Department of Homoeopathic Pharmacy, Hamsa Homeopathy Medical College, Hospital & Research Centre, Siddipet, Telangana 502279.
Ear, nose, and throat disorders represent frequent pediatric health challenges, often requiring holistic management beyond conventional interventions. This study explores the anatomical development and pathophysiology of ENT structures in children, alongside prevalent conditions like otitis media, allergic rhinitis, sinusitis, pharyngitis, and tonsillitis, emphasizing homeopathic therapeutics for individualized symptom relief. Through detailed embryology, clinical descriptions, and a resolved case of a 13-year-old male with acute tonsillitis—featuring throat pain associated with difficulty in swallowing solid food also there is Stitching type of Pain, bilateral temple headache, and fear of snakes—Belladonna 200C demonstrated efficacy in reducing inflammation, pain, and systemic symptoms over follow-ups, highlighting homeopathy's role in restoring immune balance without antibiotics or surgery.
Ear, nose, and throat (ENT) disorders constitute a significant portion of pediatric consultations worldwide, frequently disrupting children's daily activities, sleep, and development due to their high prevalence in early childhood. Conditions such as acute otitis media, allergic rhinitis, sinusitis, pharyngitis, and tonsillitis arise from unique anatomical vulnerabilities in developing ENT structures, compounded by immature immune responses and environmental factors like infections or allergens.
Pediatric ENT Anatomy
ENT organs undergo critical embryological development early in intrauterine life, with the ear's labyrinth forming first by 20 weeks, followed by middle ear structures by 30 weeks, making infants particularly susceptible to congenital anomalies and infections. The nose's osteocartilaginous framework and turbinates, along with the pharynx's lymphoid tissues like tonsils, serve as primary defense barriers but often become sites of inflammation in children aged 6 months to 6 years.
Common Challenges
Acute otitis media peaks between 6-24 months, while chronic suppurative forms and mastoiditis emerge from unresolved infections; nasal issues like adenoid hypertrophy cause obstruction, and throat conditions including tonsilliti, streptococcal pharyngitis risk complications like rheumatic fever. Conventional approaches emphasize antibiotics and surgery, yet rising resistance and recurrence highlight the need for holistic alternatives.
AIMS :
OBJECTIVES :
MATERIALS & METHODS
1. Textbooks and Academic References
Authoritative medical and homeopathic texts were referred to for embryology, anatomy, clinical features, and treatment guidelines of ENT diseases in children, including:
2. Software and Digital Tools
3. Clinical Materials
4. Diagnostic & Examination Findings
5. Homeopathic Medicines
6. Literature for ENT Development and Pathology
Materials used to describe:
REVIEW OF LITERATURE
EAR
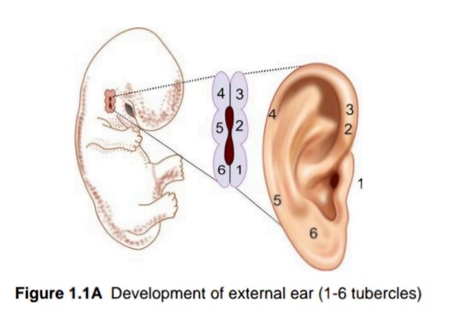
DEVELOPMENT OF EAR
External Ear
Middle Ear
Inner Ear
Labyrinth is the first organ, which develops before other organs has yet started forming in the embryo. Vestibular apparatus develops before cochlea. 1
ANATOMY OF EAR
Ear can be divided into three parts:
External Ear
External ear consists of pinna and the external auditory meatus.
Middle Ear Cavity
Middle ear cleft consists of middle ear proper, eustachian tube and mastoid antrum.
