
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Abhinav Education Society's College of Pharmacy, Narhe, Pune, Maharashtra, India. 411041
Gajanan Maharaj College of Pharmacy Chh.Sambhajinagar, Maharashtra, India. 431005
Shri. Babanrao Pachpute Vichardhara Trust’s Group of Institutions, Faculty of Pharmacy, Kashti, Shrigonda, Ahmednagar, Maharashtra, India. 414701
Central India College of Pharmacy, Lonara, Nagpur, Maharashtra, India.
Shri Vile Parle Kelavani Mandal's Institute of Pharmacy, Dhule, Maharashtra, India 424001
Ketamine, originally developed as an aesthetic in the 1960s, has since evolved into a multipurpose agent with significant roles in anaesthesia, analgesia, and psychiatry. Its unique pharmacological profile, particularly as an NMDA receptor antagonist, provides rapid onset and preserves cardiovascular and respiratory functions—making it indispensable in emergency and low-resource settings. In recent decades, ketamine has shown promise as a rapid-acting antidepressant, especially for treatment-resistant depression. The approval of esketamine and exploration of safer analogues, novel delivery systems, and personalized pharmacogenomic approaches represent the forefront of psychiatric innovation. However, ketamine's potential for misuse and long-term cognitive effects remain challenges. This review critically evaluates ketamine’s pharmacodynamics, clinical uses, adverse effects, historical development, and future directions in personalized psychiatric care.
Importance of Ketamine in Medicine: Ketamine, a versatile anaesthetic agent, has garnered widespread recognition due to its broad spectrum of applications in both human and veterinary medicine. Initially synthesized in the 1960s, ketamine was introduced into clinical practice for general anaesthesia due to its unique pharmacodynamic properties, particularly its dissociative anaesthetic effects. Unlike traditional anaesthetics, ketamine induces a state of profound analgesia and amnesia while preserving respiratory and cardiovascular stability. This distinctive feature made it especially valuable in challenging environments such as battlefield medicine and emergency care, where rapid intervention and patient stabilization are paramount. Over the years, ketamine's use has expanded beyond anaesthesia to include indications in pain management, mental health, and even as a rapid-acting treatment for depression.
In the realm of psychiatry, ketamine has emerged as a breakthrough treatment for individuals with treatment-resistant depression (TRD). Studies have demonstrated that low-dose ketamine can produce rapid antidepressant effects, sometimes within hours, offering hope for patients who have failed traditional pharmacological therapies (Berman et al., 2000; Murrough et al., 2013). This rapid onset distinguishes ketamine from conventional antidepressants, which often take weeks to show therapeutic effects. Furthermore, the discovery of esketamine, a nasal spray form of ketamine approved by the FDA in 2019, highlights its growing importance in modern psychiatric practice (FDA, 2019).
Objective of the Review
This review aims to provide a comprehensive examination of ketamine's pharmacology, clinical uses, and potential risks. By exploring the drug’s chemical structure, mechanism of action, and applications in anaesthesia, analgesia, and psychiatry, the review will highlight both the therapeutic potential and the challenges associated with its use. Additionally, it will focus on the historical development of ketamine, from its initial discovery to its current status as a vital therapeutic agent in both medical and psychiatric settings. The review also seeks to discuss ongoing research exploring ketamine’s expanding range of indications and its role in the future of mental health treatment.
Scope of the Discussion
This discussion will cover several key areas:
The review will also explore the safety and regulatory issues surrounding ketamine, including its classification as a controlled substance and its potential for misuse in recreational settings.
HISTORY
"Ketamine’s origins trace back to the 1950s, when researchers at Parke-Davis Laboratories in Detroit, Michigan, explored cyclohexylamines in their search for an ideal anaesthetic with analgesic effects."
On March 26, 1956, chemist Maddox developed a method that led to the synthesis of phencyclidine (PCP), chemically known as N-(1-phenyl-cyclohexyl)-piperidine. Later, on September 11, 1958, Parke-Davis pharmacologist Dr. Chen received the compound, labelled CI-395, from Maddox. Around the same time, both Dr. Chen and Dr. Domino began investigating its effects in animal models. Their studies revealed that phencyclidine produced strong analgesic effects—monkeys underwent laparotomy procedures without exhibiting signs of pain. However, the animals entered a cataleptic state, characterized by open eyes and limited muscle relaxation. Dr. Chen described this cataleptic state as an 'akinetic condition marked by the loss of postural reflexes, yet with preserved consciousness, where the limbs appear paralyzed due to both motor and sensory suppression.
