1M Pharmacy, Matoshri College of pharmacy, Eklahare, Nashik, Maharashtra
2Department of Pharmaceutics, Matoshri College of pharmacy, Eklahare, Nashik, Maharashtra
3Department of Pharmaceutical Chemistry, Matoshri College of pharmacy, Eklahare, Nashik, Maharashtra
In 2007, sitagliptin, the first drug in a new family of oral glucose-lowering drugs, was introduced to the UK market. When hyperglycemia is present, it suppresses the secretion of glucagon and increases the secretion of insulin. The goal of the current study is to use lactose as a diluent in a direct compression approach to create a novel drug delivery system: sustained release tablets of the antidiabetic medication sitagliptin phosphate monohydrate. FTIR investigations were used to rule out the drug-excipient interaction. Using xanthan gum (X1) and microcrystalline cellulose (MCC) (X2), nine formulations of sitagliptin phosphate tablets were created based on factors like hardness and dissolving profile. Organoleptic characteristics, hardness, friability, weight fluctuation, and in vitro drug release were assessed for the manufactured batches. Each formulation exhibited a sluggish rate of disintegration and minimal weight fluctuation. The formulation made with 27.5% xanthan gum ended up being the best overall out of nine potential formulations. This optimized formulation (F5) showed good dissolution profile with 99.61% drug release within 10 hours. It was concluded that sustained release tablets of Sitagliptin Phosphate Monohydrate can be successfully formulated by using Xanthan gum natural polymer.
Diabetes mellitus, which is sometimes just called diabetes, is a metabolic condition that results in elevated blood sugar levels. Insulin transports blood sugar into your cells so that it can be stored or used as fuel. [1]
Types of diabetes
There are a few different types of diabetes:
Type 1: An autoimmune condition is type 1 diabetes. The cells that produce insulin in the pancreas are attacked and destroyed by the immune system. The reason for this strike is unknown.
Type 2: When sugar accumulates in your blood and your body grows resistant to insulin, type 2 diabetes develops. Type 2 diabetes is the most prevalent kind, with 90% to 95% of persons with the disease having this reliable source.
Gestational: High blood sugar during pregnancy is known as gestational diabetes. This kind of diabetes is brought on by the placenta's production of insulin-blocking substances. [2]
Type 1 diabetes
What specifically causes type 1 diabetes is unknown to doctors. The pancreatic beta cells that produce insulin are unintentionally attacked and destroyed by the immune system. Some persons may have a genetic component. A virus may also trigger an attack on the immune system. [3]
Figure 1: Autoimmune attack in type 1 diabetes
Type 2 diabetes
Genetics and lifestyle factors work together to cause type 2 diabetes. Being obese or overweight also raises your risk. Your cells become more resistant to the effects of insulin on blood sugar when you carry excess weight, particularly in your abdomen. This illness is inherited. Genes that increase the risk of type 2 diabetes and obesity are shared by family members. [4]
Figure 2: Type 2 Diabetes
Gestational diabetes
Hormonal changes during pregnancy might lead to gestational diabetes. Hormones produced by the placenta reduce the sensitivity of a pregnant person's cells to the effects of insulin. Insulin resistance, which occurs when muscle and adipose cells are unable to react appropriately to normal insulin levels, is a hallmark of type 2 diabetes, a chronic metabolic illness. The Centers for Disease Control and Prevention predict that there are currently 26 million Americans with type 2 diabetes mellitus (DM), and by 2050, that number is expected to quadruple. One Diabetes is referred to be a "silent killer" because, if left untreated, chronic complications kill people more frequently than hyperglycemic crises. [2,3] One inhibitor of dipeptidyl peptidase-4 (DPP-4) is sitagliptin phosphate. Sitagliptin inhibits the enzyme dipeptidyl peptidase 4 (DPP-4) in a competitive manner. The gastrointestinal hormones GLP-1 and GIP, which are produced in reaction to a meal, are broken down by this enzyme. They can decrease the pancreatic release of glucagon and boost insulin secretion by blocking GLP-1 and GIP inactivation. Blood glucose levels are brought closer to normal as a result. Designing and refining Sitagliptin Phosphate sustained release tablets using the direct compression technique was the aim of this work. Directly compressible lactose was used to compress the optimum formulation into tablets. A dosage of 100 mg of sitagliptin phosphate was administered. Therefore, Sitagliptin Phosphate sustained release tablets were made in order to preserve the medicine's bioavailability and lower the frequency of drug administration. [5]
Purpose of the Study
The oral route of administration remains the most popular because of its many benefits, which include patient compliance, simplicity of intake, pain avoidance, and adaptability. The most often used dose forms are capsules and tablets. Taking traditional dosage forms on time and more than once a day causes variations in the drug's plasma concentration, which can cause missed doses. Sustained release formulations have been created to get around this. The benefits of these include less blood level swings, fewer doses, improved patient convenience and adherence, fewer negative side effects, and lower total medical expenses.
