1Assistant Professor, Department of Pharmacology & Therapeutics, MKCG Medical College & Hospital, Berhampur, Ganjam, Odisha, India
2Assistant Professor, School of Pharmacy, G H Raisoni Skill Tech University, Nagpur, Maharashtra, India
3Assistant Professor, Department of Pharmaceutical Chemistry, Agrawan Heritage University, Agra, Uttar Pradesh, India
4Principal, Department of Pharmacy, Integrated Academy of Management and Technology, Ghaziabad, Uttar Pradesh, India
5Assistant Professor, Department of Pharmacy Practice, SGT College of Pharmacy, SGT University,
Gurugram, India
6Associate Professor, Department of Pharmaceutical Chemistry, Goel Institute of Pharmaceutical Sciences, Lucknow, Uttar Pradesh, India
7Assistant Professor, Department of Pharmacy, Aryakul College Of Pharmacy & Research, Village Jajjaur, Post Manawa, Sidhauli, District Sitapur, Uttar Pradesh, India
8Assistant Professor, Department of Pharmacy, Shri Ramswaroop Memorial University, Uttar Pradesh, India
9Assistant Professor, Faculty of Pharmacy, Dr. M.G.R. Educational and Research Institute, Chennai, Tamil Nadu, India
Barbiturate-based narcoanalysis, historically derived from the clinical use of sedative-hypnotic agents such as Sodium thiopental and Sodium amytal, emerged in the early 20th century under the premise that pharmacological disinhibition could facilitate truthful disclosure. Although initially developed for therapeutic sedation and anesthesia, these agents were later repurposed in forensic contexts as so-called “truth serums.” Despite periodic use in investigative settings, the scientific validity, ethical permissibility, and legal admissibility of narcoanalysis remain highly contested.Objective-This integrative review critically evaluates the neuropharmacology, pharmacokinetics, toxicological risks, forensic reliability, ethical implications, and human rights dimensions of barbiturate-based narco test protocols. The review aims to determine whether such procedures meet contemporary standards of scientific validity, biomedical ethics, and constitutional due process.Methods-A multidisciplinary narrative synthesis was conducted across neuropharmacology, cognitive neuroscience, forensic psychology, toxicology, legal jurisprudence, and international human rights law. Peer-reviewed literature, judicial decisions, forensic science reform reports, and international regulatory frameworks were analyzed to assess empirical reliability, reproducibility, and normative compliance. Results Barbiturates exert their central nervous system effects through potentiation of GABAA_AA receptor-mediated inhibitory neurotransmission, resulting in dose-dependent sedation, hypnosis, anesthesia, and potential respiratory depression. Neurocognitive evidence indicates that such pharmacological states impair executive control, disrupt memory encoding and retrieval, and increase suggestibility and confabulation. No robust empirical data demonstrate that narcoanalysis enhances truthful disclosure; rather, findings suggest heightened vulnerability to leading questions and interrogator bias. Pharmacokinetic variability and lack of standardized protocols further undermine reproducibility. Toxicological risks include respiratory depression, cardiovascular instability, and potential long-term neuropsychological sequelae. Legally, involuntary narcoanalysis conflicts with constitutional protections against self-incrimination and with international human rights norms, including standards articulated by the United Nations. Courts in multiple jurisdictions have either rejected or strictly limited its admissibility. Conclusions Barbiturate-based narcoanalysis lacks sufficient scientific validation, fails evidentiary reliability standards, and raises substantial ethical and human rights concerns. Contemporary forensic practice should prioritize evidence-based, non-coercive investigative methodologies consistent with biomedical ethics and constitutional safeguards. The evolution of forensic neuroscience necessitates a clear demarcation between therapeutic pharmacology and investigative intervention.
1.1 Discovery and Early Synthesis of Barbiturates
Barbiturates represent one of the earliest classes of synthetic central nervous system (CNS) depressants to achieve widespread medical use. The parent compound, barbituric acid, was first synthesized in 1864 by Adolf von Baeyer, although it lacked intrinsic pharmacological activity (Sneader, 2005). The therapeutic potential of barbiturate derivatives was realized in the early 20th century when structural modifications yielded hypnotically active compounds. The introduction of barbital in 1903 marked the beginning of the barbiturate era, followed by phenobarbital in 1912, which became widely used for epilepsy management (Goodman & Gilman, 2018; Sneader, 2005). Among the most clinically significant derivatives were Sodium thiopental and Sodium amytal (amobarbital). Sodium thiopental, introduced in the 1930s, revolutionized anesthetic practice due to its rapid onset and short duration of action, making it ideal for induction of anesthesia (Evers & Maze, 2011). Sodium amytal gained prominence as a sedative-hypnotic and later as a tool in psychiatric interviews, particularly in the context of “narcosynthesis” for trauma-related disorders (Shorter, 1997). Barbiturates exert their pharmacological action primarily by enhancing γ-aminobutyric acid (GABA)-mediated inhibitory neurotransmission through the GABAA_AA? receptor complex, thereby producing dose-dependent CNS depression ranging from sedation to anesthesia and coma (Rang et al., 2016). Their narrow therapeutic index and high potential for respiratory depression, however, later contributed to their gradual replacement by benzodiazepines and other safer sedative-hypnotics (Goodman & Gilman, 2018).
1.2 Transition from Therapeutic Sedation to Investigative “Narcoanalysis”
The sedative and disinhibitory properties of barbiturates prompted early exploration beyond strictly therapeutic settings. During World War I and II, sodium amytal was used in psychiatric practice for the treatment of “shell shock” and war-related neuroses, under the premise that sedation could facilitate access to repressed memories (Shorter, 1997). This practice, termed “narcosynthesis,” formed the conceptual bridge between medical sedation and investigative interrogation. By the mid-20th century, law enforcement agencies in several countries began experimenting with sodium thiopental as an investigative aid, believing that pharmacologically induced disinhibition could weaken deliberate deception (Inbau et al., 2013). The technique, often referred to as “narcoanalysis” or “narco test,” was premised on the assumption that CNS depression would impair higher cortical inhibitory control, thereby compelling subjects to reveal concealed information (Ramsland, 2007). However, empirical evidence supporting the reliability of such methods has remained inconsistent. Studies demonstrated that while barbiturates may reduce anxiety and resistance, they also increase suggestibility and confabulation, thereby compromising the authenticity of elicited statements (Gudjonsson, 2003; Kassin et al., 2010). Consequently, the scientific validity of narcoanalysis has been widely questioned within forensic psychology and neuroscience literature.
