolving films (MDFs) that enhances patient compliance by providing a convenient, fast-dissolving, and effective alternative to conventional dosage forms such as tablets and capsules.
Provide an alternative for individuals who have difficulty swallowing pills (e.g., pediatric, geriatric, and dysphagic patients).
Ensure fast onset of action by delivering the drug through the oral mucosa, bypassing the gastrointestinal tract and first-pass metabolism.
Offer a non-invasive, easy-to-use system without the need for water or additional aids, making it suitable for on-the-go use.
Increase drug bioavailability by leveraging absorption through the buccal or sublingual route.
Achieve effective therapeutic outcomes with potentially lower doses due to enhanced bioavailability and rapid onset.
Develop formulations that are simple to manufacture, scalable, and cost-effective for mass production.
Adapt the formulation to accommodate drugs with different solubility profiles and improve stability.
Reduce systemic side effects by targeting local or systemic delivery through controlled drug release.
METHODS OF PREPARATION:
1. Solvent casting method:
It is very old film making method. This technique involves dissolving or suspending the medication in a solution that contains plasticisers, polymers, and other excipients dissolved in a volatile solvent, such as water or ethanol. Known as “film dope,” it is subsequently cast in a petri plate and dried in an oven or other drying apparatus to eliminate all volatile solvents. After drying, the film is die-cut into strips and placed within airtight pouches. Because the temperature required to remove the volatile solvents is lower than with the hot melt extrusion approach, this technique works well for films that include heat-sensitive drugs or API.
Benefits
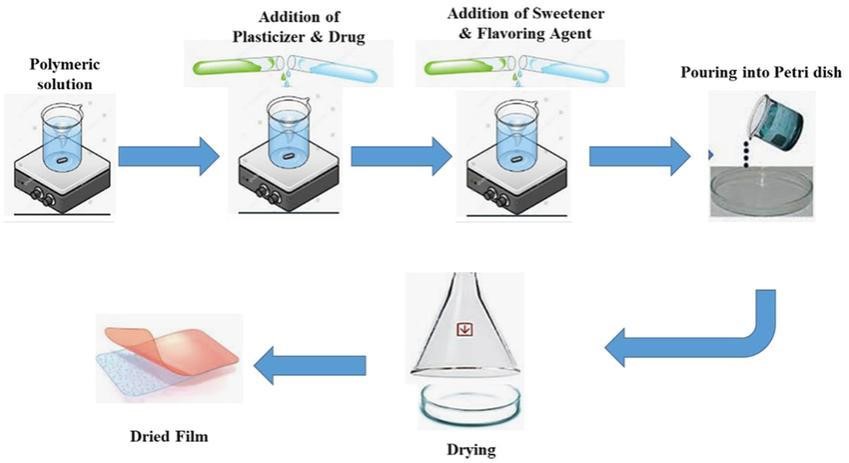
Figure No.01: solvent casting method
Experimental Section:
Drug profile: Captopril
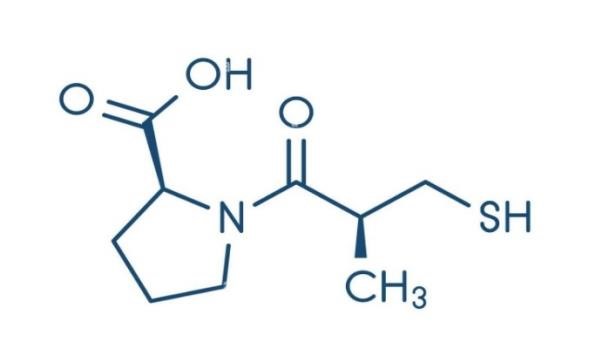
Figure no 2: structure of captopril
Molecular formula: C9H15NO3
Chemical Name: (2S)-1-[(2S)-2-methyl-3-sulfanylpropanoyl] pyrrolidine-2-carboxylic acid.
Drug class: Captopril is in a class of medications called angiotensin-converting enzyme (ACE) inhibitors. It decreases certain chemicals that tighten the blood vessels, so blood flows more smoothly and the heart can pump blood more efficiently.

