Sharda School of Pharmacy Gandhinagar, Gujarat, India.
Polycystic ovary syndrome (PCOS) is a multifactorial endocrine and metabolic disorder affecting 4–20% of women of reproductive age worldwide and is a leading cause of anovulatory infertility. Women with PCOS experience a significantly increased risk of adverse pregnancy outcomes due to hormonal imbalance, insulin resistance, and chronic low-grade inflammation. Numerous studies and meta-analyses indicate that women with PCOS have a two- to threefold higher incidence of gestational diabetes mellitus (GDM), pregnancy-induced hypertension, and preeclampsia compared to women without PCOS. The risk of early pregnancy loss, preterm delivery, and cesarean section is also markedly elevated. Insulin resistance and hyperandrogenism contribute to impaired endometrial receptivity, abnormal placentation, and vascular dysfunction, which underlie many of these complications. Furthermore, obesity—a frequent comorbidity—exacerbates metabolic and obstetric risks. Recent data suggest that early diagnosis, lifestyle modification, and the use of insulin-sensitizing agents such as metformin can improve reproductive outcomes and reduce miscarriage rates. Despite advances in assisted reproductive technologies, women with PCOS still demonstrate lower fertilization and implantation rates and increased risk of ovarian hyperstimulation syndrome. Continuous monitoring and individualized preconception counseling remain essential to improve maternal and fetal health. This review summarizes the latest evidence regarding the pathophysiology, pregnancy complications, and management strategies for optimizing pregnancy outcomes in women with PCOS.
Polycystic ovary syndrome (PCOS) is a problem with hormones that happens during the reproductive years. If you have PCOS, you may not have periods very often. Or you may have periods that last many days. You may also have too much of a hormone called androgen in your body. With PCOS, many small sacs of fluid develop along the outer edge of the ovary. These are called cysts. The small fluid-filled cysts contain immature eggs. These are called follicles. The follicles fail to regularly release eggs. The exact cause of PCOS is unknown. Early diagnosis and treatment along with weight loss may lower the risk of long-term complications such as type 2 diabetes and heart disease.
SYMPTOMS
Symptoms of PCOS often begin around the first menstrual period, though sometimes they appear later. Diagnosis requires at least two of the following criteria:
Irregular periods: Having few menstrual periods or having periods that aren't regular are common signs of PCOS. So is having periods that last for many days or longer than is typical for a period. For example, you might have fewer than nine periods a year. And those periods may occur more than 35 days apart. You may have trouble getting pregnant.
Excess androgen: Too much androgen. High levels of the hormone androgen may result in excess facial and body hair. This is called hirsutism. Sometimes, severe acne and male-pattern baldness can happen, too.
Polycystic ovaries: Your ovaries might be bigger. Many follicles containing immature eggs may develop around the edge of the ovary. The ovaries might not work the way they should.
CAUSES
The exact cause of PCOS isn't known. Factors that might play a role include:
Insulin resistance: Insulin is a hormone that the pancreas makes. It allows cells to use sugar, your body's primary energy supply. If cells become resistant to the action of insulin, then blood sugar levels can go up. This can cause your body to make more insulin to try to bring down the blood sugar level. Too much insulin might cause your body to make too much of the male hormone androgen. You could have trouble with ovulation, the process where eggs are released from the ovary. One sign of insulin resistance is dark, velvety patches of skin on the lower part of the neck, armpits, and groin or under the breasts. A bigger appetite and weight gain may be other signs.
Low-grade inflammation: White blood cells make substances in response to infection or injury. This response is called low-grade inflammation. Research shows that people with PCOS have a type of long-term, low-grade inflammation that leads polycystic ovaries to produce androgens. This can lead to heart and blood vessel problems.
Heredity: Research suggests that certain genes might be linked to PCOS. Having a family history of PCOS may play a role in developing the condition.
Excess androgen: With PCOS, the ovaries may produce high levels of androgen. Having too much androgen interferes with ovulation. This means that eggs don't develop on a regular basis and aren't released from the follicles where they develop. Excess androgen also can result in hirsutism and acne.