1.3 The “Truth Serum” Phenomenon: Neuropsychological Foundations and Misconceptions
The popularized notion of a “truth serum” rests on the belief that pharmacological sedation suppresses executive control mechanisms located in the prefrontal cortex, thereby diminishing the capacity for intentional deception. Neurobiologically, deception involves complex cognitive processes including working memory, inhibitory control, and emotional regulation (Vrij, 2008). Barbiturate-induced depression of cortical circuits may reduce behavioral inhibition but does not selectively abolish the capacity to fabricate information (Rang et al., 2016). Indeed, research in cognitive psychology suggests that memory retrieval under sedation is highly vulnerable to distortion. Sedative agents impair encoding accuracy and enhance susceptibility to external suggestion, often resulting in confabulated or reconstructed memories rather than objective truth (Gudjonsson, 2003; Loftus, 2005). This phenomenon undermines the deterministic assumption that pharmacologically altered states yield inherently truthful disclosures.
Furthermore, deception detection research demonstrates that truthfulness cannot be reliably inferred solely from behavioral disinhibition (Kassin et al., 2010). The simplistic framing of barbiturates as “truth serums” therefore represents a neuropharmacological oversimplification unsupported by contemporary evidence.
1.4 Rationale for an Integrative Evaluation
Despite declining routine medical use of barbiturates in developed clinical settings, narcoanalysis continues to generate ethical and legal controversy in certain jurisdictions. The persistence of such practices necessitates a multidimensional evaluation encompassing neuropharmacology, pharmacokinetics, toxicology, ethics, and forensic reliability.
From a clinical perspective, barbiturates possess a narrow therapeutic window and carry substantial risks, including respiratory depression, hypotension, and fatal overdose (Goodman & Gilman, 2018). Toxicological risks are amplified in custodial or non-clinical environments where intensive monitoring may be inadequate (Evers & Maze, 2011). Ethically, involuntary narcoanalysis raises significant concerns regarding autonomy and informed consent, principles enshrined in international human rights standards articulated by the United Nations and reinforced by various constitutional protections against self-incrimination (UN General Assembly, 1948). Coercive pharmacological interrogation challenges foundational doctrines of medical ethics, particularly non-maleficence and respect for persons (Beauchamp & Childress, 2019). From a forensic standpoint, admissibility of narcoanalysis-derived statements has been widely contested due to issues of reliability, voluntariness, and potential violation of due process (Inbau et al., 2013). Contemporary forensic science increasingly emphasizes empirically validated methodologies, rendering pharmacologically induced testimony problematic within evidence-based frameworks.
1.5 Scope and Objectives of the Review
Given the historical trajectory of barbiturates from therapeutic sedatives to controversial investigative tools, an integrative scholarly reassessment is warranted. This review aims to:
By synthesizing clinical pharmacology, neuroscience, toxicology, forensic science, and bioethics literature, this review seeks to clarify whether barbiturate-based narcoanalysis represents a scientifically defensible investigative modality or a historically entrenched but empirically unsupported practice.
2. Chemical Classification and Pharmacodynamic Profile of Barbiturates
2.1 Structural Chemistry and Chemical Classification
Barbiturates are derivatives of barbituric acid (2,4,6-trioxohexahydropyrimidine), formed by condensation of malonic acid and urea. Although barbituric acid itself lacks CNS activity, substitution at the C5 position of the pyrimidine ring confers lipophilicity and pharmacological activity (Smith & Williams, 2012). The nature of the alkyl or aryl substituents at C5 largely determines lipid solubility, onset of action, and duration of effect.Increased lipid solubility enhances blood–brain barrier penetration, leading to rapid onset and shorter duration due to redistribution from brain to peripheral tissues (Katzung, 2021). Replacement of the oxygen atom at the C2 position with sulfur produces thiobarbiturates (e.g., Sodium thiopental), which are more lipid-soluble and exhibit faster onset compared to oxybarbiturates (Brunton et al., 2018).
Table 2.1. Classification of Barbiturates Based on Duration of Action
|
Class |
Example |
Onset |
Duration |
Clinical Use |
|
Ultra-short acting |
Thiopental |
Seconds |
5–15 min |
Induction of anesthesia |
|
Short acting |
Pentobarbital |
10–15 min |
3–4 h |
Sedation, seizures |
|
Intermediate acting |
Amobarbital |
30–60 min |
6–8 h |
Hypnotic (historical) |
|
Long acting |
Phenobarbital |
60 min |
>12 h |
Epilepsy management |
Determinants of Duration
Phenobarbital, for example, has relatively low lipid solubility and slower redistribution, contributing to prolonged anticonvulsant action (Katzung, 2021).
2.2 Mechanism of Action: GABAA Receptor Modulation
Barbiturates exert their CNS depressant effects primarily through positive allosteric modulation of the GABAA receptor–chloride ion channel complex. They bind to distinct sites separate from benzodiazepine binding domains and prolong the duration of chloride channel opening, thereby hyperpolarizing neuronal membranes (Olsen & Sieghart, 2009). At higher concentrations, barbiturates can directly activate GABAA ? receptors even in the absence of GABA—an important mechanistic distinction from benzodiazepines (Rudolph & Knoflach, 2011). Additionally, barbiturates inhibit excitatory AMPA-type glutamate receptors, further contributing to CNS depression (Franks, 2008).
Key Pharmacodynamic Effects
These actions collectively result in progressive depression of cortical and brainstem functions (Franks, 2008).
2.3 CNS Depression via Enhanced Inhibitory Neurotransmission
Barbiturates suppress neuronal excitability in a dose-dependent manner. Low doses produce anxiolysis and mild sedation; moderate doses induce hypnosis; high doses result in surgical anesthesia; excessive doses cause respiratory depression and coma (Brunton et al., 2018).
The ascending reticular activating system (ARAS), responsible for maintaining wakefulness, is particularly sensitive to barbiturate-induced inhibition (Kandel et al., 2021). Suppression of thalamocortical circuits reduces sensory perception and cognitive processing. Barbiturates also decrease cerebral metabolic rate (CMR) and cerebral blood flow (CBF), properties that historically contributed to their use in neuroprotective anesthesia (Franks, 2008).
2.4 Effects on Cortical and Subcortical Brain Regions
Barbiturate action is not uniform across brain regions. Differential sensitivity of neuronal circuits explains their cognitive and behavioral effects.
Hippocampus
Barbiturates impair long-term potentiation (LTP), a cellular correlate of memory consolidation (Kandel et al., 2021). This explains deficits in memory encoding and recall under sedation.