Middle ear cavity is further subdivided into:
Internal Ear
Internal ear consists of a bony labyrinth contained within the petrous temporal bone along with the membranous labyrinth . Otic capsule develops from 14 centers.[1]
Bony Labyrinth
It consists of
DISEASES OF EAR
Otitis externa
Otitis externa is inflammation of the external auditory canal. Acute diffuse otitis externa is the most common form in children. Acute localised otitis externa , chronic otitis externa and malignant otitis externa are less common. It predominantly affects children between the ages of 5 and 14 years but can affect any age group. [3]
Acute otitis media
Acute otitis media is one of the most common primary care paediatric presentations. It is most prevalent between 6 and 24 months of age and then declines with a small increase at 5 and 6 years of age. It occurs as a result of infection of the middle ear cavity by both viral and bacterial organisms. A bulging tympanic membrane with evidence of middle ear inflammation and middle ear effusion supports the clinical diagnosis. [3]
Chronic suppurative otitis media
Chronic suppurative otitis media is characterised by chronic inflammation of the middle ear with chronic discharge and tympanic membrane perforation. It typically occurs in children under 2 years of age, but it can occur in older children. It generally occurs following perforation of the eardrum from acute otitis media. It may also occur as a complication of tympanostomy tube placement [3]
Otitis media with effusion
Otitis media with effusion is the presence of a middle ear effusion in the absence of acute inflammation/infection. It is more likely to be an incidental finding. It is extremely common, particularly in preschool children and tends to occur after an episode of acute otitis media. Its significance is in relation to its effect on conductive hearing. [3]
Mastoiditis
Mastoiditis is the infection of the mastoid air cells. Presentation can occur at any age, with a median of 12-48 months. There is some evidence that decreased use of antibiotics for AOM has resulted in a small increase in cases of mastoiditis. [3]
GENERAL MANAGEMENT
Acute and Chronic Otitis Media
General Precautions
Suppurative Otitis Media
NOSE
EXTERNAL NOSE
It is pyramidal in shape with its root up and the base directed downwards. Nasal pyramid consists of osteocartilaginous framework covered by muscles and skin. [4]
OSTEOCARTILAGINOUS FRAMEWORK
Bony Part
Upper one-third of the external nose is bony while lower two-thirds are cartilaginous. The bony part consists of two nasal bones which meet in the midline and rest on the upper part of the nasal process of the frontal bones and are themselves held between the frontal processes of the maxillae [4]
Cartilaginous Part
It consists of
NASAL MUSCULATURE
Osteocartilaginous framework of nose is covered by muscles which bring about movements of the nasal tip, ala and the overlying skin. They are the procerus, nasalis, levator labii superiors alaeque nasi, anterior and posterior dilator nares and depressor septic. [4]
INTERNAL NOSE
It is divided into right and left nasal cavities by nasal septum. Each nasal cavity communicates with the nor through maris or nostril and with the nasopharynx through posterior nasal aperture or the chisania. Each nasal cavity consists of a skin-lined portion-the vestibule and a mucosa-lined portion, the nasal cavity proper. [4]
VESTIBULE OF NOSE
Anterior and inferior part of nasal cavity is called vesti-bufe. It is lined by skin and contains sebaceous glands, hair follicles and the hair called thrissae. Its upper limit on the lateral wall is marked by limen nasi called nasal valve).
NASAL CAVITY PROPER
Each nasal cavity has a lateral wall, a medial wall, a roof and a floor.[4]
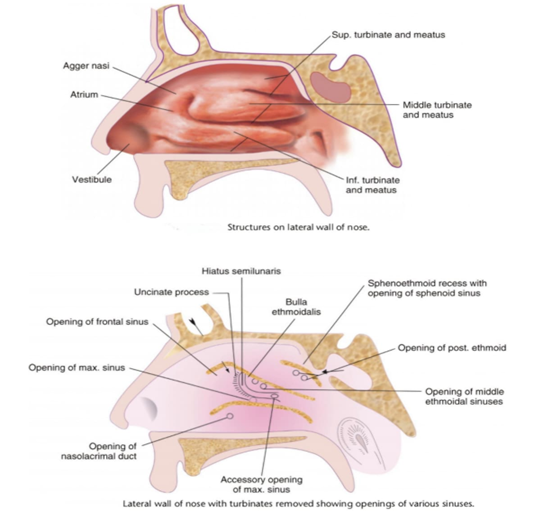
Lateral Nasal Wall
Three and occasionally four turbinates or conchae mark the lateral wall of nose. Conchae or turbinates are scroll-like bony projections covered by mucous mem-brane. The spaces below the turbinates are called meatuses. [4]
Medial wall
Nasal septum consists of three parts
Roof
Anterior sloping part of the roof is formed by nasal bones, posterior sloping part is formed by the body of sphenoid bone and the middle horizontal part is formed by the cribriform plate of ethmoid through which the olfactory nerves enter the nasal cavity. [4]
Floor
It is formed by palatine process of the maxilla in its an terior three-fourths and horizontal part of the palatine bone in its posterior one-fourth. [4]
DISEASES OF THE NOSE AND SINUSES
Allergic Rhinitis
Allergic rhinitis is an inflammatory disorder characterized by sneezing, itching, nasal obstruction and clear rhinorrhea. Examination reveals a pale nasal mucosa, congested nasal turbinates and mucoid rhinorrhea. Conjunctival itching and redness may be present. Inhaled allergens (eg. Pollen, spores and dust mites) are common causes.[3]
Sinusitis
Sinusitis can be classified as either acute or chronic. The ethmoid and maxillary sinuses are the earliest to develop and are the ones most commonly infected in paediatrics sinusitis. The frontal sinuses may become involved only after 5-6 year of life; isolated sphenoid disease is rare. Risk factors associated with sinusitis include recurrent upper respiratory infections, allergic rhinitis, cystic fibrosis, immunodeficiency, ciliary dyskinesia, daycare attendance and exposure to tobacco smoke.