Figure N0 3: Api Of Captopril
Solubility: Captopril is highly soluble in water (around 160 mg/mL) and other solvents like methanol and ethanol, but sparingly soluble in chloroform and ethyl acetate.
Mechanism of Action: Like all other ACE inhibitors, captopril blocks conversion of angiotensin I to the potent vasoconstrictor angiotensin II and inactivates simultaneously the vasodilator peptide bradykinin. Besides its blood pressure-lowering properties, captopril has various immunomodulatory functions.
Indications:
FDA-Approved Indications
Initial therapy for patients with normal renal function.
In patients with impaired renal function, captopril should be reserved for those patients who have developed unacceptable side effects or failed to respond to other drug therapy. Effective alone and in combination with other antihypertensive agents.
According to AHA/ACC/HFSA 2022 guidelines, captopril is indicated for managing HFREF (heart failure with reduced ejection fraction). ACE inhibitors, including captopril, are included in goaldirected medical therapy (GDMT), with an established reduced risk of rehospitalization and improved survival.
Captopril improves survival following myocardial infarction in clinically stable patients with a left ventricular ejection fraction of less than 40% and reduces the incidence of hospitalization. Captopril prevents remodelling and reduces cardiovascular mortality in patients with heart failure.
• Diabetic Nephropathy
Diabetic nephropathy is the leading cause of end-stage kidney disease (ESKD) in developed countries. This condition is due to microvascular complications of diabetes and can occur in type 1 and type 2 diabetes. Early treatment can prevent or slow the onset of diabetic nephropathy.
Root of Administration:
Adult Dosage
Captopril should be taken 1 hour before meals. Therapy initiation requires analysis of recent antihypertensive drug treatment, the extent of blood pressure elevation, and salt restriction. If possible, the previous antihypertensive drug regimen should be stopped 1 week before starting captopril. The daily dose of captopril may be increased every 24 hours under continuous medical supervision. The initial daily dosage should be reduced for patients with significant renal impairment, and smaller increments should be utilized for titration.
Initial dosage: 25 mg, 2 times or 3 times per day Unsatisfactory reduction of blood pressure after 1 to 2 weeks: Increase the dosage to 50 mg, 2 or 3 times daily. The dosage of captopril may increase to 100 mg, 2 or 3 times daily, and to 150 mg, 2 or 3 times daily, if further blood pressure reduction is required. The usual dosage range is 25 to 150 mg, 2 or 3 times daily. The maximum daily dose should not exceed 450 mg.
The initial dosage in patients vigorously treated with diuretics, hyponatremic, and hypovolemic patients is 6.25 or 12.5 mg, 3 times daily with titration to the usual daily dosage within several days. According to AHA/ACC/HFSA guidelines, the initial dosage in patients is 6.25 mg, 3 times daily, and the target dosage is 50 mg, 3 times daily. After a dosage of 50 mg, 3 times daily, further increases in dosage should be delayed for at least 2 weeks.
After a single dose of 6.25 mg, captopril therapy should be initiated at 12.5 mg, 3 times daily, and then increased to 25 mg, 3 times daily, over several days. Long-term use: target maintenance dose of 50 mg, 3 times daily. Therapy can be initiated as early as 3 days following myocardial infarction.
Long-term use: 25 mg, 3 times daily
Dosed orally or sublingually: 25 mg. Alternative therapy should be considered if blood pressure is nonresponsive within 20 to 30 minutes.
The initial dosage is 12.5 mg, 2 times daily; it can gradually increase to 25 mg, 3 times daily. The starting dosage may gradually increase to 25 mg, 3 times daily. Neutropenia is a common adverse event with captopril administration in patients with the Raynaud phenomenon.
Pharmacokinetics:
Absorption: Captopril is well-absorbed orally, with peak plasma concentration achieved within approximately 1 hour of administration. Food decreases the bioavailability of captopril; captopril should be administered 1 hour before meals.
Distribution: The volume of distribution is 0.8 L/kg. Plasma protein binding is approximately 25% to 30%. Captopril can cross the blood-brain barrier.
Metabolism: Captopril is metabolized to cysteine-captopril disulfide and captopril dimer disulfide.