Following its initial development, Parke-Davis explored the use of phencyclidine (PCP) as a human anaesthetic under the trade name Sernyl. In 1958, the first clinical trials involving humans were published by Dr. Edward Greifenstein, a professor of anaesthesiology at Wayne State University in Detroit. PCP was observed to elevate blood pressure, respiratory rate, and minute ventilation, while preserving corneal and laryngeal reflexes. Side effects such as nystagmus and hypersalivation were noted. These trials demonstrated a true anaesthetic state marked by catalepsy, profound amnesia, and strong analgesia. Greifenstein, alongside neurologist Dr. John Stirling Meyer, concluded that PCP induced a sensory deprivation syndrome mediated through central neural mechanisms.
Surgical procedures, including full operations in 30 of Greifenstein’s patients, were successfully conducted using Sernyl alone. However, in 13 patients, the anaesthetic effect was inadequate—five experienced intense excitatory reactions. Postoperative management was challenging in 10 patients, with recovery durations ranging from 3 to 18 hours. Notably, electroencephalographic (EEG) readings in these cases did not resemble those typical of barbiturate-induced anaesthesia or natural sleep patterns.
Further clinical observations were reported in 1959 by Johnstone and Evans in the British Journal of Anaesthesia. They described Sernyl as one of the most potent general analgesics known in clinical medicine at the time. Unlike traditional sedatives and analgesics, it did not suppress cardiovascular or respiratory function and maintained pharyngeal and laryngeal reflexes, making it particularly useful in elderly patients. Despite these advantages, prolonged excitation and psychotic symptoms following a single dose limited its clinical application.
As clinical understanding evolved, it became evident that phencyclidine was not ideal for human anaesthesia. Parke-Davis subsequently developed eticyclidine (CI-400 or PCE), chemically identified as N-ethyl-1-phenyl-cyclohexylamine. Though it shared PCP’s lack of respiratory and circulatory suppression, PCE also induced frequent hallucinations and a catatonic state with generalized rigidity, limiting its use. The emergence of ketamine around the same period further overshadowed its clinical potential. In 1960, Collins and colleagues described the induced state as a trance-like dissociation from the external environment. EEG data revealed the presence of delta waves, thought to correlate with the analgesic effect, possibly due to cortical dissociation or disruption of thalamic or thalamocortical pathways. Eventually, PCE was classified as a Schedule I substance in the 1970s due to its high potential for abuse and limited medical utility.
In the 1960s, Dr. Cal Bratton at Parke-Davis supported efforts to improve PCP derivatives with fewer side effects. Chemist Calvin Stevens, a professor at Wayne State University, synthesized various phencyclidine-related compounds. One of them, CI-581 (later named ketamine), showed strong, short-acting anaesthetic effects in animals and was selected for human trials.
In 1964, Drs. Domino and Corssen conducted the first human trial at Jackson Prison, Michigan. Participants reported out-of-body sensations. Domino’s wife coined the term "dissociative anaesthetic" to describe ketamine’s effects. This led to its formal clinical characterization.
After early trials, researchers worldwide began studying ketamine. It reached France in 1970 and the UK in 1969, though British reception was poor due to hallucinations. Ketamine was patented in Belgium in 1963, approved by the FDA in 1970, and used as a battlefield anaesthetic during the Vietnam War due to its safety and effectiveness.
Though effective, its emergence reactions led doctors to pair it with sedatives like diazepam or droperidol. Later studies clarified ketamine’s pharmacokinetics, ideal routes of administration, and use in emergencies like shock or asthma. Concerns about raised intracranial pressure and epilepsy followed.
By the 1980s, ketamine’s interaction with NMDA receptors became a major focus. It helped researchers understand synaptic plasticity, memory, and disorders like schizophrenia. Its role in managing pain resurfaced in the 1990s, especially after recognizing that opioids could worsen pain via NMDA pathways—making ketamine useful as an anti-hyperalgesic.
Ketamine’s antidepressant effects were first noted in the 1990s and confirmed in later clinical trials. Unlike typical antidepressants, ketamine works within hours, offering hope for suicidal patients.
Today, ketamine is a key tool in anaesthesia and pain management globally. While its use declined in wealthier nations due to side effects, it's making a comeback thanks to new understanding of its mechanisms. In low-resource settings, it remains essential. Future developments may include new analogues or safer versions to eliminate side effects entirely.
