Shri Venkateshwara College of Pharmacy. Ariyur..
Mucositis is a painful inflammatory condition of the mucosal lining, most commonly associated with chemotherapy and radiotherapy in cancer patients. It significantly compromises nutrition, speech, and overall quality of life, and may necessitate interruption of anticancer therapy. Conventional treatments provide symptomatic relief but are often limited by cost and adverse effects. Herbal gel formulations have emerged as promising alternatives due to their anti-inflammatory, antioxidant, antimicrobial, and wound-healing properties. This review discusses the pathophysiology of mucositis, herbal agents used in gel formulations, formulation strategies, and evaluation parameters for herbal gels intended for mucosal application.
Mucositis is a painful inflammatory condition that occurs in the mucous membranes lining the oral cavity and extending throughout the entire gastrointestinal (GI) tract. However, it most commonly affects the digestive system, particularly the oral region.
Mucositis is primarily caused by cancer treatments such as chemotherapy and radiotherapy. These therapies target rapidly dividing cells, including not only cancer cells but also the epithelial cells lining the mucous membranes. As a result, damage to the mucosal tissue occurs, especially during chemotherapy and radiotherapy. The initial stage of injury triggers the regulation of various genes, leading to the release of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6). The release of these inflammatory mediators, along with reactive oxygen species (ROS), further exacerbate tissue injury and ultimately leads to breakdown of the mucosal barrier.
This process results in the formation of painful ulcers. Subsequently, proliferation of epithelial cells occurs to cover the ulcerated areas, leading to gradual healing. Oral mucositis is the most common and extensively studied form of this condition. The main clinical features include redness and swelling of the affected mucosa. Patients often experience significant pain and discomfort, commonly described as a burning sensation, which can interfere with eating, speaking, and swallowing. Additionally, the ulcerated mucosa serves as a portal of entry for pathogens, increasing the risk of secondary bacterial, viral, or fungal infections.1
Mucositis

Fig no: 1 Mucositis
Signs and symptoms of mucositis are:
Red, shiny, or swollen mouth and gums.
Blood in the mouth.
Sores in the mouth, on the gums, or tongue.
Pain in the mouth or throat.
Having a hard time swallowing or talking.
Feeling dry in your mouth, mild burning, or pain when eating food.
Soft, whitish patches or pus in the mouth or on the tongue.
More mucus or thicker saliva in the mouth.
Risk factors
The development of mucositis is influenced by the intensity, timing, and type of cancer treatment administered. Several treatment-related risk factors have been identified, including the dosage and timing of systemic cytotoxic medications, radiation field, radiation dose, and the co-administration of chemotherapy and radiotherapy. However, some risk factors remain poorly understood.
Patients receiving high-dose chemotherapy, particularly for cancers of the head and neck, gastrointestinal tract, hematologic malignancies, and pelvic region, are at a higher risk of developing severe mucositis. In contrast, patients undergoing reduced-intensity hematopoietic stem cell transplantation generally experience a less severe form of mucositis, although the condition is still commonly observed.
Despite increased awareness and preventive strategies, patients receiving combined cancer treatment modalities remain at high risk for mucositis development. Consequently, cancer therapy continues to be a significant and persistent risk factor for mucositis.
Epidemological
Between 20% and 40% of patients with solid tumors receiving chemotherapy develop mucositis, typically within 5–14 days of treatment initiation.[8] The incidence and severity vary depending on the chemotherapeutic agent used, cumulative dose, number of treatment cycles, and individual patient factors.[5] Patients undergoing myeloablative conditioning for hematopoietic stem cell transplantation have a particularly high incidence of oral mucositis.[9]
One study reported a 76% risk of mucositis in patients receiving high-dose chemotherapy or bone marrow transplantation. Radiation-induced oral mucositis occurs in nearly 100% of head and neck cancer patients receiving altered fractionation radiotherapy. [10] The risk of mucositis is increased in patients with poor nutritional status and inadequate oral hygiene. Younger patients may also have a higher incidence of oral mucositis.
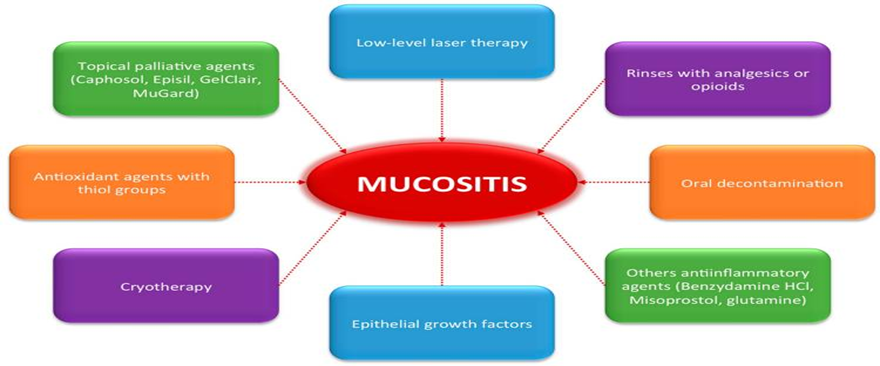
Fig No: 2 Actual strategies for managing oral mucositis
Oral mucositis Preventative:
In some cases, it may not be possible to stop mucositis from occurring, but there are steps you can take before beginning radiation or chemotherapy treatment to help alleviate its side effects and symptoms:
Speak to your doctor
Maintain a good oral care regimen
Avoid products that irritate the gums & mouth, such as products containing alcohol
Increase your fluid intake
Stop smoking
Moisturise your lips
brush twice daily with a soft toothbrush,
use alcohol-free mouth rinses (like baking soda/saline),
avoid tobacco/alcohol, and maintain high hydration
Avoid: Petroleum-based products (like Vaseline) on lips, as they can promote infection.
Consistency: Daily care is crucial; once mucositis starts, it is harder to treat.
MATERIAL AND METHODS
Chinese Woad

