Shri Swami Samarth Institute of Pharmacy, Malwadi, Bota, Sangamner, Ahmednagar, 422602
The body's endocrine glands secrete hormones, which are complex chemical messengers that are essential to many metabolic processes as well as a person's ability to procreate. Excessive or insufficient hormone imbalances can have serious effects on the entire body. Hormone levels usually fluctuate slightly as a result of aging. Adopting a variety of ways to increase cattle, dairy, poultry, and agricultural productivity has become essential due to the growing world population. Environmental deterioration has been exacerbated by the extensive use of pesticides, insecticides, herbicides, rodenticides, and a variety of other chemical agents due to this necessity. The general well-being of people is negatively impacted. The body's endocrine glands secrete hormones, which are complex chemical messengers that are essential to many metabolic processes as well as a person's ability to procreate. Excessive or insufficient hormone imbalances can have serious effects on the entire body. Hormone levels usually fluctuate slightly as a result of aging. Adopting a variety of ways to increase cattle, dairy, poultry, and agricultural productivity has become essential due to the growing world population. Environmental deterioration has been exacerbated by the extensive use of pesticides, insecticides, herbicides, rodenticides, and a variety of other chemical agents due to this necessity. The general well-being of people is negatively impacted by such, The Another significant concern is the prevalence of unemployment and the severe fight for livelihoods, which has created humans increasingly irritable and prone to stress, prompting modific.
Definition:
The Hormonal imbalance in women refers to a disruption in the normal production, secretion, or control of one or more hormones that are required for reproductive, metabolic, and general physiological health. It happens when hormones including estrogen, progesterone, androgens, thyroid hormones, insulin, or cortisol are either oversecreted (hyper-secretion) or undersecreted (hyposecretion). Menstrual cycle irregularities, infertility, weight swings, mood disorders, metabolic disorders, and an elevated risk of chronic conditions are all signs of this imbalance.