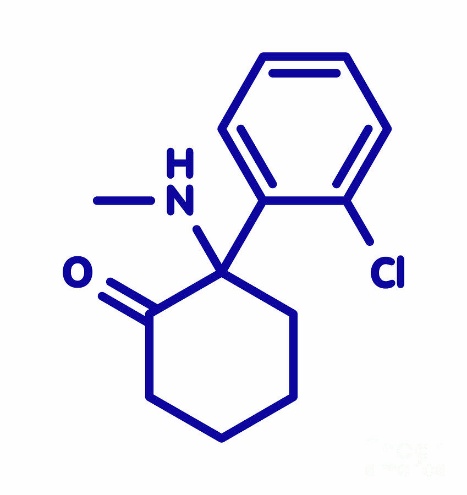
STRUCTURE AND PROPERTY’S MOLECULAR STRUCTURE AND ISOMERS
Ketamine is a chiral compound derived from the aryl cyclohexylamine class, chemically known as (RS)- 2- (2-chlorophenyl)- 2 (methylamino) cyclohexanone. It possesses a cyclohexanone backbone substituted with a methylamino group and a 2-chlorophenyl ring, creating a stereogenic centre at the carbon bearing the amino group. This configuration allows ketamine to exist as two optical isomers: S- (+)-ketamine and R- (–)-ketamine. The S-enantiomer, also referred to as esketamine, exhibits a higher affinity for the NMDA receptor and is considered more potent in terms of both anaesthetic and antidepressant effects. In contrast, the R-enantiomer demonstrates lower NMDA receptor activity but has shown promising and longer-lasting antidepressant properties in preclinical research.
Physicochemical Characteristics: Ketamine has a molecular weight of approximately 237.7 g/mol. It appears as a colourless to slightly yellow liquid in its injectable form and can also exist as a crystalline solid. Its solubility in water and lipids contributes to its rapid onset of action when administered intravenously or intramuscularly. The drug is moderately lipophilic, which facilitates its passage across the blood-brain barrier (Coppola & Mendola, 2012).
Mechanism of Action: The primary mechanism of ketamine involves noncompetitive antagonism of the N-methyl-D-aspartate (NMDA) receptor, which is a subtype of glutamate receptor in the central nervous system. By blocking NMDA receptor activity, ketamine inhibits excitatory neurotransmission, contributing to its anaesthetic and dissociative effects. Additionally, ketamine interacts with other receptor systems, including opioid, monoaminergic, and cholinergic receptors, which may contribute to its analgesic and antidepressant properties
PHARMACODYNAMICS AND PHARMACOKINETICS OF KETAMINE
Pharmacodynamics: Ketamine primarily acts as a non-competitive antagonist of the NMDA receptor, a subtype of glutamate receptor in the central nervous system. By blocking NMDA receptors, ketamine inhibits excitatory neurotransmission, which is responsible for its anaesthetic, analgesic, and antidepressant effects.
Additionally, ketamine interacts with opioid receptors, monoaminergic receptors (e.g., serotonin, dopamine), and even voltage-gated calcium channels, contributing to its complex clinical effects (Zorumski et al., 2016).
Pharmacokinetics (ADME):
Route of Administration: Ketamine can be administered through several routes:
Other experimental routes include sublingual, subcutaneous, and even rectal administration
Onset, Duration, and Half-life:
CLINICAL APPLICATION
Ketamine has emerged as a versatile agent in modern medicine, with applications extending across anaesthesia, pain management, psychiatry, and several critical care scenarios.
ADVANTAGES OF KETAMINE
Ketamine offers several unique advantages that distinguish it from many other anaesthetic and therapeutic agents in modern medicine.
SIDE EFFECTS AND LIMITATIONS OF KETAMINE
While ketamine has many clinical benefits, its use is associated with a range of side effects and limitations that must be carefully considered in both acute and long-term treatment settings.
ABUSE AND REGULATORY ISSUES OF KETAMINE
While ketamine has proven to be an important medical tool, its potential for abuse and associated public health challenges have led to strict regulatory oversight.
FUTURE DIRECTIONS IN KETAMINE-BASED THERAPIES
1. Development of Safer Ketamine Analogues: Ketamine's rapid antidepressant effects have been well-documented; however, concerns about its side effects—such as dissociation, cognitive impairments, and abuse potential—have prompted research into safer alternatives. Notably, the (R)-enantiomer of ketamine has shown promise in preclinical studies, demonstrating prolonged antidepressant effects with fewer side effects compared to the (S)-enantiomer. Additionally, ketamine's metabolites, particularly (2R,6R)-hydroxynorketamine, have been identified as potential contributors to its antidepressant effects, offering a pathway to developing treatments that retain efficacy while minimizing adverse outcomes.?