Nasal Obstruction
Chronic mouth breathing in children is generally caused by blockage of nasal airflow. The site of nasal blockage is most often in the nasopharyngeal area due to adenoid hypertrophy. Intranasal causes of obstruction include allergic rhinitis, recurrent sinusitis, nasal septum deviation, turbinate hypertrophy, nasal polyps and less commonly, neoplasms.
Adenoid enlargement should be suspected in children, usually older than 2 yr, who present with nasal blockage, mouth breathing, sleep disturbance and chronic nasal discharge.[3]
Epistaxis
Bleeding from the nose occurs frequently in children. Most paediatrics epistaxis occurs in the anterior portion of the nasal septum at a confluence of arterial vessels known as Little's area (Kiesselbach plexus). Local trauma, especially nose picking, is by far the most common cause of paediatrics epistaxis. Less frequent causes of recurrent epistaxis include juvenile nasopharyngeal angiofibroma and hereditary hemorrhagic telangiectasia. Hereditary telangiectasia also known as Osler-Weber-Rendu syndrome, is a genetic defect in blood vessel structure resulting in arteriovenous malformations.[3]
General Management
THORAT
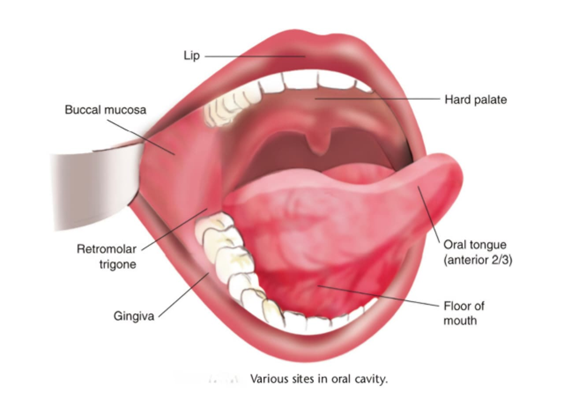
The oral cavity extends from the lips to the oropharyngeal al isthmus.It is divided in to following sites:
CAUSES OF ULCERS OF THE ORAL CAVITY
MISCELLANEOUS LESIONS OF TONGUE AND ORAL CAVITY
Anatomy and Physiology of Pharynx
Pharynx is a conical fibromuscular tube forming upper part of the air and food passages. It is 12–14 cm long, extending from base of the skull (basiocciput and basisphenoid) to the lower border of cricoid cartilage where it becomes continuous with the oesophagus. [4]
STRUCTURE OF PHARYNGEAL WALL
Consists of four layers:
DIVISIONS OF PHARYNX
Anatomically, pharynx is divided into three parts
Applied Anatomy-
Rathke’s Pouch- It is represented clinically by a dimple above the adenoids and is reminiscent of the buccal mucosal invagination, to form the anterior lobe of pituitary. A craniopharyngioma may arise from it. [4]
Clinically, It is subdivided into three regions—the pyriform sinus, postcricoid region and the posterior pharyngeal wall.[4]
ACUTE PHARYNGITIS
Acute pharyngitis is very common and occurs due to varied aetiological factors like viral, bacterial, fungal.Acute streptococcal pharyngitis (due to Group A beta-haemolytic Streptococci) has received more importance because of its aetiology in rheumatic fever and poststreptococcal glomerulonephritis. [4]
CLINICAL FEATURES
Pharyngitis may occur in different grades of severity. Milder infections present with discomfort in the throat, some malaise and low-grade fever. Pharynx in these cases is congested but there is no lymphadenopathy. Moderate and severe infections present with pain in throat, dysphagia, headache, malaise and high fever. Pharynx in these cases shows erythema, exudate and enlargement of tonsils and lymphoid follicles on the posterior pharyngeal wall.[4]
CHRONIC PHARYNGITIS
It is a chronic inflammatory condition of the pharynx. Pathologically, it is characterized by hypertrophy of mucosa, seromucinous glands, subepithelial lymphoid follicles and even the muscular coat of the pharynx.