Key Hormonal Imbalances Affecting Women Concerning Cancer:
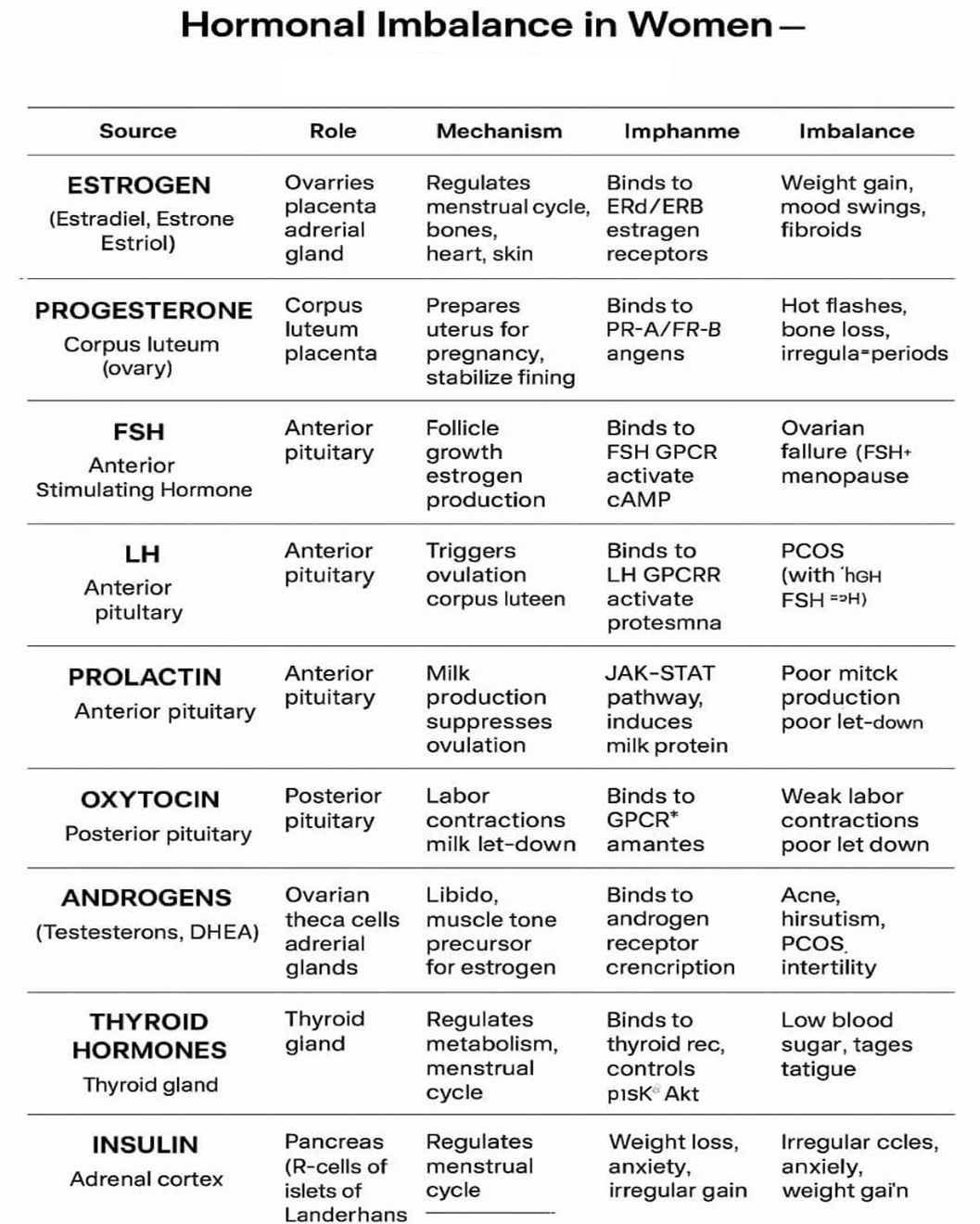
Estrogen, Progesterone, Testosterone, Follicle-Stimulating Hormone (FSH), Luteinizing Hormone (LH), Prolactin, Thyroid hormones, Cortisol, Insulin.
Common Symptoms:
Health Significance:
Overall Quality of life
1. Major Hormonal Control System — The HPO Axis :
Introduction: - The Hypothalamic–Pituitary–Ovarian (HPO) Axis is the key hormonal regulatory system that controls the menstrual cycle, ovulation, and fertility in women. It works like a communication network between the brain and the ovaries, ensuring that reproductive functions proceed in a normal cycle.
Step 1 — Hypothalamus : The hypothalamus is a region in the brain that works as the main controller of the endocrine system. It secretes a hormone known as GnRH Gonadotropin Releasing Hormone in pulses, which means that it is delivered in brief bursts as opposed to continually. These pulses are important because the following organ, the pituitary, reacts to the frequency and amplitude of GnRH pulses.
Step 2 — Anterior Pituitary Gland The anterior pituitary, located just below the brain, receives the GnRH signal. In response, it secretes two key reproductive hormones:
Step 3 — Ovarian Response The ovaries have special cells with receptors for FSH and LH. FSH acts mainly on granulosa cells → promotes follicle growth and estrogen production. LH acts mainly on theca and luteal cells → triggers ovulation and progesterone production. Together, these ovarian hormones — estrogen and progesterone — prepare the uterus for potential pregnancy.
Step 4 — Feedback Regulation Estrogen and Progesterone produced by the ovaries travel back to the hypothalamus and pituitary through the blood. They regulate their own production by feedback loops
Negative Feedback: When estrogen/progesterone levels are high, they suppress GnRH, FSH, and LH release → prevents overproduction.
Positive Feedback: Mid-cycle, a sudden rise in estrogen triggers an LH surge, which causes ovulation.
