1,2,3,5 S.N.D College of Pharmacy, Babhulgaon
4 Sayali Charitable Trust’s College of Pharmacy
Dysmenorrhea, also known as menstruation discomfort, affects more than 70% of reproductive-age women worldwide, considerably impairing their quality of life and everyday function. Current treatment options rely mostly on nonsteroidal anti-inflammatory medicines (NSAIDs), which provide symptom relief but are frequently linked with gastrointestinal discomfort, renal side effects, and hormone imbalance with prolonged usage. There is an increasing need for natural, safer, and more patient-friendly options. Herbal antispasmodics like Zingiber officinale (Ginger), Foeniculum vulgare (Fennel), and Valeriana officinalis (Valerian) have demonstrated effective outcomes in alleviating uterine spasms and inflammation by inhibiting COX enzymes and promoting smooth muscle relaxation, as evidenced by clinical studies and meta-analyses. At the same time, magnesium, a vital mineral, has shown effectiveness in easing menstrual pain by influencing prostaglandin production and calcium ion movement, thus relaxing uterine muscles and reducing cramps. Effervescent tablets present an innovative drug delivery system that guarantees quick onset of effects, better bioavailability, pleasant taste, and increased patient adherence, particularly during episodes of acute pain. The use of magnesium combined with standardized herbal antispasmodic agents in an effervescent tablet form has not been investigated in current market offerings, rendering this method both novel and commercially viable. This analysis examines the scientific foundation, pharmacological principles, formulation approaches, an current market scenario for this new herbal-magnesium effervescent dosage form, setting the stage for future investigations, product innovation, and potential nutraceutical or AYUSH-oriented commercialization.
Dysmenorrhea:-
Dysmenorrhea, commonly known as menstrual discomfort or cramps, is one of the most widespread gynecological issues that affects women of reproductive age. It is marked by cramping pain in the lower abdomen, often accompanied by symptoms such as nausea, fatigue, headaches, diarrhea, and mood swings, which can significantly affect daily activities and overall quality of life. It is estimated that worldwide, more than 70% of adolescent and young adult females experience dysmenorrhea, with varying levels of intensity and recurrence.(1)
Dysmenorrhea is broadly classified into two types:-
Primary dysmenorrhea is characterized by menstrual pain without any detectable pelvic condition. It generally starts in adolescence, a few years after the onset of menstruation, and is thought to be linked to an excess production of uterine prostaglandins, especially prostaglandin F2α (PGF2α). These prostaglandins lead to strong uterine contractions, diminish uterine blood flow (causing ischemia), and heighten the perception of pain. Elevated levels of prostaglandins can also lead to systemic symptoms such as diarrhea and nausea.(2)
Secondary dysmenorrhea arises from existing pelvic or reproductive system disorders, including endometriosis, adenomyosis, pelvic inflammatory disease (PID), fibroids, or the use of intrauterine devices (IUDs). It usually develops later in life and tends to escalate if the underlying issue remains unaddressed.(2)
The pathophysiology of dysmenorrhea is characterized by a complex interaction of hormonal, inflammatory, and neurological components. A decrease in progesterone levels before menstruation triggers the shedding of the endometrium, resulting in the release of arachidonic acid, which starts the production of prostaglandins and leukotrienes. These biochemical agents increase uterine tone, cause hypercontractility, and amplify pain sensitivity by activating peripheral pain receptors and pathways within the central nervous system.(2)
Factors that also contribute to dysmenorrhea include:-
This review examines an innovative method for managing dysmenorrhea by combining herbal antispasmodics with magnesium in an effervescent tablet formulation, providing a quicker-acting, natural, and user-friendly solution for menstrual pain relief.