Fig no: 3 Isatis indigotica
Table: 1 Taxonomical classification of Isatis indigotica
|
Common name |
: Ban-lan-gen, Chinese Woad |
|
Habit |
Biennial herb |
|
Botanical name |
Isatis indigotica |
|
Family : |
Brassicaceae (Cruciferae) |
|
Size: |
Generally, the root is 10–20 cm long and 0.5–2 cm in diameter |
Phytochemical studies
Roots Contains alkaloids, flavonoids, lignans, and organic acids indigotin, indigo, indirubin, β-sitosterol, γ-sitosterol and various amino acid. Leaves contain indigo, indigotin, isatan B, indirubin and rosasterol.
Pharmacological activity
Antiviral, Anti-inflammatory, Antioxidant, and Immunomodulatory activities
Uses:
Its roots and leaves are used in traditional Chinese medicine to treat viral pneumonia, hepatitis, influenza, and for detoxification
Green tea
Archeological evidence suggests that people consumed tea leaves steeped in boiling water as many as 500,000 years ago. Botanical evidence indicates that India and China were among the first countries to cultivate tea. Today, hundreds of millions of people drink tea around the world, and studies are now suggesting that green tea (Camellia sinensis) in particular has many health benefits.There are three main varieties of tea-green, black, and oolong. The difference between the teas is in their processing. Green tea is made from unfermented leaves and reportedly contains the highest concentration of powerful antioxidants called polyphenols.
Geographical source:
Green tea has been consumed throughout the ages in India, China, Japan, and Thailand.

Figure : 4 Camellia sinensis (L.)
Table: 2 Taxonomical classification of Camellia sinensis
|
Common name |
Green tea |
|
Habit |
Evergreen shrub or small tree, 1-5 m tall with spreading branches |
|
Botanical name |
Camellia sinensis |
|
Family : |
Theaceae |
|
Leaves |
Exstipulate, lanceolate to obovate; 4-10 cm long, 2-5 cm broad; serrate margins, pubescent when young, becoming glabrous; bright green, leathery. |
|
Fruit |
Woody capsule, 3-lobed, containing 1-3 seeds per locule |
|
Flowers |
White, fragrant, axillary; 2-4 cm diameter; solitary or in clusters |
Phytochemical screening activity
Polyphenols/Catechins, Flavonoids & Flavonols, Alkaloids, Tannins & Saponins, Phenolic Acids
Pharmacological Activities
Anti-inflammatory, Antidiabetic. Anticancer/Antitumor, Antioxidant.
Uses
In traditional Chinese and Indian medicine, practitioners used green tea as a stimulant, diuretic (to promote the excretion of urine), astringent (to control bleeding and help heal wounds), and to improve heart health.
Chamomile