Chronic pharyngitis is of two types:
SYMPTOMS
Severity of symptoms in chronic pharyngitis varies from person to person.
SIGNS
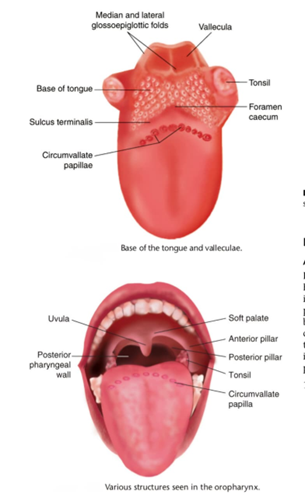
Palatine tonsils are two in number. Each tonsil is an ovoid mass of lymphoid tissue situated in the lateral wall of oropharynx between the anterior and posterior pillars. Actual size of the tonsil is bigger than the one that appears from its surface as parts of tonsil extend upwards into
The soft palate, downwards into the base of tongue and Anteriorly into palatoglossal arch. A tonsil presents two Surfaces a medial and a lateral, and two poles an upper and a lower.[4]
BLOOD SUPPLY
The tonsil is supplied by five arteries
FUNCTIONS OF TONSILS
They act as sentinels to guard against foreign intruders like viruses, bacteria and other antigens coming into contact through inhalation and ingestion. There are two mechanisms:
ACUTE TONSILLITIS classified as
SYMPTOMS
COMPLICATIONS
CHRONIC TONSILLITIS
TYPES
CLINICAL FEATURES
COMPLICATIONS
DISEASES OF LINGUAL TONSILS
GENERAL MANAGEMENT OF TONSILLITIS
HOMEOPATHIC THERAPEUTICS
Baryta carbonica
Submaxillary glands and tonsils swollen. Takes cold easily, with stitches and smarting pain. *Quinsy*. Suppurating tonsils from every cold. Tonsils inflamed, with swollen veins. Smarting pain when swallowing; worse empty swallowing. Feeling of a plug in pharynx. can only swallow liquids. Spasm of esophagus as soon as food enters esophagus, causes gagging and choking (Merc cor; Graphite). Throat troubles from over use of voice. Stinging pain in tonsils, pharynx or larynx.[2]
Baptisia Tinctoria
Dark redness of tonsils and soft palate. Constriction, contraction of esophagus (Cajeput). Great difficulty in swallowing solid food. Painless sore throat, and offensive discharge. Contraction at cardiac orifice.[2]
Belladonna
Dry, as if glazed; angry?looking congestion (Ginseng); red, worse on right side. Tonsils enlarged; throat feels constricted; difficult deglutition; worse, liquids. Sensation of a lump. Esophagus dry; feels contracted. Spasms in throat. Continual inclination to swallow. Scraping sensation. Muscles of deglutition very sensitive. Hypertrophy of mucous membrane[2]
Kali muriaticum
Follicular tonsillitis. Tonsils inflamed; enlarged so much, can hardly breathe. Grayish patches or spots in the throat and tonsils. Adherent crusts in vault of pharynx. “Hospital” sore throat. Eustachian catarrh.[2]
CASE:
A 13yrs old male, weight of 34kgs came to Hamsa homeopathy OPD with complaints of pain in the throat since 1 week associatedwith difficulty in swallowing solid food. There is also stitching type of pain. Patient also complained of headache since 3 days on and off. Pain on both right and left side of temples region. Heaviness in both temples region. Throbbing type of headache aggravates after eating and early morning. The complaints started suddenly about 1week.He had a history of fall from bike in 2023, marks present over left cheek, left hand and over right big toe. In physical generals, his appetite moderate, thirst decreased. He found to be chilly patient. Mental general - he has fear of snakes, fear when someone try's to hit him.
Physical Examination:
Inspection -
Palpation -
Diagnosis - ACUTE TONSILLITTIS
While analyzing the case, mental and physical generals, characteristic particulars and few diagnostic symptoms were considered for erecting the totality of symptoms.