COMPLICATIONS
PATHOPHYSIOLOGY
The pathophysiology of PCOS is multifactorial, and it is believed that a genetic predisposition exists that is exacerbated by excess adiposity. It is thought that the pathophysiology of PCOS involves the interaction between abnormal ovarian morphology, due to excess androgen production by the PCO—hyperinsulinemia, and elevated luteinizing hormone (LH) levels.4 It has been shown that ovarian androgen production in women with PCOS is accelerated due to the increased ovarian theca cell androgenic enzymatic activity of 3β-hydroxysteroid dehydrogenase (HSD) 17α-hydroxylase/C17, 20 lyase, a product of CYP17. 5 Women affected by PCOS can present with a spectrum of signs and symptoms, ranging from having minimal to major systemic manifestations of hyperandrogenaemia and may have profound implications for a woman with regard to her reproductive health and the Long-term health outcomes of her offspring.6 the aim of this critical review is to highlight these potential implications and suggested interventions to reduce their impact.
POLYCYSTIC OVARIAN SYNDROME (PCOS) CLINICAL FEATURES
A complete clinical assessment is critical for the diagnosis of PCOS. Diagnosis comprises criteria of which 2 out of 3 consist of history and physical examination elements, including menstrual history, fertility history, obesity, and features of hyperandrogenism. Additionally, PCOS represents a diagnosis of exclusion; therefore, clinical presentation of other conditions should be recognized.
1. Menstrual Irregularities
According to the 2023 International Evidence-Based PCOS Guidelines, irregular menstrual cycles are defined as:
2. Hair Loss Patterns
Hair loss patterns can vary widely, often appearing in a vertex, crown, or diffuse pattern. Women with more severe hyperandrogenism may experience bitemporal hair loss and a receding frontal hairline. Additionally, adolescents with severe or treatment-resistant acne, whether to oral or topical antibiotics, may have a 40% chance of developing PCOS. Clinicians should be particularly vigilant for underlying hyperandrogenism in females in their mid-20s to 30s who have persistent or worsening acne.
3. Hirsutism and Virilization
Hirsutism is characterized by the presence of course, dark terminal hairs in a pattern typically associated with males. Signs of virilisation, e.g., increased muscle mass, reduced breast size, deepening of the voice, and clitoromegaly, are not commonly seen in PCOS. Virilization suggests elevated androgen levels, which warrants further investigation. In such cases, clinicians should be more concerned about the possibility of an androgen-producing tumour in either the ovary or the adrenal gland.4
Reproductive features in women with PCOS
Adolescents with PCOS often have earlier menarche, particularly if they are obese.7 Precocious puberty, early adrenarche presenting with early pubic hair development or oligomenorrhoea may also be presenting symptoms.13-16 With regard to the potential etiology of PCOS, it is thought that exposure to excess androgens in early fetal life may increase the likelihood of developing PCOS in later years.
Various clinical and phenotypic presentations may precede the diagnosis of PCOS and include, but are not limited to, hyperandrogenism, menstrual irregularity, olio/anovulation and infertility. In total, 80% of women affected by anovulatory infertility have PCOS, which is further adversely affected by excess weight. Furthermore, women with anovulatory infertility have a longer interval until pregnancy, hence are more likely to require fertility investigations and treatment. Interestingly, in one observational study, women with PCOS are also more likely to have had their first pregnancy at a younger age and gave birth at least once; however, the total number of pregnancies in their lifetime tends to be lower than women without PCOS. Women diagnosed with PCOS have a lower natural conception rate, an increased rate of biochemical pregnancy and a reduced response to artificial reproductive technology (ART).17
REPRODUCTIVE OUTCOMES
PCOS is associated with an increase in subfertility, ectopic pregnancy and early pregnancy loss (EPL).18-19 Potential causes are an altered endometrial environment and subsequent reduction in implantation success due to the hyper insulinemic environment and concurrent hyperandrogenism. The rates of infertility and EPL have been estimated to be 15 times and three times greater, respectively, than women of similar demographics however, it is unclear as to whether body mass index (BMI) or the use of fertility treatment (ovulation induction and/or in vitro fertilization (IVF)) had a role to play in the higher rates observed.