Table: 3 Taxonomical classification of Matricaria recutita L
|
Common name |
German chamomile / True chamomile |
|
Habit |
Annual |
|
Botanical name |
Matricaria recutita L |
|
Family : |
Asteraceae |
|
Leaves |
Thin, spindle-shaped roots |
Phytochemical screening activity
Active component of chamomile contains terpenoids (bisoprolol, matricin, and chamazulene), flavonoids (luteolin, rutin, and apigenin), hydroxycoumarins, and mucilages.
Pharmacological Activities
Anti-inflammatory, antioxidant, sedative, and antispasmodic, driven by compounds like apigenin, bisabolol, and chamazulene. It inhibits inflammation by suppressing COX-2 and iNOS, acts as a mild sedative via GABA receptor binding, and treats gastrointestinal issues.
Collection of materials (15)
From the medicinal garden are harvested, including all herbs. With rinsed water, clean the herbs. Then let the herbs dry in the sun for 5 to 6 days. These herbs are transformed into fine powder after drying. Followed by usage in formulation.
Formulation of gel
The gelling ingredient carbopol 934 is utilised in the formulation of gels. is used as a gelling agent in the treatment of mouth ulcers. After being adequately soaked in distilled water for the night, Carbopol 934 was combined with distilled water while being constantly stirred with a mechanical stirrer. With constant stirring, all plant extract was combined with the necessary amount of methyl paraben and propyl paraben. The fluid also included propylene glycol. Create with water for up to 20 ml, and the pH was then adjusted by adding triethanolamine to get the desired consistency of gel. The herbal gel formulations were created.
Method of preparation of simple herbal gel
Combined demineralized water and carbopol 934 Add 5 ml of distilled water with the propyl paraben and methyl paraben warming in a water bath
When it has cooled, add propylene glycol. Then mix in various extracts or powdered herbs in varying concentrations.
All chemicals were combined with carbopol 934. Triethanolamine should be added gradually while stirring to get the required pH. (6.5- 7) [1]
EVALUATION (16)
Gel formulations are evaluated based on visual appearance, pH, homogeneity, and spreadability.
Visual appearance: Color, clarity, texture, transparency, and presence of gritty particles.
PH Measurement: Dissolve 1 g of gel in 10 mL distilled water, allow to stand for 2 hours, then measure pH three times and report the average value.
Homogeneity: Gel formulations are assessed for homogeneity through visual inspection after being poured into containers. The gel is examined for any aggregate masses or inconsistencies in appearance.
Spreadability
Definition: Spreadability measures how easily the gel spreads on the skin, expressed as the time (in seconds) required for two glass slides to separate when a gel sample is placed between them under a specified weight.
Procedure:
Place a precise amount of gel (typically 0.5–1 g) between two clean glass slides.
Apply a standard weight (e.g., 500–1000 g) on the upper slide to ensure uniform pressure.
Measure the time taken for the slides to slip apart completely due to the gel's spreading action.
Lower separation time indicates superior spreadability, reflecting better formulation performance for topical application
This test mimics skin application, ensuring the gel spreads smoothly without excessive resistance
Spreadability is calculated by using the formula.
S = M × L / T
Where, M = weight tied to upper slide
L = length of glass slides
T = time taken to separate the slides.
Viscosity: Viscosity is determined using a Brookfield viscometer with spindle #64 at 10, 20, and 30 rpm.
In Vitro Drug Release Study (15)
Franz diffusion cells are employed to evaluate in vitro drug release from the herbal gel formulation. The donor compartment receives 1 mL of formulation (equivalent to 1 g gel), while the receptor compartment is filled with freshly prepared phosphate buffer (pH 6.8). An egg membrane separates the chambers, with one cell serving as a blank containing only phosphate buffer.
The assembly is placed on a thermostated magnetic stirrer maintained at 37 ± 0.5°C. Samples (1 mL) are withdrawn at 1-hour intervals, replaced with an equal volume of fresh buffer from the blank to maintain sink conditions. Withdrawn samples are diluted to 10 mL with PBS (pH 6.8), and drug concentration is quantified using UV-Vis spectrophotometry (with PBS pH 6.8 as blank). Cumulative percent drug release is calculated using a pre-established calibration curve.
RESULT:
The present review and formulation focus on oral mucositis, a severe inflammatory and ulcerative condition commonly induced by chemotherapy and radiotherapy in cancer patients. Oral mucositis significantly affects patients’ quality of life by causing pain, difficulty in swallowing, increased risk of infection, and potential interruption of cancer therapy.
The proposed herbal formulation incorporates selected medicinal plants known for their anti-inflammatory, antioxidant, antimicrobial, and wound-healing properties. These include Isatis indigotica, Camellia sinensis, and Matricaria recutita.
Isatis indigotica is known for its anti-inflammatory and antiviral activities.
Camellia sinensis (green tea) possesses strong antioxidant and anti-inflammatory properties due to its polyphenolic compounds.
Matricaria recutita (chamomile) exhibits soothing, antimicrobial, and wound-healing effects.
A herbal gel will be prepared incorporating extracts of the above ingredients. The formulation will then be subjected to various evaluation tests, including physicochemical characterization (pH, viscosity, spreadability), stability studies, antimicrobial activity, and in vitro/in vivo assessment of anti-inflammatory and wound-healing potential.
REFERENCES

Indumathy K, Nandhini S., Mohamed musharaf A., Karthigeyan R., Kavin Kumar A., Madhan kumar S., Herbal Mouth Gel Formulations and Evaluation for the Management of Mucositis: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 970-977 https://doi.org/10.5281/zenodo.19448748
 10.5281/zenodo.19448748
10.5281/zenodo.19448748