AIM:
To formulate and evaluate Sitagliptin Phosphate Monohydrate sustained release tablet by using natural polymers for type 2 diabetes mellitus.
OBJECTIVE
Drug Profile
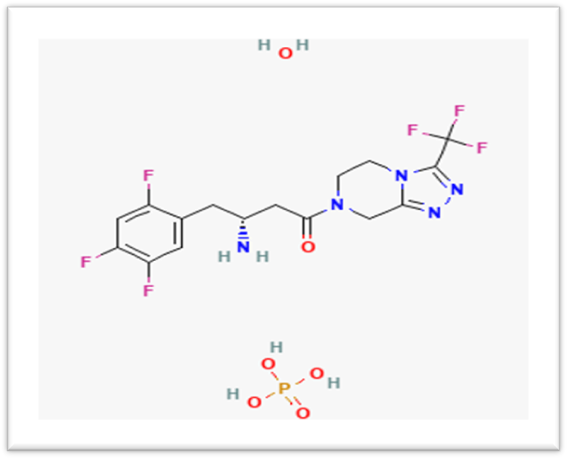
Sitagliptin
Chemical structure:
Colour: White
Molecular Formula: C16H20F6N5O6P
Catagory: Antidiabetic
Synonyms: Sitagliptin Phosphate, Januvia
CAS No.: 654671-77-9
Molecular Weight: 523.32 g/mol
Melting Point: 206-208 0C
Bioavailability: 87 %
BCS Classification: class-III (High soluble low permeable)
Dose: 100 mg twice a day with or without food [8,9]
MATERIALS & METHOD
Ingredients List
Table 1: Ingredients used for Sitagliptin Phosphate Monohydrate sustained release tablet
|
Sr.no. |
Ingredients |
Role |
|
1. |
Sitagliptin Phosphate Monohydrate |
Anti-diabetic |
|
2. |
Xanthan gum |
Sustained release polymer |
|
3. |
Microcrystalline cellulose (MCC) |
Binder |
|
4. |
Lactose |
Diluent |
|
5. |
Magnesium stearate |
Lubricant |
|
6. |
Talc |
Glidant |
Prepration of Sitagliptin Phosphate Monohydrate sustained release tablet
Before tablet preparation, the mixture blend of all the ingredients were subjected to precompression parameters like Angle of repose, Bulk density, Tapped density, Compressibility index and Hausner’s ratio.
EXPERIMENTAL WORK
1. Preformulation study:
A. Drug Characterization:
Drug characterization parameters such as colour, odour and appearance were analysed for the procured drug samples
Table 2: Drug characterization parameters
|
Colour |
White |
|
Odour |
Odourless |
|
Appearance |
Fine powder |
B. Determination of melting point:
The melting point of Sitagliptin PM was found to be in the range of 206-208 0C which comply with reported melting point of Sitagliptin PM
C. Solubility study:
The solubility study of Sitagliptin PM was carried out by using different solvent systems as per the literature. The solubility results were shown in table
Table 3: Results for solubility study
|
Sr.no |
Solvent |
Observation |
|
1. |
Methanol |
Soluble |
|
2. |
Phosphate buffer 6.8 pH |
Soluble |
|
3. |
0.1 N Hydrochloric acid |
Soluble |
|
4. |
Water |
Soluble |
UV-visible spectrophotometric analysis
The UV-visible spectrophotometric analysis of drug was carried out 0.1N hydrochloric acid as well as Phosphate buffer 6.8 pH were used as solvent system for determination of λ max 40 µg/ml of Sitagliptin PM sample was used and λ max was found as 266 nm for 0.1N HCl and 267 nm for PB 6.8 pH respectively.