Amygdala
Suppression of amygdalar excitability reduces emotional reactivity and fear conditioning, contributing to disinhibition during interrogation contexts (LeDoux, 2012).
Prefrontal Cortex
Depression of dorsolateral prefrontal cortex function impairs executive control and inhibitory regulation, potentially increasing suggestibility (Miller & Cohen, 2001).
2.5 Dose-Dependent CNS Effects
The pharmacodynamic continuum of barbiturates is characterized by progressive CNS depression:
Table 2.2. Dose-Response Relationship
|
Plasma Concentration |
Clinical Effect |
|
Low |
Sedation, anxiolysis |
|
Moderate |
Hypnosis (sleep induction) |
|
High |
General anesthesia |
|
Very high |
Coma, respiratory arrest |
Unlike benzodiazepines, barbiturates lack a ceiling effect on CNS depression, significantly increasing overdose risk (Katzung, 2021). Respiratory centers in the medulla are particularly vulnerable, leading to fatal hypoventilation in toxic doses (Olsen & Sieghart, 2009).
2.6 Comparison with Benzodiazepines and Other Sedative-Hypnotics
Barbiturates have largely been replaced by benzodiazepines such as Diazepam due to improved safety profiles.
Table 2.3. Comparison Between Barbiturates and Benzodiazepines
|
Parameter |
Barbiturates |
Benzodiazepines |
|
GABA Action |
Prolong channel open duration |
Increase frequency of opening |
|
Direct GABA activation |
Yes (high dose) |
No |
|
Ceiling effect |
No |
Yes |
|
CYP450 induction |
Strong |
Minimal |
|
Overdose risk |
High |
Lower (unless combined with opioids) |
|
Dependence |
Significant |
Moderate |
Benzodiazepines exhibit a ceiling effect because they require endogenous GABA for activity, reducing fatal overdose risk (Rudolph & Knoflach, 2011). In contrast, barbiturates directly activate GABAA receptors at high doses, producing profound CNS suppression (Olsen & Sieghart, 2009). Non-barbiturate hypnotics (e.g., Z-drugs) selectively target α1 subunit-containing GABAA ? receptors, providing sedation with reduced muscle relaxation and anticonvulsant effects (Rudolph & Knoflach, 2011). Barbiturates are structurally defined by C5 substitution of the barbituric acid nucleus, with lipid solubility determining pharmacokinetic and pharmacodynamic behavior. Their primary mechanism involves potentiation and direct activation of GABAA receptors, leading to dose-dependent CNS depression. Effects on hippocampal, amygdalar, and prefrontal circuits explain cognitive impairment and behavioral disinhibition. Compared with benzodiazepines, barbiturates carry higher toxicological risk due to absence of a ceiling effect and stronger respiratory suppression.
3. Neuropharmacology of Memory, Cognition, and Suggestibility Under Barbiturate Influence
3.1 Neurobiology of Memory Encoding, Consolidation, and Retrieval
Human memory is a multistage neurobiological process involving encoding, consolidation, storage, and retrieval. Encoding depends on coordinated hippocampal–neocortical activity, particularly theta–gamma oscillatory coupling that facilitates synaptic plasticity (Buzsáki & Draguhn, 2004). Consolidation requires protein synthesis–dependent long-term potentiation (LTP) within hippocampal CA1 and dentate gyrus circuits (Bliss & Collingridge, 2013). Retrieval engages distributed cortical networks, including medial temporal lobe structures and prefrontal regulatory systems (Rugg & Vilberg, 2013).
At the molecular level, memory formation depends on NMDA receptor activation, calcium influx, CREB phosphorylation, and synaptic strengthening (Kandel, Dudai, & Mayford, 2014). Any pharmacological agent that enhances inhibitory neurotransmission or suppresses excitatory glutamatergic signaling can disrupt these processes. Barbiturates, through potentiation of GABAA_AA? receptor activity and inhibition of AMPA-mediated excitatory transmission, interfere with hippocampal synaptic plasticity and cortical integration necessary for memory encoding (Macdonald & Olsen, 1994; Franks, 2008).
3.2 Impact of Barbiturates on Hippocampal Function
The hippocampus plays a central role in declarative memory and contextual integration. Barbiturates reduce hippocampal neuronal firing rates and suppress LTP, thereby impairing encoding and consolidation (Perouansky & Hemmings, 2009).
Experimental electrophysiological studies demonstrate that thiobarbiturates decrease population spike amplitude in CA1 pyramidal neurons and attenuate NMDA receptor–dependent plasticity (Macdonald & Olsen, 1994). This suppression produces:
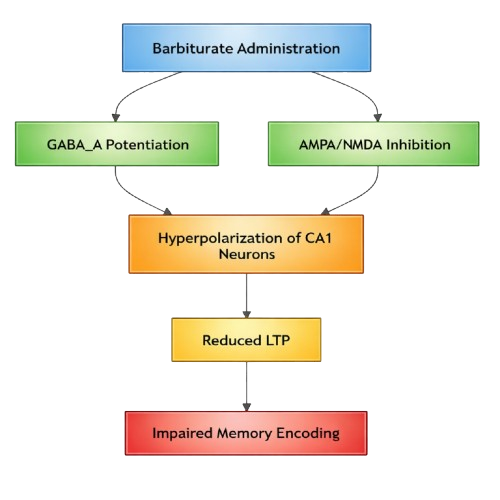
Figure 3.1. Barbiturate Effects on Hippocampal Synaptic Plasticity
Neurocognitive models suggest that disrupted hippocampal theta rhythms under sedation correlate with reduced episodic coherence (Buzsáki & Draguhn, 2004).
3.3 Effects on Executive Control and Prefrontal Cortex
Executive control, mediated by dorsolateral prefrontal cortex (DLPFC), governs working memory, inhibitory control, and deception management (Miller & Cohen, 2001). Functional neuroimaging research indicates that intentional deception requires increased DLPFC activation to suppress truthful responses (Christ et al., 2009).
Barbiturate-induced depression of prefrontal activity reduces inhibitory regulation and self-monitoring. This impairment may create an illusion of increased candor while simultaneously reducing cognitive accuracy.
Table 3.1. Executive Function Impairment Under Barbiturate Influence
|
Cognitive Domain |
Neural Substrate |
Barbiturate Effect |
Behavioral Outcome |
|
Working memory |
DLPFC |
Reduced firing rate |
Disorganized responses |
|
Inhibitory control |
Ventrolateral PFC |
Decreased suppression |
Disinhibition |
|
Error monitoring |
Anterior cingulate cortex |
Blunted activation |
Reduced self-correction |
|
Decision-making |
Orbitofrontal cortex |
Impaired valuation |
Increased suggestibility |
Reduced prefrontal inhibition may weaken deliberate deception but also diminishes critical evaluation of internally generated memories (Christ et al., 2009).