Enhanced Section: Global Burden & Lifestyle Impact of Dysmenorrhea:-
Dysmenorrhea is not only common in medical settings but also has significant social ramifications. It impacts 45–95% of menstruating women worldwide, with the highest occurrence noted among adolescents and young adults. A survey in India indicated that over 72% of college-aged women suffer from moderate to severe menstrual pain, often resulting in missed school, college, or workdays, as well as a notable decline in productivity and concentration.(3)
Research from Japan found that one-third of women experiencing dysmenorrhea miss at least one day of work each month, and the situation is even more critical in developing nations due to inadequate access to pain relief and menstrual hygiene products.(4)
Additionally, lifestyle elements such as unhealthy diets, stress, insufficient physical activity, and irregular sleep patterns have been shown to exacerbate the severity and duration of menstrual cramps. Women who lead sedentary lifestyles, experience high levels of anxiety, or have low magnesium intake are particularly vulnerable to more intense symptoms.(5)
The effect of lifestyle on dysmenorrhea:-
Specifically, a lack of physical activity can lead to uterine ischemia and reduced blood flow in the pelvic area, while elevated stress levels can increase cortisol, heightening pain sensitivity through inflammation. A study conducted by Unsal et al. (2010) found that students who engaged in unhealthy habits, such as skipping meals and poor sleep practices, reported significantly greater menstrual pain compared to those who led more balanced lifestyles. These results suggest that comprehensive management of dysmenorrhea should encompass not just medication for relief, but also lifestyle modifications as a preventive approach.(6)
Scientific Basis for Herbal and Magnesium Use:-
The use of herbal antispasmodics and magnesium for treating dysmenorrhea is supported by growing pharmacological and clinical research. For instance, Zingiber officinale (ginger) inhibits cyclooxygenase (COX) enzymes, mimicking the action of NSAIDs but without adverse effects on the stomach. Foeniculum vulgare (fennel) works through phytoestrogens and facilitates smooth muscle relaxation, whereas Valeriana officinalis acts centrally as a GABA agonist to alleviate cramps linked to anxiety.
Magnesium operates at a neuromuscular level by decreasing intracellular calcium and reducing uterine hypercontractility. A randomized placebo-controlled trial conducted by Ziaei et al. (2001) found that magnesium supplementation notably decreased pain intensity scores over two consecutive menstrual cycles. Consequently, these substances provide complementary mechanisms—anti-inflammatory, antispasmodic, and muscle-relaxant—making them potential candidates for combination therapy.(7)
Necessity for Innovative Formulation Methods:-
Even though there is growing awareness around menstrual health, the majority of existing pharmaceutical and herbal solutions for dysmenorrhea continue to depend on traditional dosage forms like capsules, syrups, and tablets, which frequently face issues related to delayed onset, poor taste, or gastrointestinal discomfort. Furthermore, a significant number of patients favor non-hormonal, plant-based alternatives; however, the current market lacks rapid-acting, user-friendly solutions tailored for menstrual pain relief.
Effervescent tablets present an innovative solution. They facilitate quick disintegration and absorption, providing faster relief and better adherence from patients, particularly during intense pain episodes. A 2020 review by Kalita et al. highlighted that effervescent delivery systems enhance both pharmacological efficacy and patient satisfaction, especially in situations requiring immediate action, such as spasmodic or musculoskeletal pain. The combination of standardized herbal antispasmodics with magnesium in this format has yet to be commercialized, making this formulation a unique and viable concept in the realm of menstrual wellness.(8)
Pathophysiology of Dysmenorrhea:-
Primary dysmenorrhea is characterized by painful menstruation that occurs without any underlying pelvic conditions. It usually affects young women, particularly adolescents, and is strongly associated with hormonal fluctuations that trigger a series of uterine and neurochemical responses leading to discomfort.
Towards the conclusion of the luteal phase, levels of progesterone decrease, prompting endometrial cells to release arachidonic acid, which is then transformed into prostaglandins (PGF?α and PGE?) through the cyclooxygenase (COX) pathway. The rise in prostaglandins heightens uterine contractions, diminishes blood circulation, and increases the sensitivity of pain receptors. (9) Women experiencing dysmenorrhea have prostaglandin levels in menstrual fluid that are 3–4 times higher than those who do not have pain.(10)
Heightened levels of PGF?α lead to forceful, frequent, and disorganized uterine contractions, resulting in increased intrauterine pressure. This elevation causes vasoconstriction of spiral arteries, leading to diminished blood supply to the uterus, which induces ischemia and discomfort. The ischemic effects are similar to angina-like chest pain in terms of mechanism, as both scenarios initiate anaerobic metabolism and the accumulation of lactic acid.(11)
Some women experience elevated levels of vasopressin, a hormone that encourages vasoconstriction in the uterus and increases the activity of PGF?α. Leukotrienes, particularly LTC? and LTD?, are generated via the lipoxygenase pathway and play a role in smooth muscle contraction and inflammation, especially in women who do not respond well to NSAIDs.(12,13)
Frequent intense contractions and episodes of ischemia can lead to hyperalgesic priming, where peripheral nociceptors become overly sensitive. Over time, central sensitization develops, resulting in structural alterations in brain regions that regulate pain, causing even slight uterine contractions to be perceived as painful.(11)
This type results from pathological conditions such as endometriosis, adenomyosis, fibroids, or pelvic inflammatory disease. These conditions lead to abnormal growth of endometrial or uterine tissue, increased inflammation, and pain that may begin earlier and last longer than typical menstrual cramps.(14)
Herbal Antispasmodics for Managing Dysmenorrhea:-
Table.1 Commonly studied herbal antispasmodics, their active constituents, and mechanisms of action.