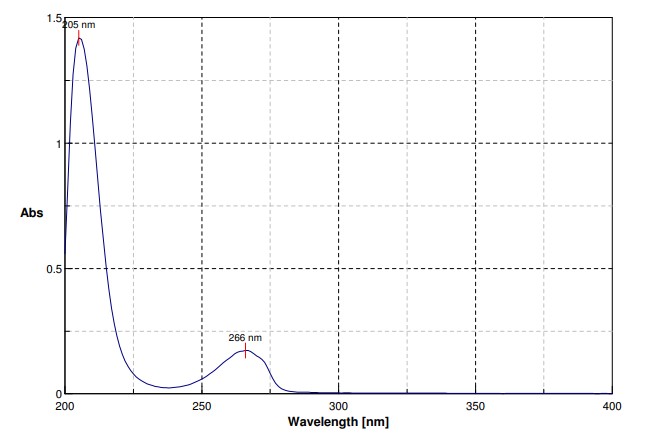
Figure 3: 40 PPM solution of Sitagliptin PM in 0.1 N hydrochloric acid
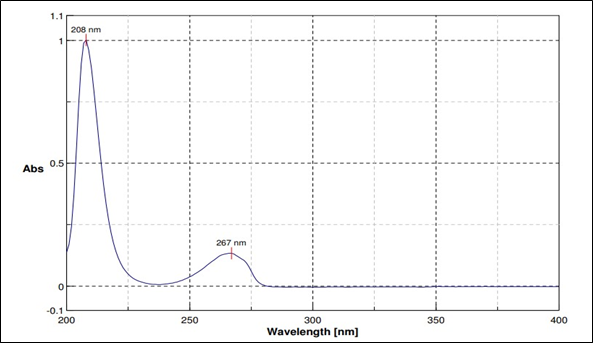
Figure 4: 40 PPM solution of Sitagliptin PM in Phosphate buffer 6.8 pH
Preparation of Calibration curve for Sitagliptin PM in 0.1 N Hydrochloric acid
The calibration curve of Sitagliptin PM was drawn by measuring the absorbance of different concentrations in 0.1N hydrochloric acid at 266 nm
Table 4: Calibration curve for Sitagliptin PM in 0.1N Hydrochloric acid
|
Sr.no. |
Concentration (ppm) |
Absorbance |
|
1. |
10 |
0.0475 |
|
2. |
20 |
0.0981 |
|
3. |
30 |
0.1311 |
|
4. |
40 |
0.1708 |
|
5. |
50 |
0.2139 |
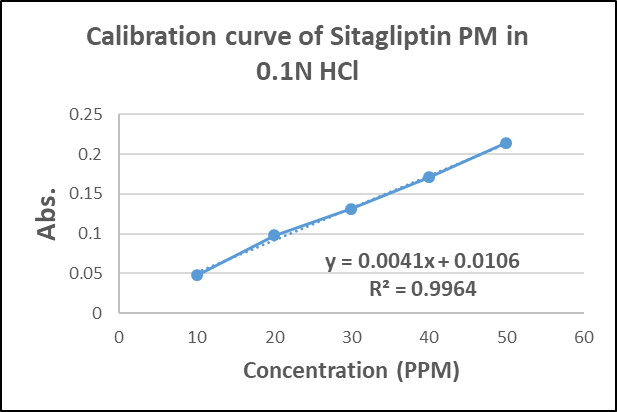
Figure 5: Calibration curve for Sitagliptin PM in 0.1N Hydrochloric acid
The calibration curves were linear and obeyed Beer-Lambert’s law in the concentration range 10-50 μg/ml. The correlation coefficient values were 0.9964 indicating excellent linearity of the data.
B. Preparation of Calibration curve for Sitagliptin PM in Phosphate buffer 6.8 pH:
The calibration curve of Sitagliptin PM was drawn by measuring the absorbance of different concentrations in phosphate buffer 6.8 pH at 267 nm.
Table 5: Calibration curve for Sitagliptin in Phosphate buffer 6.8 pH
|
Sr.no. |
Concentration (ppm) |
Absorbance |
|
1. |
10 |
0.0418 |
|
2. |
20 |
0.0782 |
|
3. |
30 |
0.1079 |
|
4. |
40 |
0.1347 |
|
5. |
50 |
0.1795 |
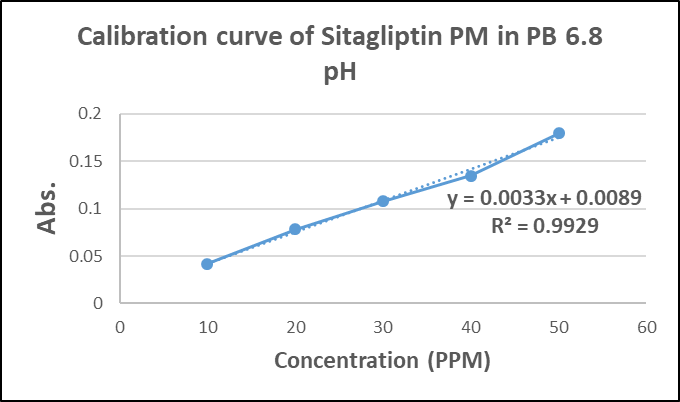
Figure 6: Calibration curve for Sitagliptin PM in phosphate buffer 6.8
Drug excipient compatibility study:
Drug excipient interaction studies are significant for the successful formulation of every dosage form. Fourier Transform Infrared (FTIR) Spectroscopy studies were used for the assessment of physicochemical compatibility and interactions, which helps in the prediction of interaction between drug and other excipients. In the current study 1:1 ratio was used for preparation of physical mixtures used for analyzing of compatibility studies.