In one study, rates of EPL were no different between women with and without PCOS; however, the control group were comparatively older with lower ovarian reserve.17 A meta-analysis has reported a five times increased risk of EPL and reported a significant improvement of EPL in patients treated with metformin. It has been shown that treatment with the insulin sensitizer metformin, a synthetically derived biguanide, which leads to a reduction in serum insulin concentrations, may improve the features of PCOS. After IVF miscarriage, rates of 35.8% have been reported in women with PCOS in comparison to rates of 23.6% in women without PCOS; however, raised BMI, increased waist hip ratio and insulin resistance are also likely to play a part.
According to the World Health Organization (WHO), PCOS is the commonest cause of anovulatory infertility.20 For some women with PCOS undergoing IVF or in vitro maturation (IVM), increasing quantities of follicle-stimulating hormone (FSH) are required to stimulate ovulation, particularly in those women who are obese. Due to the polycystic nature of the ovaries in women with PCOS, they are at moderate risk of ovarian hyperstimulation syndrome (OHSS). Reported OHSS rates in the literature for women with PCOS who conceive after IVF are up to 7.5% compared to women without PCOS being in the order of 2.7%. Despite the increased oocytes retrieved during an IVF cycle, the oocytes are often of a poorer quality, and these cycles are characterized by lower fertilization rates and a higher incidence of embryo transfer cancellations due to failed fertilization or OHSS.
PREGNANCY COMPLICATIONS
Maternal Complications
Women with PCOS are at significantly higher risk of maternal complications, with studies reporting up to a threefold increase compared to healthy controls.22 This risk is influenced by pre-existing medical conditions, hyperinsulinemia, hyperandrogenemia, obesity, and frequent use of assisted reproductive technologies (ART), which also increase the likelihood of multiple pregnancies. Common complications include gestational diabetes mellitus (GDM), pregnancy-induced hypertension (PIH), preeclampsia (PET), and cesarean section (CS), all of which are consistently higher in women with PCOS, even after adjusting for BMI. For example, GDM is reported to be two- to threefold higher, PIH and PET are increased three- to fourfold, and the rate of operative deliveries, including CS, is doubled due to maternal obesity, fetal macrosomia, and ART-related multiple pregnancies. Additionally, increased gestational weight gain and oligo-anovulation contribute to a fivefold increase in adverse pregnancy outcomes. Prolonged time to conception, frequently observed in PCOS, further elevates obstetric and perinatal risks, emphasizing the importance of optimizing maternal health prior to conception and ensuring safe ART interventions aimed at singleton pregnancies.
Gestational Diabetes Mellitus
GDM is more common and often diagnosed earlier in women with PCOS, likely due to inadequate pancreatic β-cell function to compensate for the insulin resistance exacerbated by pregnancy.17, 26 Insulin resistance also contributes to vascular dysfunction, increasing pregnancy complications. In one study, women with GDM had higher BMI and lower β-cell function (HOMA-β), while other parameters such as fasting glucose, insulin, HOMA-IR, QUICKI, and testosterone did not differ from women without GDM. Obese women with PCOS exhibited severe insulin resistance and impaired β-cell function compared to normal-weight patients, highlighting the importance of preconception BMI reduction and β-cell assessment to predict and reduce GDM risk. Sterling et al. reported a 15.5% incidence of GDM in women with PCOS versus 5% in controls, while lean women with PCOS did not have a significantly increased risk.