3.4 Modulation of Emotional Memory Circuits
The amygdala modulates emotionally salient memory encoding by interacting with hippocampal networks (Phelps & LeDoux, 2005). Barbiturates suppress amygdalar excitability and decrease noradrenergic facilitation of memory consolidation.
This results in:
However, emotional dampening does not equate to enhanced truthfulness. Emotional flattening may instead reduce resistance while simultaneously destabilizing memory integrity (Cahill & McGaugh, 1998).
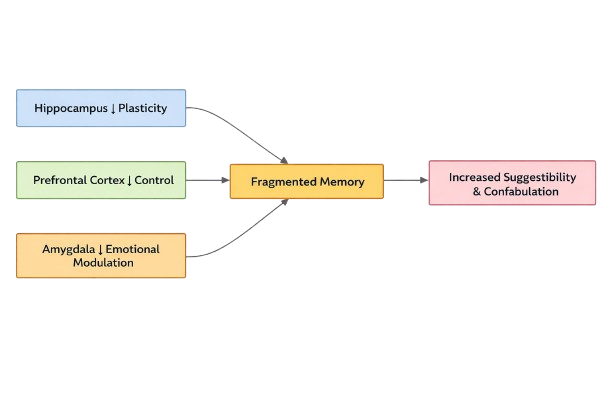
Figure 3.2. Interaction of Memory Circuits Under Barbiturate Sedation
3.5 Mechanisms Underlying Increased Suggestibility and Confabulation
Suggestibility refers to heightened susceptibility to external cues during memory retrieval. Confabulation involves generation of fabricated but subjectively believed memories (Gudjonsson, 2003).
Pharmacologically, suggestibility arises from:
Source monitoring—the ability to distinguish internally generated from externally suggested information—is critically dependent on prefrontal–hippocampal interaction (Johnson, Hashtroudi, & Lindsay, 1993). Barbiturate-induced suppression of this circuitry increases the probability of memory distortion.
Table 3.2. Neurocognitive Mechanisms of Confabulation
|
Mechanism |
Neural Basis |
Barbiturate Effect |
Outcome |
|
Source misattribution |
PFC–Hippocampus |
Reduced connectivity |
Memory distortion |
|
Pattern completion error |
CA3 network |
Impaired specificity |
False recall |
|
Suggestibility |
Executive inhibition |
Reduced skepticism |
Acceptance of leading questions |
|
Emotional detachment |
Amygdala suppression |
Lower resistance |
Compliance |
Experimental interrogation research indicates that cognitively impaired states significantly elevate false confession rates (Gudjonsson, 2003; Kassin et al., 2010).
3.6 Dissociation Between Perceived and Actual Truthfulness
Subjects under barbiturate influence may subjectively experience enhanced openness and authenticity due to decreased anxiety and inhibition. However, subjective confidence does not correlate with objective accuracy (Wixted & Wells, 2017).
This dissociation arises because:
Consequently, pharmacologically induced statements may appear spontaneous and credible while containing inaccuracies or fabrications.
3.7 Functional Neuroimaging Insights (EEG and fMRI Correlates)
EEG Findings
Barbiturates produce dose-dependent EEG slowing characterized by increased delta and beta oscillations and burst-suppression patterns at high doses (Brown, Purdon, & Van Dort, 2011). Reduced gamma synchronization correlates with impaired cortical integration.
fMRI Findings
Functional MRI studies show:
These patterns resemble global network disintegration observed during anesthetic-induced unconsciousness.
Neuroimaging evidence thus supports the conclusion that sedation disrupts network-level coordination required for accurate memory retrieval rather than selectively enhancing truth disclosure.
3.8 Integrated Interpretation
Barbiturate-induced potentiation of inhibitory neurotransmission disrupts hippocampal plasticity, prefrontal executive oversight, and amygdalar emotional modulation. These neurobiological effects collectively:
Neuroimaging findings further confirm global cortical suppression and reduced network coherence. Thus, from a neuropharmacological standpoint, barbiturate-induced states are incompatible with the assumption of enhanced forensic reliability.
4. Pharmacokinetics and Clinical Protocols in Narcoanalysis
Barbiturate-based narcoanalysis relies heavily on pharmacokinetic properties that permit rapid CNS penetration, controllable depth of sedation, and transient cognitive disinhibition. However, variability in absorption, redistribution, metabolism, and elimination substantially influences both clinical safety and forensic reliability (Katzung, 2021; Brunton et al., 2018).
4.1 Absorption, Distribution, Metabolism, and Excretion (ADME)
4.1.1 Absorption
In investigative contexts, barbiturates such as Sodium thiopental are administered intravenously to ensure rapid and predictable bioavailability. IV administration bypasses first-pass metabolism, producing near-complete systemic availability (Katzung, 2021). Oral barbiturates (e.g., Phenobarbital) demonstrate slower absorption influenced by gastric pH and intestinal motility (Brunton et al., 2018), but these are not typically used in narcoanalysis due to delayed onset.
4.1.2 Distribution
Barbiturates are weak acids with high lipid solubility (particularly thiobarbiturates), enabling rapid blood–brain barrier penetration. Following IV injection, peak brain concentrations occur within seconds (Shafer, 2010). Redistribution from brain to muscle and adipose tissue accounts for the short duration of ultra-short acting agents. This phenomenon explains why sedation may wane even while plasma levels remain elevated. Protein binding (40–60%) influences free drug availability. Hypoalbuminemia increases pharmacologically active unbound fraction (Kharasch & Brunt, 2016).
4.1.3 Metabolism
Barbiturates undergo hepatic metabolism primarily via cytochrome P450 (CYP) enzymes. Phenobarbital is a potent inducer of CYP3A4 and CYP2C9, accelerating metabolism of co-administered drugs (Zanger & Schwab, 2013).
Thiopental and amobarbital are metabolized via oxidative desulfuration and side-chain oxidation, producing inactive metabolites excreted renally (Brunton et al., 2018). Hepatic impairment prolongs elimination and increases risk of cumulative toxicity.
4.1.4 Excretion
Renal excretion of metabolites is influenced by urinary pH. Alkalinization of urine enhances elimination of weak acidic barbiturates through ion trapping (Katzung, 2021). Phenobarbital’s long elimination half-life (80–120 hours) contrasts sharply with thiopental’s short redistribution half-life (5–15 minutes), illustrating the distinction between redistribution and elimination kinetics (Shafer, 2010).