|
Sr. No. |
Common name |
Botanical name |
Active constituent |
Mechanism of action |
Reference |
|
1. |
Ginger |
Zingiber officinale |
Gingerols, Shogaols |
Inhibits COX and LOX → reduces prostaglandin synthesis → ↓ uterine contractions |
Ozgoli et al., 2009; Rahnama et al., 2012; Daily et al., 2015 |
|
2. |
Fennel |
Foeniculum vulgare |
Anethole, Fenchone, Estragole |
Phytoestrogenic effect; inhibits uterine contractions by blocking oxytocin receptors |
Modarres et al., 2011; Delaram et al., 2011 |
|
3. |
Valerian |
Valeriana officinalis |
Valerenic acid, Iridoids, Flavonoids |
Modulates GABA receptors → muscle relaxant and CNS calming effect |
Mirabi et al., 2011; Sadeghi Aval et al., 2014 |
|
4. |
Chamomile |
Matricaria chamomilla |
Apigenin, Bisabolol, Flavonoids |
Anti-inflammatory, COX-2 inhibition, mild sedative; relieves cramps and mood swings |
Sharifi et al., 2014; Srivastava et al., 2010 |
|
5. |
Peppermint |
Mentha piperita |
Menthol, Menthone, Flavonoids |
Calcium channel blocker; antispasmodic effect on uterine and intestinal smooth muscle |
Nahidi et al., 2009; Uritu et al., 2021 |
Dysmenorrhea, especially its primary type, is often linked to heightened uterine contractions driven by increased prostaglandin levels, which lead to ischemia and pain. A range of natural agents known as herbal antispasmodics show promise in alleviating this condition by influencing smooth muscle tone, decreasing inflammation, and regulating hormonal responses. These herbs have a strong reputation in various traditional medical systems, including Ayurveda, Persian, and Chinese medicine, and are gaining more backing from clinical studies and scientific research.
Mechanisms of Action:-
Herbal antispasmodics exert their effects through various pharmacological pathways:
Commonly Studied Herbal Antispasmodics:-
Ginger is among the most extensively researched herbal remedies for dysmenorrhea. Its primary active compounds, gingerols and shogaols, work by inhibiting the production of prostaglandins through COX and LOX pathways, which helps to alleviate uterine spasms.
Clinical Support:-
In a randomized controlled trial, ginger (250 mg taken four times daily) demonstrated effectiveness comparable to that of mefenamic acid and ibuprofen in diminishing the intensity of menstrual pain (Ozgoli et al., 2009). A meta-analysis conducted by Daily et al. (2015) further validated the effectiveness of ginger in various RCTs.l

Fig.2 Ginger (Zingiber officinale)
Fennel contains anethole, a compound with estrogenic properties that also inhibits uterine muscle contractions by acting on oxytocin receptors and calcium channels.
Clinical Support:-
Modarres et al. (2011) found fennel extract (30 drops every 4 hours) significantly reduced menstrual pain intensity compared to placebo. It also improved associated symptoms like bloating and nausea.

Fig.3 Fennel (Foeniculum vulgare)
Valerian exerts a GABAergic effect, promoting central and peripheral muscle relaxation. Its components such as valerenic acid reduce uterine spasms through modulation of GABA-A receptors.
Clinical Support:
A double-blind RCT showed that valerian significantly reduced pain severity in young women over two menstrual cycles (Mirabi et al., 2011). Sadeghi Aval et al. (2014) also noted reduced reliance on rescue analgesics in valerian users.

Fig.4 Valerian (Valeriana officinalis)
Chamomile is rich in apigenin and bisabolol, which are flavonoids that have anti-inflammatory properties and mild sedative effects. These compounds inhibit the release of prostaglandins and decrease the contractions of the uterus.