Hypertensive Disorders
Women with PCOS are also at higher risk of PIH and PET, independent of BMI and ART.27,28 Elevated maternal androgen levels, particularly testosterone, may impair trophoblast invasion and placental function, contributing to abnormal placentation.29–31 Pregnancy further exacerbates the chronic low-grade inflammation seen in PCOS, with increased LDL, triglycerides, free radicals, and inflammatory markers inducing endothelial dysfunction, spiral artery remodeling, and reduced uterine artery impedance.29,32,33
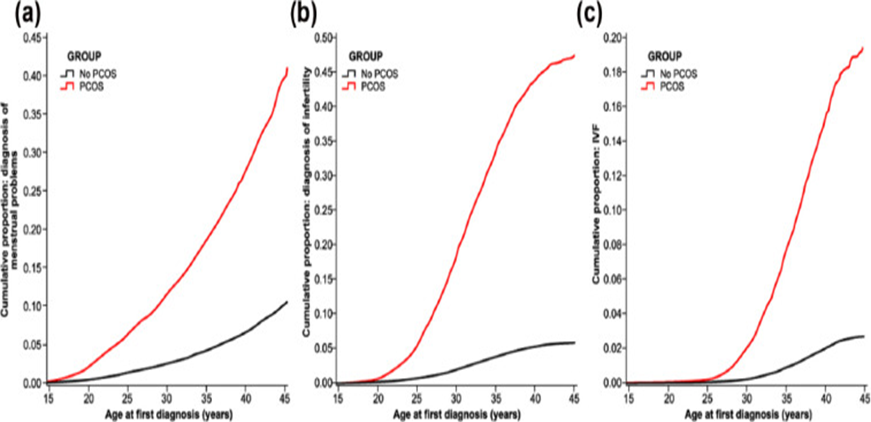
Figure 1 Courtesy – National Institute Of Health
Preterm Delivery and Perinatal Outcomes: Rates of preterm delivery (PTD) in women with PCOS are increased, particularly for those with hyperandrogemia. Doherty et al. reported rates of 21.1% compared to 12.5% in the control group (Table 1). The risk of stillbirth is elevated with rates reported in the order of 3.3% versus 1.6% in control groups. Elevated stillbirth rates are influenced by the effects of increased maternal pregnancy risk factors in women with PCOS and prematurity. In an older study, using a control group with a low ovarian reserve, Sterling et al. demonstrated adverse pregnancy outcomes in women with PCOS who conceived via IVF, compared to those women who conceived with IVF who did not have PCOS. Their findings were consistent with those published in the literature. GDM and hypertensive disorders in pregnancy were both increased. They also found an increase in antepartum haemorrhage (APH), cervical cerclage placement, preterm premature rupture of membranes (PPROMs) and fetal death in utero (FDIU). These findings were consistent with those of Wax37 who also recorded increased rates of cesarean wound complications.
ETIOLOGY
PCOS is a complex, multigenic disorder with strong epigenetic factors associated with it.2 Genome-wide association studies (GWAS) have identified multiple PCOS-associated genetic loci; many of these genes are involved in various levels of insulin resistance, ovarian steroidogenesis, steroid hormone biosynthesis, PI3K-Akt signaling pathway, adrenal cortisone reductase deficiency, and gonadotrophic dysregulation3.
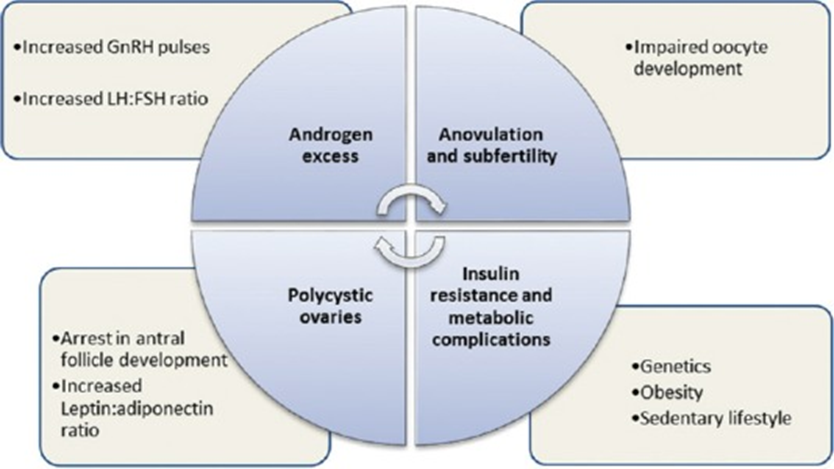
Figure – courtesy of National Institute Of Health
Epidemiology of PCOS in India
Only a few researchers have studied the prevalence of PCOS in India and among those, most of the sampling was convenience based, which might not reflect the true status of PCOS prevalence in the community. A pilot cross-sectional study conducted in Tamil Nadu assessed young adolescent females and found a prevalence of 18 per cent for PCOS34. They also concluded that the proportion of PCOS was higher in urban women in comparison to the rural women. A similar study conducted in Mumbai, which was an urban community-based