4.2 Lipophilicity and Rapid CNS Penetration
Thiobarbiturates possess sulfur substitution at the C2 position, increasing lipid solubility and facilitating rapid CNS penetration (Franks, 2008). High lipid solubility results in:
However, repeated dosing leads to accumulation in adipose tissue, prolonging sedative effects and increasing interindividual variability (Kharasch & Brunt, 2016).
Table 4.1. Lipophilicity and Onset Characteristics
|
Drug |
Lipid Solubility |
Onset |
Redistribution Half-life |
Clinical Implication |
|
Thiopental |
Very high |
20–30 sec |
5–15 min |
Rapid sedation |
|
Amobarbital |
Moderate |
30–60 min |
6–8 h |
Prolonged hypnotic effect |
|
Phenobarbital |
Low |
1 h |
Long |
Sustained anticonvulsant |
4.3 Elimination Half-Life Variability
Elimination half-life depends on hepatic metabolic capacity, renal clearance, and enzyme induction. Variability arises due to:
Elderly individuals exhibit prolonged elimination due to decreased hepatic blood flow and reduced metabolic capacity (Mangoni & Jackson, 2004).
4.4 Standardized and Non-Standardized Narco Test Protocols
There is no universally accepted medical protocol for narcoanalysis. Practices vary across jurisdictions, raising concerns regarding reproducibility and safety.
4.4.1 Dose Titration Strategies
Narcoanalysis typically involves incremental IV dosing of thiopental until a “twilight state” is achieved. Dose is titrated based on responsiveness, speech coherence, and sedation depth.
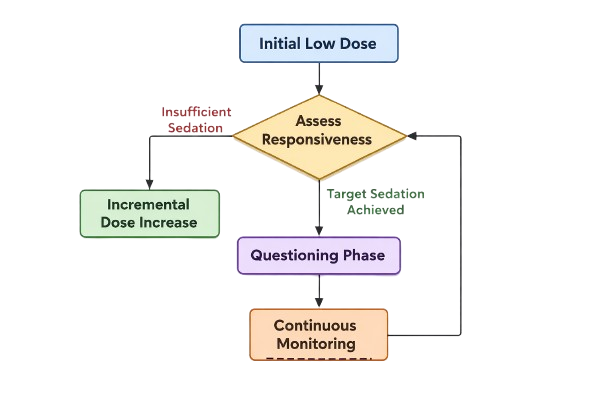
Figure 4.1. Dose-Titration Strategy
Overtitration risks respiratory depression and hemodynamic instability.
4.4.2 Monitoring Parameters
Clinical safety requires continuous monitoring:
EEG monitoring reveals progressive slowing and burst suppression at higher doses (Brown et al., 2011). Absence of structured monitoring increases medico-legal liability.
4.4.3 Adjunctive Agents
Adjunctive medications may include:
Polypharmacy complicates pharmacokinetic predictability and may potentiate respiratory depression.
4.5 Factors Influencing Interindividual Variability
Table 4.2. Determinants of Pharmacokinetic Variability
|
Factor |
Mechanism |
Clinical Impact |
|
Age |
Reduced hepatic clearance |
Prolonged sedation |
|
Hepatic disease |
Impaired CYP metabolism |
Accumulation |
|
Obesity |
Increased adipose storage |
Delayed recovery |
|
Chronic barbiturate use |
Enzyme induction |
Reduced efficacy |
|
Alcohol use |
Cross-tolerance |
Altered dose response |
|
Genetic polymorphisms |
Variable CYP activity |
Unpredictable plasma levels |
Tolerance develops through pharmacodynamic receptor adaptation and enzyme induction (Zanger & Schwab, 2013). Chronic exposure may necessitate higher doses, increasing toxicological risk.
4.6 Integrated Pharmacokinetic–Clinical Interpretation
The pharmacokinetic properties that enable rapid induction of sedation also introduce substantial variability and risk. Redistribution kinetics may create fluctuating levels of consciousness during interrogation. Hepatic metabolism and enzyme induction alter drug–drug interactions, complicating interpretation of behavioral responses. From a forensic standpoint, absence of standardized dosing algorithms and pharmacokinetic monitoring undermines reproducibility and evidentiary validity.
5. Toxicological Risks and Adverse Outcomes
Barbiturates possess a narrow therapeutic index, meaning that the margin between therapeutic sedation and life-threatening toxicity is small. In the context of narcoanalysis—where dosing is titrated to achieve altered consciousness rather than controlled anesthesia—the toxicological risk profile becomes particularly concerning (Nelson et al., 2019; Brunton et al., 2018).
5.1 Acute Toxicity: Respiratory Depression, Hypotension, and Cardiovascular Instability
5.1.1 Respiratory Depression
The most serious acute toxic effect of barbiturates is dose-dependent respiratory depression, mediated through suppression of medullary respiratory centers. Barbiturates decrease sensitivity of central chemoreceptors to carbon dioxide and reduce neuronal excitability in the brainstem (Weinbroum, 2001). Ultra-short acting agents such as Sodium thiopental may rapidly induce hypoventilation or apnea if overdosed. Unlike benzodiazepines, barbiturates lack a pharmacological antagonist equivalent to flumazenil, increasing fatality risk (Olsen & Sieghart, 2009).
5.1.2 Hypotension and Cardiovascular Instability
Barbiturates reduce systemic vascular resistance and myocardial contractility, leading to hypotension (Butterworth, Mackey, & Wasnick, 2018). Rapid IV administration may produce:
Patients with pre-existing cardiac disease or hypovolemia are at particularly high risk (Nelson et al., 2019).
5.2 Risk of Overdose and Fatal Complications
Barbiturate overdose remains a recognized cause of fatal poisoning worldwide. Toxic plasma concentrations suppress brainstem reflexes, leading to coma, aspiration, hypoxia, and death (Isbister & Balit, 2003).
Table 5.1. Toxic Dose and Clinical Manifestations
|
Plasma Level |
Clinical Manifestation |
|
Mild elevation |
Sedation, slurred speech |
|
Moderate |
Ataxia, confusion |
|
High |
Coma, hypotension |
|
Severe |
Apnea, cardiovascular collapse |
Unlike benzodiazepines, barbiturates directly activate GABAA_AA? receptors at high doses, eliminating any intrinsic ceiling effect (Rudolph & Knoflach, 2011). Combined CNS depressant exposure further increases mortality risk.