Clinical Evidence:
According to Sharifi et al. (2014), women who drank chamomile tea during their menstrual periods experienced significantly reduced pain and improved emotional health. The effectiveness of chamomile was found to be similar to that of NSAIDs, but with fewer side effects.

Fig.5 Chamomile (Matricaria chamomilla)
Peppermint oil is rich in menthol, which acts as a calcium channel blocker, thereby relaxing uterine and gastrointestinal smooth muscles. Though more commonly used for IBS, it shows potential in dysmenorrhea.
Clinical Support:
A small RCT by Nahidi et al. (2009) indicated that peppermint significantly reduced dysmenorrhea scores in students after one cycle of use.

Fig.6 Peppermint (Mentha piperita)
Role of Magnesium in Dysmenorrhea Management:-
Magnesium is essential for neuromuscular functioning, vascular regulation, and balancing prostaglandins, all of which are significant in the development of dysmenorrhea. Its role as a natural antagonist to calcium helps to alleviate uterine muscle contractions, while its properties that reduce inflammation and promote blood vessel dilation aid in relieving pain.
Mechanism of Action
Clinical Evidence
Critical Assessment of Clinical Trials :-
Although the clinical studies analyzed show favorable results for both herbal remedies and magnesium in treating dysmenorrhea, several limitations are significant. Numerous trials have small participant numbers, brief durations (1–2 menstrual cycles), or lack a placebo comparison, which could influence the statistical reliability. For example, the magnesium study conducted by Ziaei et al. (2001) was encouraging but only involved 50 subjects. Likewise, studies on valerian and chamomile do not maintain consistency in extract dosages and types of formulations. These deficiencies stress the necessity for widespread, multicentric studies to validate effectiveness, refine dosages, and assess against conventional NSAIDs.
A recent meta-analysis reaffirmed that ginger is comparably effective as NSAIDs while resulting in fewer gastrointestinal issues (Daily et al., 2020). Another review emphasized the potential of herbs from the Lamiaceae family, such as peppermint, in managing pain, supporting their use in treating dysmenorrhea (Uritu et al., 2021). Furthermore, a double-blind randomized trial found that magnesium supplementation significantly alleviated pain intensity and enhanced mood scores among teenagers experiencing primary dysmenorrhea (Shahnazi et al., 2022). (15)
Commercial Herbal Products for Dysmenorrhea:-
Several herbal formulations are presently sold in both Indian and international markets for alleviating primary dysmenorrhea and menstrual discomfort. These products typically incorporate herbs known for their antispasmodic, anti-inflammatory, or hormonal-balancing properties. They come in various forms such as capsules, syrups, teas, tonics, and granules; however, the absence of effervescent tablets indicates an opportunity for your formulation concept to fulfill this gap.
Tabel.2 Marketed herbal formulations for menstrual pain relief.
|
Sr.No |
Brand Name |
Manufacturer |
Formulation |
Key Herbal |
Claim/Use |
|
1. |
EveCare |
Himalaya Wellness |
Syrup/ Capsule |
Ashoka (Saraca indica), Lodhra (Symplocos racemosa), Dashamoola |
Menstrual regulation, relief from cramps |
|
2. |
MyTanix Syrup |
Aimil Pharmaceuticals |
Syrup |
Shatavari, Ashoka, Lodhra, Guduchi |
Relieves pain, regulates cycles |
|
3. |
Femiza Tablets |
Solumiks Herbaceuticals |
Tablet |
Shatavari, Ashoka, Lodhra, Nagarmotha |
Supports uterine health, manages pain |
|
4. |
Gynocare Capsules |
Ayusya Naturals |
Capsule |
Lodhra, Ashoka, Shatavari, Kumari |
Alleviates menstrual discomfort |
|
5. |
Herbocare Dysmeno |
Morpheme Remedies |
Capsule |
Ginger, Fennel, Chamomile, Valerian |
Natural pain relief from cramps and bloating |
|
6. |
MenstCare Herbal Tea |
Tea Treasure Herbal |
Tea |
Hibiscus, Chamomile, Fennel, Peppermint |
Relaxing tea to reduce spasms and irritability |
|
7. |
Moha Pain Oil |
Charak Pharma |
Topical Oil |
Nirgundi, Eucalyptus, Pudina, Ajwain |
Applied topically to ease menstrual cramps |
Global Strategies for Herbal Treatment of Dysmenorrhea:
Across various cultures, herbal treatments for dysmenorrhea differ according to their traditional medical practices. In Traditional Chinese Medicine (TCM), Angelica sinensis and Chuanxiong are frequently utilized to enhance circulation and alleviate stagnation. Iranian traditional medicine highlights Zataria multiflora, fennel, and cinnamon, with multiple clinical studies affirming their antispasmodic properties. European herbal medicine, particularly in Germany, often incorporates Valerian, Chamomile, and Melissa officinalis, which are regulated by the German Commission E Monographs. These international approaches emphasize the cross-cultural acknowledgment of herbal methods and support the idea of innovative delivery systems such as effervescent tablets.