study, found that the prevalence of PCOS was 22.5 per cent by the Rotterdam criteria and 10.7 per cent by the Androgen Excess Society criteria35. A study conducted among medical students at a private medical college in south India using the modified Cronin questionnaire36, which included 10 items, found that PCOS was a common disorder among the participants and reported a high incidence of mood disorders among them36. A study from Lucknow was published, in which college-going women with menstrual irregularity and hirsutism, in the age range of 18-25 yr, were studied, and it was reported that the calculated prevalence using the NIH criteria, among the participants, was only 3.7 per cent37. Another study from Andhra Pradesh studied young women from a residential college and found that 9.13 per cent of them satisfied the Rotterdam criteria for PCOS38. Vidya Bharathi et al39 showed that the prevalence of PCOS diagnosed by the Rotterdam criteria in community-dwelling women from rural and urban areas of Chennai was 6 per cent. International studies report the prevalence of PCOS to be in the range of 4-10 per cent of women of reproductive age40. As the prevalence of PCOS has been found to be higher or lower depending on the criteria used in these studies, which might be the obvious reason for the discrepancy in the prevalence rates among the studies from India, it is difficult to draw a clear conclusion. Hence, from the limited data available, it can be said that the prevalence of PCOS in India ranges from 3.7 to 22.5 per cent (Table III).
Table III Prevalence studies on polycystic ovary syndrome in Indian women/girls
|
Study |
n |
Place/ yr |
Population/sampling |
Prevalence per cent (criteria) |
|
Balaji et al |
126 |
Tamil Nadu/ 2015 |
Young adolescents (12-19 yr) Urban and rural |
18 (Rotterdam) |
|
Joshi et al |
600 |
Mumbai/ 2014 |
Adolescents and young adolescents (15-24 yr) Community based |
22.5 (Rotterdam) 10.7 (AES) |
|
Joseph et al |
441 |
Karnataka/ 2016 |
Medical and dental college students (20.4±1.5 yr) with either menstrual irregularity or hirsutism |
9.1 (modified version of Cronin questionnaire) |
|
Gill et al |
1520 |
Lucknow/ 2012 |
College girls (18-25 yr) with menstrual irregularity and hirsutism |
3.7 (NIH criteria) |
|
Nidhi et al |
460 |
Bengaluru/ 2011 |
College girls (15-18 yr) Oligomenorrhoea and/or hirsutism |
9.13 (Rotterdam) |
|
Vidya Bharathi et al |
Chennai/ 2017 |
Random general rural and urban population |
6 (Rotterdam) |
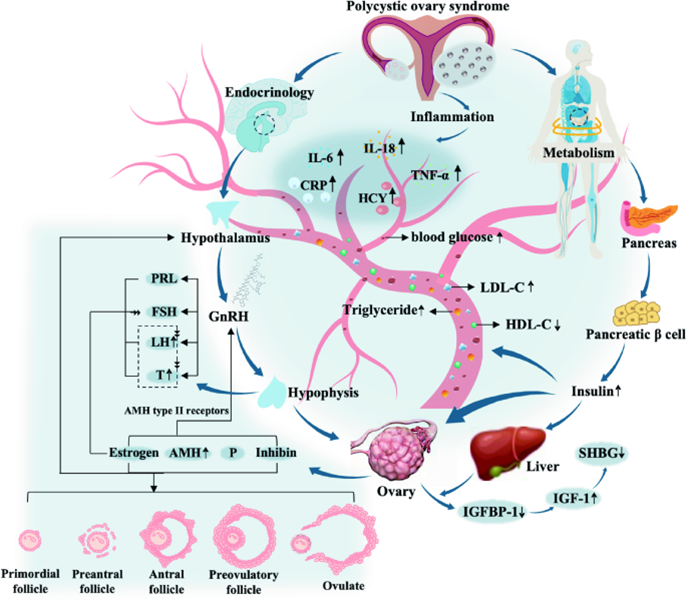
Figure – image courtesy Journal of Ovarian Research article 34 year [2025]
THERAPEUTIC GOALS
Difficulty in losing weight, irregular menses, infertility, and excessive hair growth were the most important health problems reported by patients with polycystic ovary syndrome in an international survey5.