Management of overdose requires:
5.3 Long-Term Neuropsychological Sequelae
Chronic or repeated barbiturate exposure is associated with:
Experimental data suggest that prolonged GABAergic enhancement may impair neuroplasticity and synaptic remodeling (Bittigau et al., 2002). Long-term sedative exposure during neurodevelopment has been linked to neuronal apoptosis in animal models (Jevtovic-Todorovic et al., 2003).
Table 5.2. Long-Term Neurocognitive Effects
|
Domain |
Observed Sequelae |
|
Memory |
Impaired consolidation |
|
Attention |
Reduced sustained focus |
|
Executive function |
Poor decision-making |
|
Mood |
Depression, irritability |
Although narcoanalysis is typically short-term, repeated or improperly monitored procedures may increase cumulative neurotoxicity risk.
5.4 Drug Interactions
Barbiturates interact synergistically with other CNS depressants.
5.4.1 Alcohol
Concurrent alcohol ingestion markedly potentiates respiratory depression. Ethanol enhances GABAergic activity and inhibits NMDA receptors, compounding barbiturate effects (Koob & Volkow, 2016).
5.4.2 Opioids
Combination with opioids such as Morphine significantly increases risk of fatal respiratory suppression (Nelson et al., 2019). Both drug classes depress medullary respiratory centers via distinct but convergent mechanisms.
5.4.3 Antidepressants
Tricyclic antidepressants (e.g., Amitriptyline) may exacerbate hypotension and arrhythmias when combined with barbiturates. Additionally, barbiturate-induced CYP450 enzyme induction can alter plasma levels of selective serotonin reuptake inhibitors (Zanger & Schwab, 2013).
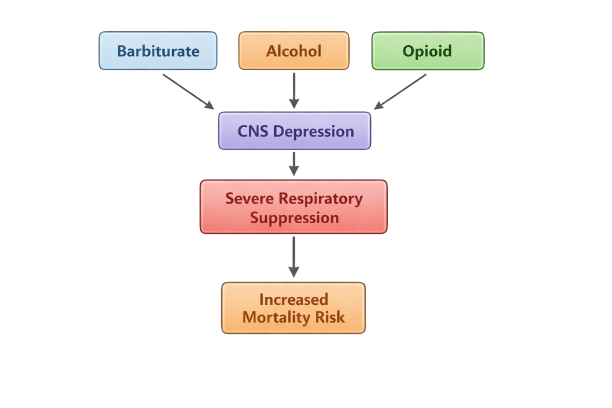
Figure 5.1. Synergistic CNS Depression
5.5 Dependence, Tolerance, and Withdrawal Syndromes
Barbiturates are associated with both physiological dependence and psychological addiction. Tolerance develops due to:
Abrupt discontinuation after chronic exposure may precipitate severe withdrawal characterized by:
Withdrawal may resemble delirium tremens and can be fatal without medical management (Nelson et al., 2019).
Table 5.3. Withdrawal Severity Spectrum
|
Stage |
Symptoms |
|
Early |
Anxiety, insomnia |
|
Intermediate |
Tremors, tachycardia |
|
Severe |
Seizures, delirium |
|
Critical |
Cardiovascular instability |
5.6 Case Reports of Morbidity and Mortality During Investigative Procedures
Although systematic global data are limited, reports from forensic and medico-legal literature document adverse events during narcoanalysis, including:
Improper dosing, lack of anesthetic monitoring, and inadequate resuscitation preparedness have contributed to morbidity (Weinbroum, 2001). Absence of standardized protocols further complicates attribution of causality and medico-legal accountability. From a forensic toxicology perspective, interpretation of barbiturate blood levels must consider redistribution effects and postmortem changes (Isbister & Balit, 2003).
5.7 Integrated Toxicological Perspective
Barbiturate toxicity is characterized by:
In investigative contexts lacking full anesthetic infrastructure, these risks are magnified. The absence of reversal agents, coupled with unpredictable pharmacokinetics and interindividual variability, underscores the inherent medical danger of barbiturate-based narcoanalysis.
6. Forensic Reliability and Evidentiary Validity
6.1 Scientific Evaluation of the “Truth Serum” Hypothesis
The characterization of barbiturates—particularly Sodium thiopental and Sodium amytal—as “truth serums” emerged in the early 20th century from anecdotal psychiatric observations suggesting that sedative-induced disinhibition facilitated disclosure (Bleckwenn, 1930; Redlich & Freedman, 1966). However, contemporary forensic neuropsychology rejects the premise that pharmacological sedation compels veridical speech (Gudjonsson, 2003; National Research Council [NRC], 2003). Barbiturates enhance GABAergic inhibition, reducing executive control and increasing suggestibility rather than enhancing memory accuracy (Bremner et al., 1993). Experimental studies indicate that sedative states may reduce deliberate deception but simultaneously impair source monitoring and increase confabulation (Kopelman, 1999; Loftus, 2005). Thus, the pharmacological mechanism underlying narcoanalysis promotes disinhibition, not epistemic reliability.
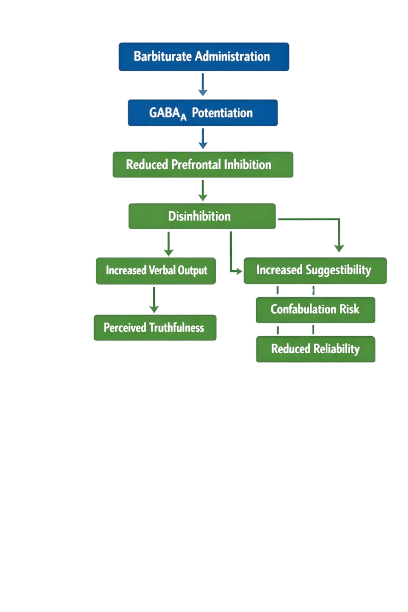
Figure 6.1. Conceptual Model of “Truth Serum” Effects
6.2 False Positives, Confabulation, and Memory Distortion
6.2.1 Confabulation Mechanisms
Confabulation refers to the production of fabricated or distorted memories without conscious intent to deceive (Kopelman, 1999). Sedative-induced impairment of frontal-limbic circuitry may disrupt monitoring processes necessary to distinguish authentic memory traces from reconstructed narratives (Johnson et al., 1993). Studies on amnestic and suggestible populations demonstrate that reduced executive oversight increases vulnerability to leading questions (Gudjonsson, 2003). Barbiturate intoxication may mimic such vulnerability states.