Table 6: Drug excipient compatibility
|
Ingredient |
Ratio |
Initial |
Condition |
|
40°C/75% RH (Accelerated) |
|||
|
1 month |
|||
|
Sitagliptin Phosphate monohydrate |
NA |
White |
NCC |
|
Sitagliptin PM: Xanthan gum |
1:1 |
White |
NCC |
|
Sitagliptin PM: MCC |
1:1 |
White |
NCC |
|
Sitagliptin PM: Lactose |
1:1 |
White |
NCC |
|
Sitagliptin PM: Magnesium stearate |
1:1 |
White |
NCC |
|
Sitagliptin PM: Talc |
1:1 |
White |
NCC |
Note- NCC means No Conformational Change
Formulation development of Sustained Release Tablets
All the formulations were prepared by Direct Compression method. The compositions of different formulations are given in Table.
Table 7: Formulation strategy
|
Sr.No. |
Ingredients |
Quantity (mg) |
||||||||
|
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
F9 |
||
|
1 |
Sitagliptin Phosphate monohydrate |
128.5 |
128.5 |
128.5 |
128.5 |
128.5 |
128.5 |
128.5 |
128.5 |
128.5 |
|
2 |
Xanthan gum |
87.5 |
87.5 |
87.5 |
96.25 |
96.25 |
96.25 |
105 |
105 |
105 |
|
3 |
Microcrystalline cellulose (MCC) |
52.5 |
61.25 |
70 |
52.5 |
61.25 |
70 |
52.5 |
61.25 |
70 |
|
4 |
Lactose |
67.5 |
58.75 |
50 |
58.75 |
50 |
41.25 |
50 |
41.25 |
32.5 |
|
5 |
Magnesium stearate |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
|
6 |
Talc |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
7 |
|
Total weight of tablet |
350 mg. |
|||||||||
Evaluation of formulated batches:
A. Precompression parameters
The powder blend from all the batches were evaluated for density and flow property parameters which includes Bulk density, Tapped density, Compressibility index, Hausner’s ratio and Angle of repose.
Table 8: Precompression parameters
|
Batches |
Bulk density |
Tapped density |
Compressibility index |
Hausner’s ratio |
Angle of repose |
|
F1 |
0.4545 |
0.5224 |
12.99 |
1.15 |
29.25 |
|
F2 |
0.4516 |
0.5147 |
12.26 |
1.14 |
28.39 |
|
F3 |
0.4487 |
0.5109 |
12.18 |
1.14 |
30.41 |
|
F4 |
0.4545 |
0.5263 |
13.64 |
1.16 |
29.79 |
|
F5 |
0.4403 |
0.5147 |
14.47 |
1.17 |
30.03 |
|
F6 |
0.4321 |
0.4930 |
12.35 |
1.14 |
27.5 |
|
F7 |
0.4605 |
0.5303 |
13.16 |
1.15 |
28.39 |
|
F8 |
0.4403 |
0.5000 |
11.95 |
1.14 |
29.01 |
|
F9 |
0.4516 |
0.5109 |
11.61 |
1.13 |
29.29 |
B. Post compression parameters:
1. Physical appearance:
The tablets from all trial batches were white round convex shaped beveled edge with having plane upper and lower side.
2. Thickness and diameter:
The thickness and diameter for all the tablets were measured by using Vernier caliper by picking the tablets randomly. Thickness was found in the range from 5.0 mm to 5.2 mm respectively and diameter was found in the range of 9.7 – 9.9 mm. Uniformity in the values indicates that formulations were compressed without sticking to the dies and punches.