These problems should therefore represent the main targets for therapeutic intervention, although priority setting partnerships are still needed to help focus research priorities. Existing drug treatments have not been licensed specifically for polycystic ovary syndrome and are used off-label to target symptoms. Also, previous studies have not emphasised health related quality of life measures when evaluating response to treatment. An ideal treatment for polycystic ovary syndrome should look at the health risks, reduce key processes in the pathogenesis of the disease, and be responsive to the symptom profile and needs of the individual. Where relevant, treatments should reduce clinical and biochemical hyperandrogenism, restore ovulatory cycles and fertility, normalise the length of the menstrual cycle, improve insulin sensitivity, reduce weight and cardiometabolic risk, and improve condition specific quality of life.
Existing treatments
Non-pharmacological interventions
International guidelines highlight the importance of modifications to lifestyle in the management of the disease6. Changes in lifestyle can improve fasting insulin levels and anthropometric outcomes, although benefits on hyperandrogenism are modest7 and adherence is often difficult to sustain in clinical practice. Data on reproductive benefits are limited8 although a recent small randomised controlled trial of 68 women with polycystic ovary syndrome showed that a behavioural modification programme improved menstrual regularity compared with a minimal intervention group Laser treatment might have a role in the treatment of facial hirsutism, although further trials are needed to confirm the benefits on quality of life and cost effectiveness6.
Contraceptive pill
In women not attempting to conceive, combined contraceptive pills are first line treatments for menstrual irregularity and hyperandrogenism he oestrogen component increases sex hormone binding globulin, thus reducing free testosterone and improving hyperandrogenism. Because this stimulatory effect on hepatic production of proteins also causes hypercoagulability, ethinyloestradiol based contraceptive pills containing the lowest effective dose of oestrogen (eg, 20-30 μg of ethinyloestradiol) are recommended. Combined contraceptive pills containing newer, more physiological, oestrogenic compounds have recently been developed, and might have a lower risk of venous thromboembolism than ethinyloestradiol9.
The progestogen component reduces ovarian androgen production by inhibiting secretion of luteinising hormone and protects the endometrium from hyperplasia10 Combined contraceptive pills containing androgenic progestogens, such as norethisterone, should be avoided because of the potential to aggravate hyperandrogenic symptoms. Furthermore, ethinyloestradiol based contraceptive pills containing cyproterone acetate, the most potent anti-androgenic progestogen, are not currently recommended as first line treatment because of the increased risk of venous thromboembolism A recent systematic review of 19 randomised controlled trials, however, concluded that the ethinyloestradiol-cyproterone acetate combination improved serum testosterone (mean difference 0.38 nmol/L, 95% confidence interval 0.33 to 0.43) and hirsutism compared with conventional combined contraceptive pills11. Thus combinations of cyproterone acetate and newer oestrogenic compounds might have the potential to improve hyperandrogenism in patients with polycystic ovary syndrome without the added risk of venous thromboembolism.
Anti-androgen agents
Currently available anti-androgen agents act by blocking androgen receptors (cyproterone acetate, spironolactone, and flutamide) or reducing production of androgens (finasteride and dutasteride). Guidance on specific preparations or doses in polycystic ovary syndrome is necessarily vague, because studies on these agents are few in number and small scale.
Furthermore, although targeting excess production of androgens might be crucial to improved patient outcomes, the use of currently available anti-androgen drugs is limited by side effects. All anti-androgen drugs carry a risk of feminisation of a male fetus and therefore use must be restricted to patients with adequate contraception in place6.
Insulin sensitisers
Metformin modulates hepatic insulin sensitivity and glucose production by activating AMP activated protein kinase and AMP activated protein kinase independent pathways. More recently, metformin has also been shown to mediate its antiglycaemic effects by actions on the gastrointestinal tract and the gut microbiome12.
If you want to become pregnant now or in the future, treatment for PCOS includes:
Drugs to induce ovulation (releasing an egg): A successful pregnancy begins with ovulation. Certain drugs have been proven to induce ovulation in people with PCOS. The medications clomiphene and letrozole are taken orally, while gonadotropins are given by injection.