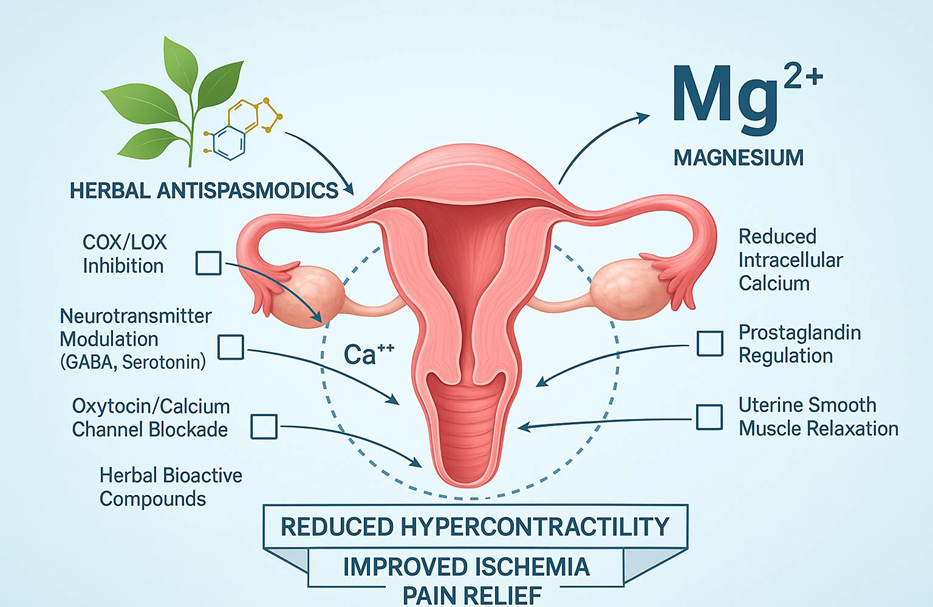
Fig.7 Synergistic role of herbal antispasmodics and magnesium in Reducing uterine hypercontractility and menstrual pain.
Benefits of Merging Herbal Antispasmodics with Magnesium for Managing Dysmenorrhea:
The simultaneous use of herbal antispasmodics and magnesium creates a synergistic and multi-faceted approach to address primary dysmenorrhea. Each element offers unique pharmacodynamic effects that, when combined, may deliver better therapeutic results with fewer adverse effects compared to traditional NSAIDs.