6.2.2 Empirical Evidence of Memory Distortion
Research in cognitive psychology shows that memory is reconstructive rather than reproductive (Loftus, 2005). Under sedative influence:
The NRC (2003) concluded that no scientifically validated evidence supports narcoanalysis as a reliable lie detection method.
Table 6.1. Sources of Error in Barbiturate-Based Interrogation
|
Error Type |
Neurocognitive Basis |
Forensic Consequence |
|
Confabulation |
Frontal lobe disinhibition |
False admissions |
|
Source misattribution |
Impaired hippocampal-prefrontal integration |
Inaccurate timelines |
|
Suggestibility |
Reduced executive monitoring |
Compliance with leading questions |
|
Emotional distortion |
Amygdala hyper-reactivity |
Exaggerated or dramatized accounts |
6.3 Suggestibility and Interrogator Bias
Interrogative suggestibility is defined as the extent to which individuals accept and incorporate misleading information during questioning (Gudjonsson, 2003). Pharmacological sedation enhances compliance and reduces resistance to authority.
Key Contributing Factors
Interrogator bias further compounds unreliability. Confirmation bias may shape question framing, influencing subject responses (Kassin et al., 2010). Under narcoanalysis, reduced cognitive defenses heighten susceptibility to such bias.
6.4 Lack of Reproducibility and Standardization
Scientific admissibility requires reproducibility and standardized methodology. Narcoanalysis protocols vary significantly in:
No universally accepted operating guidelines exist (NRC, 2003). Variability in pharmacokinetics and individual neurobiology further reduces consistency.
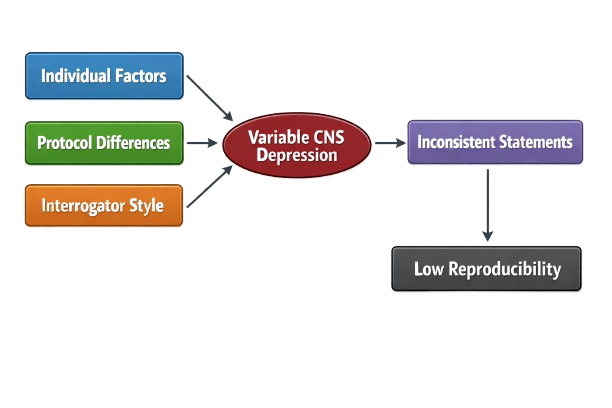
Figure 6.2. Variability in Narcoanalysis Outcomes
6.5 Comparison with Polygraph and Neuroimaging-Based Lie Detection
6.5.1 Polygraph Testing
The Polygraph measures autonomic responses (heart rate, respiration, galvanic skin response). While widely used, meta-analyses indicate substantial false-positive and false-negative rates (NRC, 2003).
6.5.2 fMRI-Based Lie Detection
Functional neuroimaging investigates deception-related activation in prefrontal and anterior cingulate cortices (Langleben et al., 2002; Spence et al., 2001). Commercial ventures (e.g., No Lie MRI) claim high accuracy, yet courts remain skeptical.
Compared to narcoanalysis, fMRI:
However, both methods face concerns regarding generalizability and individual variability.
6.6 Admissibility in Courts: Evidentiary Standards and Jurisprudential Challenges
6.6.1 Scientific Standards
Admissibility frameworks such as the Daubert standard (Daubert v. Merrell Dow Pharmaceuticals, 1993) require:
Narcoanalysis fails these criteria due to lack of standardized validation.
6.6.2 Constitutional Protections
In democratic legal systems, compulsory narcoanalysis raises concerns under protections against self-incrimination and coerced confession. In Selvi v. State of Karnataka (2010), the Supreme Court of India ruled involuntary narcoanalysis unconstitutional, citing violations of mental privacy and personal liberty.
6.6.3 International Human Rights Law
The United Nations Convention Against Torture prohibits coercive interrogation methods that impair autonomy. Sedative-facilitated questioning may be construed as psychological coercion.
6.7 Synthesis: Forensic Reliability Assessment
Table 6.2. Multidimensional Reliability Evaluation
|
Domain |
Assessment |
|
Biological plausibility |
Does not enhance truthfulness |
|
Cognitive integrity |
Impaired |
|
Reproducibility |
Low |
|
Error rate |
Unknown but high |
|
Legal admissibility |
Limited / Rejected |
|
Ethical acceptability |
Highly contested |
Barbiturate-based narcoanalysis lacks empirical validation, fails evidentiary standards, and presents significant risk of false or contaminated testimony.
7. Ethical, Legal, and Human Rights Considerations
Barbiturate-based narcoanalysis occupies a contested intersection between medicine, law enforcement, and human rights. Originally developed for therapeutic sedation, agents such as Sodium thiopental and Sodium amytal have been repurposed in some jurisdictions for investigative questioning. This transformation raises profound ethical, constitutional, and international law concerns.
7.1 Principles of Biomedical Ethics
The four foundational principles articulated by Beauchamp and Childress (2019)—autonomy, beneficence, non-maleficence, and justice—provide the core analytical framework for evaluating narcoanalysis.
7.1.1 Autonomy
Autonomy requires respect for an individual’s capacity for self-determination. Narcoanalysis directly interferes with cognitive liberty by pharmacologically altering consciousness to elicit disclosures.
Key concerns:
Bioethical scholarship emphasizes that autonomy includes the right to control one's thoughts and mental processes (Bublitz & Merkel, 2014). Sedative-facilitated interrogation intrudes upon this domain.
7.1.2 Beneficence
Beneficence requires that interventions promote the well-being of the subject. Narcoanalysis is not performed for therapeutic benefit but for investigative utility.
Ethical tension arises because:
Professional medical associations have historically warned against physician participation in coercive interrogation (World Medical Association, 2017).
7.1.3 Non-Maleficence
The duty to “do no harm” is central to medical ethics. Barbiturates carry risks of:
Administering sedatives outside therapeutic indication exposes subjects to medical risk without clinical justification.
7.1.4 Justice
Justice concerns equitable treatment and protection of vulnerable populations. Narcoanalysis is often applied to individuals in custodial settings, raising concerns of:
Custodial suspects represent a legally and psychologically vulnerable population (Gudjonsson, 2003).
7.2 Informed Consent Dilemmas
Informed consent requires:
Under custodial conditions, voluntariness is inherently compromised. Even when formal consent is obtained, implicit coercion may invalidate its ethical legitimacy (Appelbaum, 2007). Additionally, sedation itself impairs cognitive capacity, undermining contemporaneous consent during the procedure.