Surgery: A surgical procedure can help restore ovulation by removing tissue in your ovaries that produces androgen hormones. With newer medications available, surgeons rarely perform this procedure.
In vitro fertilization (IVF): This is an option for people with PCOS when medication doesn’t help with ovulation. Your provider fertilizes your egg with your partner’s sperm in a lab before transferring it to your uterus.
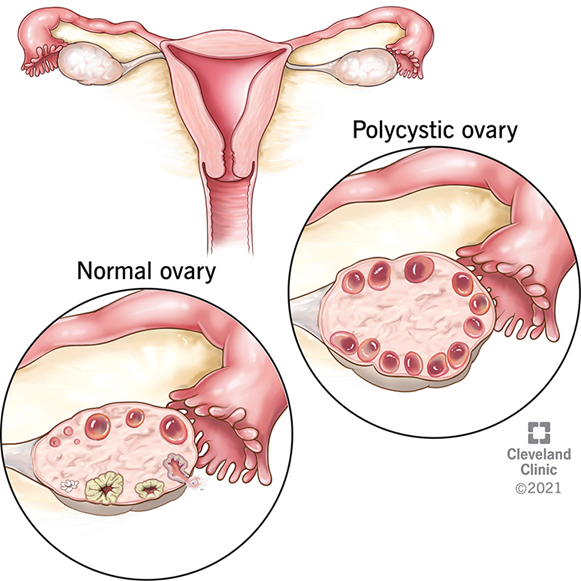
Erica Newlin, MD, explains what polycystic ovarian syndrome (PCOS).
Figure – courtesy of image Cleveland Clinic
While there isn’t a cure for PCOS, your healthcare provider can help you manage your symptoms. The effects of PCOS may change over time so that you become less aware of the condition. However, there isn’t a treatment that permanently cures it.
PCOS can make it hard to conceive while also increasing your risk for certain pregnancy complications, but many people with PCOS do get pregnant on their own. Your healthcare provider will work with you to develop a treatment plan to help you ovulate. Your treatment plan could include medication or assisted reproductive technologies like in vitro fertilization (IVF).
There’s no proven way to prevent PCOS, but you can take small steps to reduce your symptoms. For example, eating nutritious foods, exercising regularly and managing a healthy weight for your body can help you avoid the effects of PCOS.
CONCLUSION
One of the best ways to cope with PCOS is to maintain a healthy bodyweight, eat nutritious foods and exercise regularly. These changes to your lifestyle can affect hormone levels, in turn regulating your menstrual cycle and easing your symptoms. If excess hair growth or acne is hurting your confidence, cosmetic treatments or working with a dermatologist might be helpful. Finally, if you’re trying to conceive and have PCOS, know that you’re not alone. Nearly 1 in 10 people have PCOS. Polycystic ovary syndrome is a common reproductive and metabolic disorder resulting from polygenic and environmental influences. Key pathological changes include neuroendocrine dysregulation, excess production of androgens, insulin resistance, and changes in adipose tissue biology, with variation in dysfunction of these pathways contributing to differences in phenotypic expression and severity of the disease. Advances in genetic understanding, together with new techniques to assess the steroid metabolome, have identified new biological targets, challenged the perception of polycystic ovary syndrome as one entity, and could facilitate an individualised approach to long term cardiometabolic surveillance based on the metabolomic signature. These advances could, for the first time, enable the development of specific drug treatments for the disorder based on an improved understanding of the underlying pathophysiology. Well designed, multicentre, patient centred clinical trials of neurokinin receptor antagonists, kisspeptin based treatments, and repurposed antidiabetic drugs are now needed to investigate new therapeutic options for polycystic ovary syndrome.
REFERENCES

Rudraksh PK Chavda, Bhavya P Patel, Kachhadiya Hemanshi, Patel Nirali, Dr. Ashok Choudhary, Dr. Divyakant Patel, Pregnancy Complications and Outcomes in Women with Polycystic Ovary Syndrome: An Updated Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 1696-1709. https://doi.org/10.5281/zenodo.17369994
 10.5281/zenodo.17369994
10.5281/zenodo.17369994