Totality of symptoms:
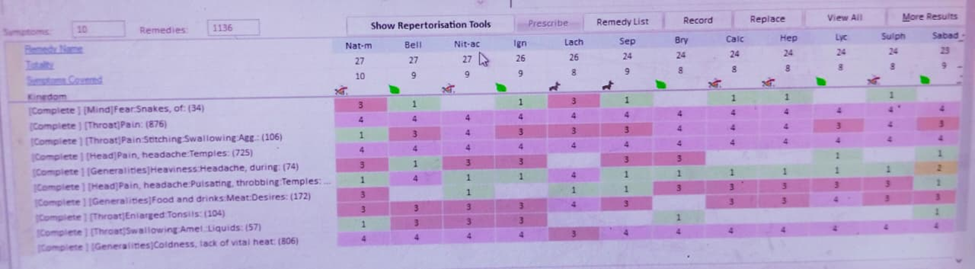
Considering the totality, complete repertory was selected and Repertorisation was done with HOMPATH ZOMEO Software.After Repertorisation from the list of drugs Belladonna 200c -3doses was selected after further confirmation from materia medica.[5]
Follow up
|
15-11-2025 |
Pain in the throat is slightly better Heaviness in head persists Thirst – decreased |
Belladonna 200 c 1 dose |
|
22-11-2025 |
Pain in the throat slightly better Heaviness in head reduced Thirst-slightly increased |
Belladonna 200 c 1 dose |
|
28-11-2025 |
Pain in the throat reduced Heaviness in head reduced Generals – improved |
Sac lac 1 dose |
DISCUSSION
This Case Concerns a 13 yrs, male experiencing pain in throat with difficulty is swallowing, also Complained of headache on both sides of temples. Clinical findings- tenderness present over submandibular region. There is no lymphadenopathy. Inflammation and redness present and Tonsils enlarged bilaterally (+).
The Case was examined holistically, giving attention to mental and physical generals, characteristic particulars and few diagnostic symptoms. The patient displayed fear of Snakes & fear when someone tries to hit him. These mental generals have Significantly shaped the individualizing totality. Physical generals such as loss of vital heat, appetite moderate, thirst decreased, sleep disturbed combined with local symptoms. Pain in throat with difficult in swallowing aggravates while eating and ameliorates by drinking water. Headache in both sides of temples, throbbing type of pain with heaviness in head aggravates after eating and early morning.
Repertorisation using the complete repertory in HOMPATH ZOMEO BELLADONNA 200C WAS SELECTED. Its materia medica profile closely fits pain in the throat complaints, headache on both temples, fear of snakes.
Considering the close correspondence between the patient’s totality, Repertorial indications and the remedy’s clinical sphere belladonna 200c was chosen to address both the physical pathology and the underlying mental generals offering a personalized and integrative therapeutic plan.
CONCLUSION:
Tonsillitis represents an acute or recurrent inflammatory disorder influenced by infective, immunological, and environmental factors that disturb the local oro-pharyngeal defense mechanisms. While conventional management relies on analgesics, antipyretics, and, in severe cases, antibiotics or surgical intervention, homeopathy provides an individualized, holistic, and non-invasive therapeutic approach aimed at modulating the immune response, reducing mucosal inflammation, and promoting natural recovery. By focusing on the characteristic symptom totality rather than the pathological outcome alone, homeopathic remedies help restore physiological balance, shorten the duration of acute episodes, and potentially reduce recurrence. This case highlights the role of homeopathy as a safe, effective, and integrative option in supporting long-term throat and immune health.
ACKNOWLEDGEMENT
I extend heartfelt thanks to Director Dr. Umesh Akkaladevi Sir, Principal Prof. Dr. Nurus Saher Khan Madam. Hamsa Homoeopathy Medical College Hospital & Research Centre. My mentors, colleagues, and peers for their guidance, constructive suggestions, and encouragement throughout the preparation of this work.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to the research, authorship, or publication of this article. All data presented are based on clinical observation, standard homeopathic principles, and authenticated literature sources.
REFERENCES

Dr. Srinivas Babu Kathi, Dr. Kavya Boini, Dr. Nagavath Swetha, Dr. Gangadari Srilekha, Dr. Budharapu Roopini, Dr. Shaik Ruksana, Dr. Aluka Sai Prabha, Holistic Management of Pediatric ENT Diseases: Integrating Embryology, Clinical Features, and Homeopathic Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3512-3527. https://doi.org/10.5281/zenodo.18038339
 10.5281/zenodo.18038339
10.5281/zenodo.18038339