Function Summary:
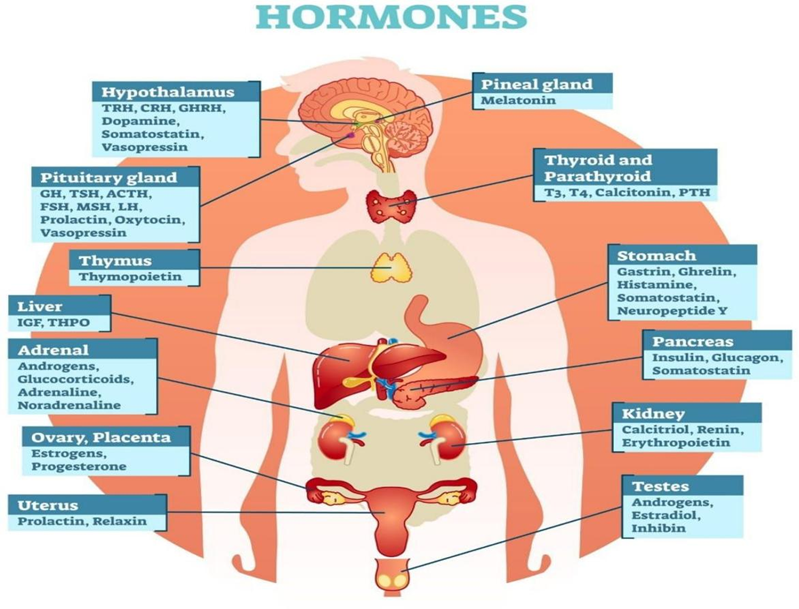
FIG NO .1.2
This image is a diagram of the human endocrine system, showing the major glands and the hormones, they produce. The endocrine system releases hormones into the bloodstream to regulate body functions such as growth, metabolism, stress response, reproduction, and sleep.
MECHANISM OF ACTION :
Summary:
|
Category |
Key Function |
|
HPO Axis Brain–Ovary communication controlling the cycle Estrogen & Progesterone |
Maintain uterus, bones, skin, pregnancy FSH & LH |
|
Prolactin & Oxytocin |
Milk production and childbirth |
|
Thyroid, Insulin, Cortisol |
Indirectly influence reproductive health metiram for implantatin |
Pathophysiology of hormonal imbalance for concern woman:
A. Hypothalamic–Pituitary–Gonadal (HPG) Axis Dysfunction: GnRH (gonadotropin-releasing hormone) is released by the hypothalamus, which stimulates the pituitary gland to release FSH and LH and acts on the ovaries to create progesterone and estrogen. Disruption at any level (hypothalamus, pituitary, or ovary) can produce hormonal imbalance. For instance, stress, eating disorders, or intense physical activity decrease GnRH → FSH/LH → estrogen and progesterone → irregular menstruation or amenorrhea.
C. Adrenal Gland Imbalance: Cortisol and androgens produced by the adrenal glands affect reproductive hormones. Chronic stress → ↑ cortisol → suppresses GnRH and LH → menstrual irregularities. Congenital Adrenal Hyperplasia (CAH): excess adrenal androgens → masculinization and menstrual disturbance.
D. Thyroid Hormone Imbalance: Thyroid hormones interact with sex hormones: Hypothyroidism: ↑ TRH → ↑ prolactin → inhibits GnRH → anovulation and amenorrhea. Hyperthyroidism: ↑ SHBG (sex hormone–binding globulin) → altered estrogen and testosterone levels → menstrual changes.
Clinical Manifestations in hormonal imbalance for concern woman:
Common Conditions Involving Hormonal Imbalance:
|
Condition |
Key Hormonal Changes |
Main Effects |
|
PCOS |
↑ LH, ↑ androgens, ↓ FSH |
Anovulation, infertility, hirsutism |
|
Hypothyroidism |
↓ T3/T4, ↑ TRH, ↑ prolactin |
Irregular menses, fatigue |
|
Hyperparathyroidism |
↑ Prolactin |
Amenorrhea, galactorrhea |
|
Premature Ovarian Insufficiencies |
↓ Estrogen, ↑ FSH/LH |
Early menopause symptom |
|
Cushing’s Syndrome |
↑ Cortisol |
Menstrual irregularity, weight gain |
|
Menopause osteoporosis |
↓ Estrogen, ↓ Progesterone |
Hot flashes |
The primary systems involved are:
The hypothalamus secretes gonadotropin releasing hormone (GnRH) in pulses.