3. Hardness:
Monsanto hardness tester was used for the determination of hardness for all the batches Hardness was found to be in range of 7.5 kg/cm2 to 9 kg/cm2. The hardness for all formulated batches were uniform and possess good mechanical strength with sufficient hardness
4. Friability
Tablets from all batches were evaluated by using Roche Friabilator and Friability was acceptable range 0.29 to 0.86 (Less than 1%). The result was given in table
Table 9: Post compression parameters
|
Batches |
Thickness (mm) |
Diameter (mm) |
Hardness (kg/cm2) |
Friability (%) |
|
F1 |
5.1±0.1 |
9.9±0.1 |
7.5±0.5 |
0.29 |
|
F2 |
5.0±0.2 |
9.8±0.2 |
8±0.5 |
0.56 |
|
F3 |
5.0±0.2 |
9.9±0.1 |
8±0.5 |
0.29 |
|
F4 |
5.1±0.1 |
9.7±0.1 |
7.5±0.5 |
0.58 |
|
F5 |
5.0±0.2 |
9.8±0.2 |
8.5±0.5 |
0.56 |
|
F6 |
5.1±0.2 |
9.8±0.2 |
8.5±0.5 |
0.29 |
|
F7 |
5.0±0.1 |
9.9±0.2 |
8±0.5 |
0.58 |
|
F8 |
5.2±0.3 |
9.7±0.2 |
8.5±0.5 |
0.59 |
|
F9 |
5.1±0.2 |
9.8±0.2 |
9±0.5 |
0.86 |
5.Drug content
Drug content uniformity test was performed for all formulated batches and results were expressed in table 10. The drug content was found to be between 98- 102 % which was under specified limit.
Table 10: Drug content
|
Batches |
Drug content |
|
F1 |
100.61 |
|
F2 |
101.82 |
|
F3 |
101.21 |
|
F4 |
101.52 |
|
F5 |
100.91 |
|
F6 |
101.82 |
|
F7 |
100.91 |
|
F8 |
100.61 |
|
F9 |
100.00 |
7. In vitro dissolution test:
The in vitro evaluation of all the formulated batches were carried out for 10 hrs. by using 0.1N hydrochloric acid (0 – 2 hrs.) and Phosphate buffer 6.8 pH (3 – 10 hrs.)
Table 11: In vitro dissolution
|
Time (hrs.) |
Batches
|
% Cumulative Drug Release (%) |
||||||||
|
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
F9 |
||
|
1 |
8.76 |
8.01 |
8.34 |
8.67 |
7.75 |
7.53 |
7.75 |
6.80 |
6.72 |
|
|
2 |
20.15 |
17.96 |
19.03 |
18.37 |
18.99 |
18.77 |
18.53 |
17.71 |
19.05 |
|
|
3 |
38.75 |
38.57 |
39.05 |
28.27 |
28.53 |
27.33 |
26.71 |
25.02 |
25.65 |
|
|
4 |
51.08 |
48.91 |
49.58 |
40.57 |
39.55 |
40.37 |
39.83 |
35.09 |
34.79 |
|
|
5 |
62.07 |
59.90 |
60.57 |
51.56 |
50.54 |
51.36 |
50.82 |
46.08 |
45.78 |
|
|
6 |
74.59 |
71.03 |
72.10 |
65.99 |
62.65 |
64.48 |
61.65 |
55.51 |
54.62 |
|
|
7 |
85.71 |
83.33 |
82.20 |
73.49 |
71.38 |
72.22 |
71.14 |
65.61 |
64.41 |
|
|
8 |
95.21 |
91.02 |
89.59 |
81.26 |
79.59 |
80.43 |
77.60 |
75.01 |
72.29 |
|
|
9 |
95.94 |
93.83 |
94.06 |
89.36 |
90.93 |
86.08 |
85.70 |
81.42 |
78.29 |
|
|
10 |
96.51 |
97.67 |
96.62 |
98.55 |
99.61 |
96.41 |
92.90 |
89.71 |
87.70 |
|
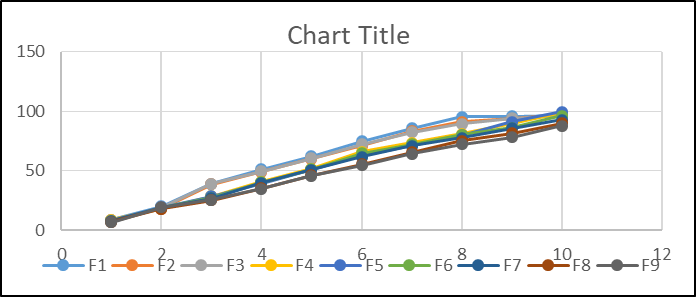
Figure 7: In vitro dissolution study
Evaluation of optimized batch:
Table 12: Evaluation of optimized batch
|
Sr.no. |
Evaluation parameter |
Results |
|
1. |
Thickness |
5.1 mm |
|
2. |
Diameter |
9.8 mm |
|
3. |
Hardness |
8.5 kg/cm2 |
|
4. |
Friability |
0.56 % |
|
5. |
Drug content |
100.91 % |
|
6. |
In vitro dissolution (%CDR) |
99.61% |
Stability study
The optimized formulation batch of Sitagliptin Phosphate Monohydrate sustained release tablet was wrapped in an aluminum foil and subjected to 40 ± 20C temperature and 75 ± 5% RH in stability chamber for the period of 1 months. The formulation was analyzed for Physical appearance, Thickness, Hardness, Drug content and Dissolution study. In any rational design of dosage forms for drug, the stability of the active component is the major criteria in determining their acceptance or rejection. Stability studies were carried out as per ICH Q1A(R2) guidelines.