Elimination: The kidney is the major route of elimination of captopril. The clearance is 0.7 L/h/kg, and the elimination half-life is approximately 2 hours; thrice daily administration is required. The clearance of captopril (unchanged) is greater than the glomerular filtration rate due to the active tubular secretion
Adverse effect: Dry cough (1% to 10%)
Proteinuria (1%), which subsides or clears within 6 months even when captopril therapy is continued
Renal insufficiency, renal failure, nephrotic syndrome, polyuria, oliguria, and urinary frequency (0.1% to 0.2%) Neutropenia (<1000/mm3) or agranulocytosis with myeloid hypoplasia Rash with pruritus and occasionally with fever, arthralgia, and eosinophilia (4% to 7%) Angina pectoris, myocardial infarction, Raynaud syndrome, and congestive heart failure (0.2% to 0.3%) Dysgeusia (diminution or loss of taste perception) is reversible and usually self-limited (2% to 4%) Anaphylactoid and other related reactions due to the inhibition of the metabolism of eicosanoids and polypeptides, including bradykinin Intestinal angioedema, which presents as abdominal pain with or without nausea or vomiting Flushing or pallor Tachycardia, chest pain, and palpitations, Hypotension
Contraindications:
Hypersensitivity to captopril, any component of the formulation, or any other ACEI. Angioedema related to previous treatment with ACEI. Concomitant aliskiren use in patients with diabetes Coadministration with or within 36 hours of switching to or from a neprilysin inhibitor (sacubitril)
Drug interaction: Sacubitril. …
High blood pressure drugs. …
Diuretics (water pills) …
Potassium supplements and potassium-based salts. …
Mood stabilizers. …
Pain drugs. …
Drugs to prevent organ transplant rejection. … Gold.
Special consideration: Captopril should be taken 1 hour before meals. Therapy initiation requires analysis of recent antihypertensive drug treatment, the extent of blood pressure elevation, and salt restriction. If possible, the previous antihypertensive drug regimen should be stopped 1 week before starting captopril.
Melting point: 103°c
Boiling point: 108°c
Pka: Captopril has two Pka values: 3.7 and 9.8
Stability: As a solid, captopril is stable; however, in solution, it undergoes free-radical oxidation to yield captopril disulfide as the major degradation product. This degradation is complex and concentration and pH dependent, with the highest stability at pH 3.5.
Carriers:
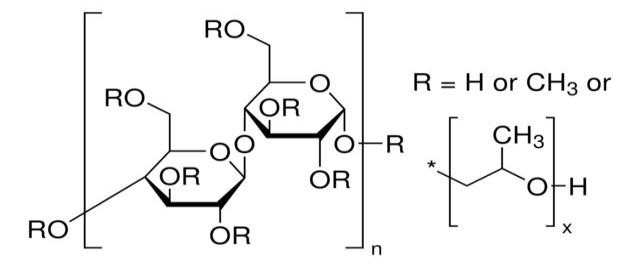
Polymer Profile
Table No 2: HPMC E15
|
Non-proprietary name |
hydroxypropyl methylcellulose (HPMC). |
|
Synonym |
“Hydroxypropyl methylcellulose,” “Hypromellose,” “Cellulose, 2hydroxypropyl methyl ether,” and “2-Hydroxypropyl cellulose methyl ether” |
|
Description |
Hydroxypropyl methylcellulose (hpmc), hpmc is white or milky white, odourless and tasteless, fibrous powder or granules, the loss on drying does not exceed 10%, may be dissolved in cold water but not in warm water, slowly in warm water swells, peptizes, forms a viscous colloidal solution, cools to an answer, and for .. |
|
Structural formula |
|
|
Chemical Name |
Hydroxy Propyl Methyl Cellulose Hpmc E 15 Lv Premium. |
|
Empherical Formula |
Hydroxypropyl Methylcellulose (HPMC), including the E15 grade, is C56H108O30. |
|
Molar weight |
HPMC (Hypromellose), including grades like HPMC-E15, typically ranges from around 10,000 to 1,500,000 g/mol |
|
Freezing point |
HPMC-E15, being a solid, doesn’t have a freezing point in the traditional sense, as it decomposes before melting. Instead, it’s known to decompose before melting, and its melting point/range is around 225-230°C. |
|
Solubility |
HPMC E15, a type of hydroxypropyl methylcellulose, does not have a defined freezing point as it is a solid powder and decomposes before melting. Instead, its melting point/range is typically observed at 225-254°C |