GnRH stimulates the anterior pituitary to release FSH (follicle-stimulating hormone) and LH (luteinizing hormone). FSH and LH act on the ovaries Hormonal imbalance in women (PCOS, menopausal transition, thyroid disorders, metabolic/endocrine cross-talk), plus a one-paragraph summary of each paper’s mechanistic.
Polycystic Ovary Syndrome — comprehensive reviews (pathophysiology & mechanisms)
Mechanism summary: PCOS arises from a complicated combination of insulin resistance, adiposity- caused inflammation, and hypothalamic–pituitary–ovarian (HPO) axis dysfunction leading to increased ovarian Andro This image illustrates a representation of the human endocrine system, depicting the major glands and the hormones, they make. The endocrine system sends hormones into the bloodstream to govern physiological activities such as growth, metabolism, stress response, reproduction, and sleep.
Hormonal changes during menopause — Mechanism summary:
Hormonal changes during menopause — Mechanism summary: Menopause is caused by ovarian follicular depletion, which lowers estradiol and inhibit levels; lack of negative feedback increases FSH and modifies autonomic regulation, systemic metabolism (lipids, endothelial function), and vasomotor, cardiovascular, and bone consequence.
Thyroid disorders and female reproductive health — mechanistic: Mechanism summary: Thyroid hormones modulate gonadotropin releasing hormone (GnRH) pulse patterns, SHBG, and ovarian steroid metabolism. Hypothyroidism and hyperthyroidism can cause menstrual irregularities, infertility, and altered pregnancy outcomes via direct effects on ovarian function and indirect metabolic/vascular actions Hypothyroidism and hyperthyroidism can cause menstrual abnormalities, infertility, and altered pregnancy outcomes by direct impacts on ovarian function and indirect metabolic/vascular action.
Metabolic hormones and female reproductive regulation: According to Athar F. et al., metabolic hormones are essential regulators of female Mechanism summary: Leptin, insulin, adipokines and gut hormones convey nutritional status to the hypothalamus and pituitary; perturbations (e.g., obesity, insulin resistance) perturb GnRH/LH pulses and ovarian receptivity, linking metabolic disease to reproductive hormonal imbalance. The majority of female hormonal imbalances are complex, involving peripheral gland dysfunction (ovary, thyroid, adrenal) + metabolic status (insulin, adipokines) + central (hypothalamic/pituitary) alterations. Reproductive hormone signaling is disrupted and androgen excess (PCOS) is amplified by insulin resistance and adipose-driven inflammation. Menopausal hormonal changes (estrogen/inhibit → FSH) are caused by ovarian follicle depletion and loss of ovarian endocrine feedback. Peripheral steroid metabolism and central neuroendocrine rhythms are two ways that thyroid hormones impact reproduction.
Diagnosis involves a combination of clinical evaluation, lab tests, and sometimes imaging:
Treatment of hormonal imbalance:
Treatment depends on the cause and specific hormones involved:

Fig no 1.3] Hormone balancing food wheel
When to See a doctor:
CONCLUSION:
Hormonal imbalance in women is a complex illness with major implications for physical, mental, and reproductive health. It may show through menstrual irregularities, infertility, metabolic issues, mental disturbances, and long- term dangers such as osteoporosis and cardiovascular disease. Early detection and appropriate evaluation are critical for prompt intervention. Lifestyle adjustments, pharmaceutical therapy, and tailored care techniques can help restore hormonal balance and improve quality of life. Continued research and patient-centered education remain necessary to raise awareness, maximize treatment.
REFERENCES


Pranali Wagh, Akash Shelke, Harmone Imbalance A Cause for Concern in Women, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 2065-2072. https://doi.org/10.5281/zenodo.17909518
 10.5281/zenodo.17909518
10.5281/zenodo.17909518