Table 13: Stability study
|
Evaluation parameters |
Results |
|
Physical appearance |
White round convex shaped |
|
Thickness |
5.1±0.2 |
|
Hardness |
8.5 kg/cm2 |
|
Drug content |
99.73 % |
|
Dissolution study |
96.61% |
RESULT AND DISCUSSION
1. Weight variation: The weight of 20 tablets was determined, and the average weight is calculated. The individual weights of the tablets not vary more than 5% from the average weight.
2. Hardness: The hardness of the tablets was determined using a tablet hardness tester. The tablets should have sufficient hardness to withstand handling and transportation. Hardness of optimized F5 formulation was 8.5 kg/cm2
3. Friability: The friability of the tablets was determined using a friability tester. The tablets are subjected to tumbling action, and the percentage weight loss is calculated. The percentage weight loss should not be more than 1%.
4. Dissolution: The dissolution rate of the tablets is determined using a dissolution apparatus. The tablets are placed in a basket, and the basket is rotated in a dissolution medium. The amount of Sitagliptin Phosphate Monohydrate released from the tablet is measured at various time intervals. This optimized formulation (F5) showed good dissolution profile with 99.61% drug release within 10 hours.
5. Content uniformity: The content uniformity of the tablets is determined by assaying the Sitagliptin Phosphate Monohydrate content in 10 tablets individually. The amount of drug in each tablet should be within 85-115% of the labeled amount.
6. Stability: The stability of the tablets is determined by storing them at 25°C/60% RH for 1 month. The physical appearance, drug content, dissolution rate, and other parameters are monitored periodically to assess the stability of the tablets.
By evaluating the above parameters, we can ensure the quality and effectiveness of the sustained release Tablet of Sitagliptin Phosphate Monohydrate The chosen Sitagliptin Phosphate Monohydrate did not interact with the polymers, according to FTIR analyses of the drug and excipients. Sitagliptin sustained release tablets were significantly impacted by the drug polymer ratio. Every powder mix demonstrated the appropriate flow characteristics in accordance with pharmacopoeial standards. Following a 10-hour dissolving analysis, it was discovered that the drug release from formulations F1, F2, F3, F4, F5, F6, F7, F8, and F9 was 96.51%, 97.67%, 96.62%, 98.55%, 99.61%, 96.41%, 92.90%, 89.71%, and 87.70%, respectively. According to stability investigations, the physical properties and invitro drug release profiles of the manufactured Sitagliptin Phosphate Monohydrate tablets in optimized formulation F5 did not significantly alter. Formulation F5 was refined and used to create sustained release tablets. The results of many quality control tests performed on the prepared tablets are displayed in table No. 12.
CONCLUSION
The current study comes to the conclusion that by lowering the frequency of dosages, continuous drug administration of sitagliptin phosphate monohydrate may be an effective strategy to extend the duration of action of the medication. According to the current study, administering sitagliptin phosphate monohydrate should be done with a sustained drug delivery system. It was discovered that the F5 formulation was the most optimized.
REFERENCES


Samadhan Bandagar*, Shraddha Bhavsar, Dr. Gokul Talele, Dr. Prashant Malpure, Formulation development and evaluation of Sitagliptin Phosphate Monohydrate sustained release tablet by using natural polymers, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3956-3968. https://doi.org/10.5281/zenodo.15501129
 10.5281/zenodo.15501129
10.5281/zenodo.15501129