|
Viscosity |
HPMC E15, a type of hydroxypropyl methylcellulose, typically exhibits a viscosity of around 15 centipoises (cP) or 15 mPa·s when |
|
PH |
The pH of a 2% aqueous solution of HPMC E15 typically falls within the range of 5.0 to 8.0. |
|
Functional categories |
HPMC E15, a type of hydroxypropyl methylcellulose, functions as a binder, film-forming agent, and controlled-release agent in pharmaceutical formulations, also acting as a thickening agent and stabilizer in other applications. |
|
Storage conditions |
Keep it in a dry, cool place, in a tightly closed container, and away from heat and ignition sources. |
|
Incompatibilities’
|
HPMC E15, a type of hydroxypropyl methylcellulose, is generally considered compatible with many pharmaceutical ingredients and excipients, but potential incompatibilities can arise depending on the specific formulation and processing conditions. |
|
Safety |
Hydroxypropyl methylcellulose (HPMC), including the E15 grade, is generally considered safe for use in food and pharmaceutical applications, with approvals from the FDA and EU. However, like any substance, it’s important to handle it with caution and follow safety guidelines, especially when dealing with dust formation. |
|
Applications |
HPMC E15 is widely used as a Binder: Used in tablet formulations to help ingredients bind together. Film-forming agent: Used to coat tablets and pills, protecting them from environmental factors and enhancing their appearance. Disintegrant: Promotes the breakdown of tablets in water, aiding in drug release and absorption. Suspension agent: Used in liquid formulations to prevent particles from settling and ensuring uniform distribution of the drug. |
|
|
Thickener: Modifies the viscosity of liquid and semi-solid formulations, improving their stability and ease of use. Ophthalmic formulations: Used as a matrix material in eye drops and other ophthalmic preparations. |
MATERIAL AND METHOD
Formula development
Captopril Mouth Dissolving Film – Formula [ per 10 films]
Table No. 3. formula of mouth dissolving film
|
Ingredient |
Quantity |
Function |
|
Captopril |
25 mg |
Active pharmaceutical ingredient |
|
Hydroxypropyl methylcellulose [HPMC] |
100 mg |
Film forming-Polymer |
|
Polyethylene glycol 400 |
10 mg |
Plasticizer |
|
Citric acid |
5 mg |
Saliva stimulating agent |
|
Glucose |
2-5 mg |
Sweetener |
|
Methanol /flavouring agent |
1-3 mg |
Flavour enhancer |
|
Distilled water |
q. s |
Solvent |
4.4 Preparation of mouth dissolving film
1. Polymer Solution Preparation
Description: Hydroxypropyl methylcellulose (HPMC E15) is dissolved in distilled water and allowed to swell.
Visual: A clear, viscous solution in a beaker, often stirred using a magnetic stirrer.
2. Addition of Plasticizer and Excipients
Description: Polyethylene glycol 400 (PEG 400), citric acid, sweeteners and flavouring agents are added to the polymer solution with continuous stirring
Visual: The solution remains clear, with all components uniformly mixed.
3. Incorporation of Captopril
Description: Captopril is added to the solution and stirred until completely dissolved.
Visual: A homogeneous solution, ensuring even distribution of the drug.
4. Casting the Film
Description: The final solution is poured onto a flat, levelled surface (like a glass plate) and spread uniformly using a film applicator.
Visual: A wet, uniform layer of solution spread over the casting surface.
5. Drying the Film
Description: The cast film is dried at 40°C in a hot air oven until the solvent evaporates completely.
Visual: A dry, transparent film formed on the casting surface.
6. Cutting and Packaging
Description: The dried film is carefully peeled off and cut into desired sizes (e.g., 2x2 cm squares), each containing a specific dose of Captopril.
Visual: Uniformly cut film strips, ready for packaging.