1. Complementary Antispasmodic Effects
Herbal remedies such as ginger, fennel, and valerian alleviate uterine muscle contractions by suppressing prostaglandin production or modulating GABAergic transmission. Magnesium acts as a calcium channel blocker, promoting relaxation of the uterine muscles.(16,17)
2. Combined Anti-Inflammatory Actions
Both herbal ingredients (e.g., chamomile, ginger) and magnesium work to inhibit inflammatory mediators:
3. Nutraceutical Synergy
While herbal medicines offer active relief, magnesium addresses micronutrient deficiencies by supporting:
4. Enhanced Safety and Tolerability
In comparison to NSAIDs, this combination is:
5. Increased Compliance through Effervescent Format
Effervescent tablets can:
Table3.Compared to conventional NSAIDs, herbal antispasmodics combined with magnesium offer a safer, Hormone-free, and patient-friendly option for dysmenorrhea management
|
Parameter |
NSAIDs(Conventional) |
Herbal Antispasmodics+ Magnesium (Prosposed) |
|
Mechanism |
Inhibit COX enzymes → ↓ prostaglandins |
Herbs: COX inhibition, oxytocin/GABA modulation, anti- inflammatory; Magnesium: calcium channel blockade, ↓ PGF?α |
|
On set of action |
Fast (30–60 min) |
Moderate (herbs slower, magnesium faster when combined) |
|
Side effect |
GI irritation, ulcers, renal risk, hormonal imbalance (long-term) |
Minimal GI effects, hormone-free, nutrient support |
|
Safety |
Long-term risks |
Generally safe, well tolerated |
|
Patient compliance |
Moderate (bitter, requires food) |
Better (natural, holistic, fewer side effects) |
|
Innovation |
Conventional |
Integrative & novel |
Patient-Centered Perspective:-
Adherence to treatment is a crucial factor influencing the success of therapy. Research indicates that women, particularly adolescents and young adults, often favor natural, hormone-free solutions for menstrual discomfort because of their worries about the long-term safety of NSAIDs and hormonal contraceptives. Interventions that are pleasant in taste, easy to administer, and holistic tend to enhance both compliance and overall satisfaction.(12,13)
Challenges and Limitations of Herbal Formulations for Dysmenorrhea:-
Despite the encouraging effectiveness of herbal remedies in alleviating menstrual discomfort, various obstacles impede their widespread acceptance, large-scale clinical validation, and consistent therapeutic outcomes. It is essential to recognize these challenges when contemplating the incorporation of herbal antispasmodics into contemporary dosage forms such as effervescent tablets.
The active ingredient content in herbal extracts can differ considerably due to variations in plant origin, timing of harvest, extraction methods, and storage conditions. This inconsistency affects the potency, safety, and clinical effectiveness.(22)
While many herbs have traditional and empirical backing, only a few have been subjected to expansive, multicentric randomized controlled trials to confirm their efficacy and safety for treating primary dysmenorrhea. Small participant numbers and the absence of placebo controls diminish the reliability of many current studies.(23)
Numerous herbs can interact with prescribed medications through enzyme inhibition or activation (e.g., CYP450). This is particularly concerning for people simultaneously taking NSAIDs, hormonal contraceptives, or anticoagulants during their menstrual cycle.(24)
In comparison to synthetic pain relievers like ibuprofen or mefenamic acid, herbal formulations may require longer to produce discernible effects due to slower pharmacokinetics and lower bioavailability in plasma.(25)
Herbal formulations generally fall under less rigorous regulatory categories (such as nutraceuticals or supplements), leading to variability in product quality, claims, and safety information, unlike synthetic drugs.(26)
Many herbal extracts have a bitter flavor, are poorly soluble, or may be unstable in watery or effervescent bases, presenting challenges in formulation. Stabilizers or taste-masking agents might be necessary, particularly in innovative delivery forms like effervescent tablets.(27)
Literature Gaps and Opportunities for Future Reviews:-
Future Perspectives and Broader Considerations:-
The combination of herbal antispasmodics and magnesium in an effervescent dosage form represents an innovative and patient-focused method for managing dysmenorrhea. Although this idea has not yet been commercialized, it paves the way for several future advancements:
CONCLUSION:
Dysmenorrhea continues to be a significant clinical and quality-of-life issue for women worldwide, typically managed with NSAIDs and hormonal therapies that may produce unwanted side effects. This review underscores the potential therapeutic benefits of herbal antispasmodics like ginger, fennel, valerian, and chamomile, alongside the vital mineral magnesium, which offer diverse mechanisms such as prostaglandin inhibition, muscle relaxation, and anti-inflammatory properties.
The Idea of merging these components into a single effervescent tablet offers a novel and patient-friendly strategy with the capability to improve the speed of action, taste, and adherence, particularly among younger women. Although the formulation has yet to be created, this concept introduces an encouraging path for forthcoming research and innovation.
Nevertheless, existing literature highlights significant gaps, such as the lack of standardized herbal preparations, a shortage of large-scale trials, and no combination studies involving both herbal and mineral agents in advanced delivery systems. Addressing these shortcomings through well-structured clinical investigations and formulation research will be crucial in translating this novel idea into a safe, effective, and commercially feasible solution for menstrual health.
REFERENCES


Pranav Sonawane, Sayli Patil, Vaishnavi Khilari, Vaishnavi Tanpure, Shraddha Shinde, Herbal Antispasmodics with Magnesium: A Novel Approach to Dysmenorrhea Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 3407-3420. https://doi.org/10.5281/zenodo.17493598
 10.5281/zenodo.17493598
10.5281/zenodo.17493598