7.3 Coercion and Custodial Vulnerability
Interrogation settings amplify psychological vulnerability through:
The European Court of Human Rights has consistently held that evidence obtained through coercion violates fair trial guarantees (Jalloh v. Germany, 2006). Pharmacological disinhibition may constitute psychological coercion even absent physical force.
7.4 International Legal Frameworks
7.4.1 United Nations Human Rights Conventions
The United Nations framework provides several relevant protections:
Chemical interrogation techniques may fall within the scope of prohibited coercive practices if involuntary or harmful.
7.4.2 Constitutional Protections Against Self-Incrimination
Many democratic constitutions safeguard the right to silence.
Pharmacologically extracting statements challenges the voluntariness requirement central to these protections.
7.5 Landmark Judicial Decisions
Selvi v. State of Karnataka (2010)
In Selvi v. State of Karnataka (2010), the Supreme Court of India ruled involuntary narcoanalysis unconstitutional, holding that:
The Court emphasized cognitive liberty as integral to personal liberty.
Jalloh v. Germany (2006)
In this European Court of Human Rights case, forced administration of emetics to retrieve evidence was deemed a violation of Article 3 (prohibition of inhuman treatment), reinforcing the principle that bodily integrity and dignity are protected during criminal investigations.
7.6 Ethical Tension Between State Interests and Cognitive Liberty
Narcoanalysis highlights a broader jurisprudential conflict:
Modern human rights theory increasingly recognizes “cognitive liberty” as an extension of privacy rights (Bublitz & Merkel, 2014). Pharmacological interrogation intrudes directly into mental processes, raising unprecedented ethical implications.
8. Future Directions, Alternatives, and Policy Recommendations
The trajectory of barbiturate-based narcoanalysis reflects a broader historical arc—from therapeutic sedation to controversial investigative application. As forensic science increasingly embraces empirical validation and human rights–centered jurisprudence, the continued reliance on pharmacologically induced interrogation faces mounting scientific and ethical scrutiny. This section outlines emerging directions in evidence-based forensic neuroscience, non-pharmacological investigative tools, technological innovation, regulatory reform, and policy recommendations.
8.1 Shift Toward Evidence-Based Forensic Neuroscience
Modern forensic science emphasizes reproducibility, transparency, and peer-reviewed validation. The 2009 report by the National Academy of Sciences criticized several forensic practices for lacking rigorous empirical foundations (National Research Council, 2009). Narcoanalysis, lacking standardized protocols and validated accuracy rates, does not meet contemporary scientific benchmarks.
Key Requirements for Evidence-Based Forensic Methods:
Emerging research in cognitive neuroscience explores deception-related neural correlates using functional neuroimaging (Langleben et al., 2002). However, even advanced neurotechnologies remain subject to ecological validity limitations and interindividual variability.
8.2 Non-Pharmacological Investigative Tools
Given the medical and ethical risks associated with barbiturate-based interrogation, contemporary investigative psychology promotes non-coercive, cognitively informed interviewing techniques.
8.2.1 Cognitive Interview Techniques
The Cognitive Interview (CI) model emphasizes:
Meta-analyses indicate that CI increases accurate recall without proportionally increasing false memories (Memon et al., 2010).
8.2.2 Investigative Interviewing Frameworks
The PEACE model (Preparation and Planning, Engage and Explain, Account, Closure, Evaluate), adopted in the United Kingdom, rejects coercive interrogation in favor of rapport-based interviewing (Bull & Milne, 2004). This approach prioritizes reliability over confession-driven outcomes.
Table 8.1. Comparison of Investigative Approaches
|
Feature |
Narcoanalysis |
Cognitive Interview |
PEACE Model |
|
Pharmacological intervention |
Yes |
No |
No |
|
Risk of medical harm |
High |
None |
None |
|
Suggestibility risk |
High |
Controlled |
Controlled |
|
Legal admissibility |
Limited |
High |
High |
|
Ethical compatibility |
Contested |
Strong |
Strong |
8.3 Technological Advancements: AI-Assisted Behavioral Analysis
Artificial intelligence (AI) and machine learning systems are increasingly explored for behavioral pattern recognition in investigative contexts.
The European Commission has emphasized that AI systems used in law enforcement must comply with transparency, proportionality, and human oversight requirements (European Commission, 2021).
Potential Applications:
However, AI-assisted deception detection faces critical limitations:
Ethical AI governance frameworks, including those proposed by the OECD (OECD, 2019), stress accountability and rights-based safeguards.
8.4 Need for Standardized Ethical Guidelines
The transformation of medical tools into forensic instruments necessitates explicit professional boundaries.
Core Ethical Safeguards Should Include:
Professional bodies such as the World Medical Association emphasize that physicians must not participate in torture or coercive interrogation practices (WMA, 2017).
8.5 Policy Recommendations for Regulating or Prohibiting Narco Tests
Based on cumulative scientific and ethical analysis, the following policy pathways are recommended:
8.5.1 Regulatory Prohibition Model
8.5.2 Strict Regulatory Model (Where Not Fully Prohibited)
If jurisdictions do not impose a complete ban, minimal safeguards must include:
8.5.3 International Harmonization
Global alignment with:
8.6 Integration with Broader Forensic Reform
The 21st-century reform movement in forensic science emphasizes:
Narcoanalysis does not align with these reform principles and risks undermining the credibility of forensic systems.
8.7 Concluding Synthesis: From Therapeutic Sedative to Contested Forensic Tool
Barbiturates were developed as medical sedatives and anesthetics, functioning through potentiation of GABAergic inhibition. Their investigatory repurposing under the label of “truth serum” reflects a historical moment when neuropharmacology outpaced ethical governance.
Contemporary evidence demonstrates that:
The evolution of forensic science now favors non-coercive, empirically validated investigative methods. In this context, narcoanalysis represents a scientifically unsupported and ethically fraught relic of an earlier era.
The path forward requires alignment between neuroscience, law, and human rights—ensuring that investigative innovation respects cognitive liberty and evidentiary integrity.
REFERENCES

Pratyush Mishra, Ankita Vijay Thul, Sanjeev Kumar, Harjeet Singh, Geeta Rawat, Alka Mishra6, Rajeev Kumar, Yash Srivastav, Varaganti Sai Chitra Prathyusha, From Therapeutic Sedation to Investigative Intervention: An Integrative Review of the Neuropharmacology, Pharmacokinetics, Toxicological Risks, Ethical Constraints, and Forensic Reliability of Barbiturate-Based Narco Test Protocols., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 205-229. https://doi.org/10.5281/zenodo.18856728
 10.5281/zenodo.18856728
10.5281/zenodo.18856728