2. Advancements in Delivery Systems: The traditional intravenous administration of ketamine poses challenges in terms of accessibility and patient compliance. Recent innovations in drug delivery systems aim to address these issues. Transdermal delivery methods, such as microneedles and laser microoperation, have been explored to facilitate the absorption of ketamine through the skin, offering a non-invasive alternative to intravenous administration. These methods have shown potential in enhancing patient comfort and adherence to treatment protocols.?
3. Expansion of Psychiatric Indications: While ketamine and esketamine have been primarily utilized in the treatment of depression, ongoing research is exploring their efficacy in a broader range of psychiatric disorders. Clinical trials are investigating the use of ketamine-based therapies for conditions such as anxiety disorders, post-traumatic stress disorder (PTSD), and bipolar disorder. These studies aim to determine the safety and effectiveness of ketamine in diverse psychiatric populations, potentially expanding its therapeutic applications.?
4. Personalized Treatment Through Pharmacogenomics: The variability in individual responses to ketamine underscores the need for personalized treatment approaches. Pharmacogenomic research has identified genetic factors that may influence the efficacy and safety of ketamine therapy. For instance, polymorphisms in the BDNF gene and the CYP2B6 enzyme have been associated with differences in treatment response and the occurrence of side effects. Incorporating pharmacogenomic data into clinical practice could enable clinicians to tailor ketamine treatments to the genetic profiles of patients, optimizing therapeutic outcomes and minimizing adverse effects.?
In summary, the future of ketamine-based therapies lies in the development of safer analogues, innovative delivery systems, expanded indications across psychiatric disorders, and personalized treatment strategies informed by pharmacogenomics. These advancements hold the potential to enhance the therapeutic utility of ketamine while mitigating its risks, paving the way for more effective and individualized care in the field of psychiatry.
CONCLUSION
Ketamine has undergone a remarkable transformation from its early use as a battlefield anaesthetic to its current status as a multifaceted drug with psychiatric, anaesthetic, and even controversial recreational roles. Initially approved in the 1970s for anaesthesia, ketamine’s unique mechanism—primarily through NMDA receptor antagonism—opened doors to novel psychiatric applications decades later.
In recent years, ketamine and its S-enantiomer, esketamine, have gained prominence as rapid-acting antidepressants, particularly in cases of treatment-resistant depression (TRD). Esketamine’s FDA approval in 2019 for TRD and its expansion as a monotherapy in 2024 underscore this shift (FDA, 2019, Janssen, 2024). The rapid onset of symptom relief—sometimes within hours—marks a significant breakthrough compared to traditional antidepressants that may take weeks to show effects.
Clinical Importance and Resurgence: Ketamine’s resurgence in modern psychiatry highlights its clinical importance beyond anaesthesia. It offers hope for patients unresponsive to conventional treatments, including those with severe depression, suicidal ideation, PTSD, and chronic pain disorders. Clinical trials have validated its efficacy, while new delivery methods such as nasal sprays, lozenges, and oral prodrugs aim to improve access and patient adherence (PubMed Central, 2023).
Furthermore, ongoing research is focusing on developing safer ketamine analogues, understanding its long-term effects, and applying pharmacogenomic insights to personalize treatment strategies. This indicates a promising direction toward maximizing benefits while minimizing risks, including potential misuse and dependency (PubMed, 2022).
Final Thoughts on Ketamine’s Evolving Role: Ketamine’s journey—from a misunderstood hallucinogen to a fast-acting antidepressant—exemplifies how scientific innovation and clinical necessity can drive the re-evaluation of older drugs. While challenges remain—such as misuse potential, accessibility, and stigma—ongoing research and medical supervision continue to expand its safe use in therapeutic contexts.
Its evolving role is a testament to the dynamic nature of medicine: where old tools, when reimagined through modern science, can offer new hope.
REFERENCES





Tejas Pagar, Satyajit Waje, Parmeshwar Mane, Zaid-Ameen Gulam Wasi, Prerana Chaudhari, Ketamine in Modern Medicine: Antidepressant Breakthrough, Anaesthetic Staple, or Substance of Misuse, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4835-4847. https://doi.org/10.5281/zenodo.15547737
 10.5281/zenodo.15547737
10.5281/zenodo.15547737