Fig no.4 Mouth Dissolving Film Contaning Captopril

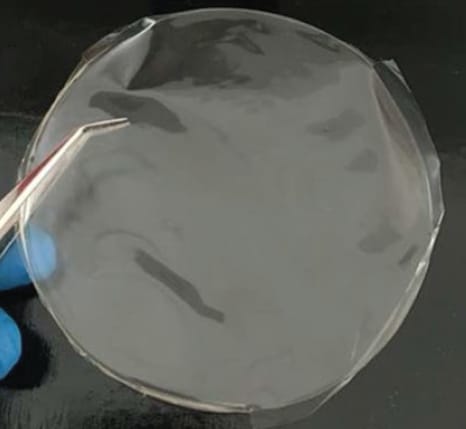
Figure.no.5. Dry mouth dissolving films of captopril
RESULTS AND DISCUSSION:
The films were uniform, smooth, and transparent. Evaluation results are summarized below:
Evaluation Parameters and Results:
Table No. 4. Evaluation Parameters and Results
|
Test parameter |
Method used |
Observed result |
Specification/Acceptance criteria |
|
Appearance |
Visual inspection |
Transparent, smooth, uniform |
Smooth, no bubbles or cracks |
|
Thickness |
Digital micro meter [mean of 3 reading] |
0.18 0.02nm |
Uniform across film |
|
Weight Uniformity |
Analytical balance [10 films] |
105±3 mg |
±10% of average weight |
|
Folding Endurance |
Manual folding at same place |
>300 folds |
should not break before 300 folds
|
|
Surface PH |
PH meter after moistening film with 1ml water |
6.7± 0.1 |
6.5-7.5 (neutral, non-irritating) |
|
Disintegration Time |
In petri dish with 5 ml simulated saliva [37?] |
22±3 seconds |
<30 seconds ideal |
|
Tensile Strength |
Texture analyzer or tensile texture |
3.1±0.2N/mm2 |
2-5 N/mm² for good handling |
|
% Elongation |
Tensile tester |
12±2% |
10 flexible films |
|
Drug Content Uniformity |
UV spectrophotometry at 212nm [n=3] |
98.6±1.5% |
95-105% of labelled claim
|
|
In-vitro Drug release |
USP paddle at 50 rpm in 900 ml phosphate buffer PH 6.8 |
92% within 5 minutes |
≥85% drug release within 5-10 minutes |
|
Moisture Content |
Dedicator [by weight loss] |
3.2±0.4% |
Should be low (<5%) to prevent degradation |
The formulation successfully met all critical quality attributes, ensuring its suitability for oral delivery. Rapid disintegration and high drug release support its potential in clinical use.
CONCLUSION:
Mouth-dissolving films (mdfs) have emerged as a transformative drug delivery platform, offering a patient-friendly alternative to conventional oral dosage forms. Their ability to rapidly disintegrate in the oral cavity without water, coupled with enhanced bioavailability and faster therapeutic action, addresses key limitations faced by traditional tablets and capsules. Mdfs are particularly valuable for special populations and in emergency scenarios where swift drug administration is critical. The integration of advanced manufacturing techniques such as solvent casting, hot melt extrusion, and nanotechnology has significantly improved film quality, drug stability, and therapeutic efficacy. Additionally, innovations like 3d printing and multilayer design have enabled the development of personalized and targeted therapies, broadening the scope of mdf applications across various medical and consumer health sectors. Despite existing formulation and scalability challenges, ongoing research and technological progress continue to drive the evolution of mdfs, positioning them as a pivotal component in the future of efficient, patient-centric drug delivery systems. The formulated captopril mdf showed promising results with quick disintegration, good mechanical properties, and satisfactory drug release. This dosage form is particularly beneficial for patients who have difficulty swallowing tablets, enhancing convenience and compliance. The evaluated mouth dissolving film meets all standard pharmaceutical requirements for quick-dissolving oral films. It is mechanically strong, disintegrates quickly, and releases captopril efficiently, making it suitable for paediatric or geriatric use.
REFERENCES

Gaikwad Mayuri*, Fufane Aditi, Gadekar Kalpesh, Dhumse Pradip, Taral M. N., Formulation and Evaluation of Captopril Loaded Mouth Dissolving Films for Rapid Antihypertensive Action, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 2612-2625. https://doi.org/10.5281/zenodo.15430207
 10.5281/zenodo.15430207
10.5281/zenodo.15430207
