
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Krupanidhi College Of Pharmacy, Bangalore 560035.
Lithium has remained a cornerstone of mood stabilization for over half a century, primarily in bipolar disorder. Increasing evidence suggests its therapeutic benefits extend across multiple psychiatric conditions. Despite advances in psychopharmacology, lithium continues to occupy a unique position due to its efficacy, neuroprotective potential, and anti-suicidal properties. This review aims to synthesize the available evidence on lithium as a mood stabilizer across psychiatric disorders, highlighting its clinical efficacy, underlying mechanisms, and therapeutic relevance beyond bipolar disorder. A systematic search of PubMed, Scopus, and Web of Science databases was conducted to identify clinical trials, meta-analyses, and observational studies from 1990 to 2025. Studies evaluating lithium in bipolar disorder, major depressive disorder, schizoaffective disorder, and related psychiatric conditions were included. Findings were categorized by disorder and outcome measures. Lithium demonstrates robust efficacy in preventing relapse and stabilizing mood in bipolar disorder. Evidence also supports its augmentation role in treatment-resistant depression and its potential in schizoaffective disorder. Long-term use is associated with reduced suicide risk, independent of diagnosis. Emerging data indicate possible benefits in borderline personality disorder and neuroprotective effects in neuropsychiatric populations. However, concerns remain regarding side effects, narrow therapeutic index, and declining clinical use. Lithium remains the most evidence-based mood stabilizer across psychiatric disorders, with proven efficacy and unique anti-suicidal properties. Broader clinical application and renewed research may reinforce its role as a transdiagnostic treatment.
One of the most important turning points in contemporary psychiatry is thought to have been the identification of lithium as a psychotropic drug. A new era in the treatment of mood disorders began in 1949 when Australian psychiatrist John Cade first showed that lithium had therapeutic effects in mania¹. As the first successful mood stabilizer, lithium quickly established itself as a mainstay in the treatment of bipolar disorder² in the decades that followed. Pharmacological interventions were developed as targeted treatments for specific psychiatric conditions³, marking the beginning of biological psychiatry and a paradigm change in psychiatry.
Because of its strong effectiveness in both the acute and maintenance stages of bipolar disorder, lithium is still regarded as the "gold standard" among mood stabilizers. In addition to lowering manic and depressive episodes, lithium has special qualities that set it apart from other antipsychotics and mood stabilizers4. These include its neuroprotective potential, its well-established anti-suicidal action, and its capacity to lower relapse rates?,?. There is proof that it has a wide range of psychotropic and neurological advantages including promoting neurogenesis, regulating inflammatory pathways, and regulating circadian rhythms7. Lithium's multidimensional efficacy has been continuously confirmed by decades of clinical trials and real-world studies, even in the face of the advent of newer medicines.
Crucially, the benefits of lithium are not limited to bipolar disorder. Therapeutic effects in cyclothymia, schizoaffective disorder, unipolar depression, and even neurodegenerative diseases like Alzheimer's disease are suggested by preclinical and clinical data?,?. Its psychiatric importance has been further highlighted by its augmentation function in treatment-resistant depression and possible preventative benefits in suicidality¹?. Ironically, however, lithium is still underutilized in modern therapeutic settings. Clinical concerns regarding side effects (thyroid and renal toxicity), the necessity of routine serum monitoring, and the impact of more recent pharmaceutical options are all contributing factors¹¹,¹². Despite recommendations for lithium as a first-line treatment for bipolar disorder and mounting evidence of its unmatched benefits, this under prescription trend continues¹³.
In order to restore lithium's place in contemporary psychiatry, a thorough synthesis of the available data is required, taking into account the conflicting facts of its broad usefulness across illnesses and its waning clinical use.
This review's goal is to present a current, fact-based assessment of lithium's effectiveness in treating a variety of mental illnesses. This study attempts to illustrate the long-lasting significance of lithium in psychiatry by outlining its historical development, reinforcing its status as the gold standard in bipolar disorder, and showing its wider therapeutic benefits. We will also discuss obstacles to its best use and investigate methods for incorporating lithium into clinical practice more successfully. Lithium's status as a pillar of precision psychiatry is thus reaffirmed in this review, which aims to close the gap between evidence and practice.
Pharmacology and Mechanisms of Action
Because of its distinct pharmacological profile, lithium, the oldest mood stabilizer in psychiatry, is still a mainstay in the treatment of bipolar disorder and associated disorders. Its pharmacokinetics and several molecular processes, which together explain its neuroprotective and anti-suicidal effects, are intimately related to its clinical value.
Pharmacokinetics
Peak plasma concentrations of lithium are reached in 1-3 hours for immediate-release formulations and a little longer for sustained-release formulations due to the quick absorption of lithium from the gastrointestinal tract14,15. With a volume of distribution of roughly 0.6–0.9 L/kg16, distribution mostly takes place in total body water. Lithium has predictable kinetics since it is not protein-bound and does not undergo hepatic metabolism like the majority of psychotropic drugs do17. Nearly all excretion occurs in the kidneys, with sodium transport routes reabsorbing 80% of it in the proximal tubules18. This explains why the therapeutic index is narrow (0.6–1.2 mmol/L for maintenance) and why frequent serum monitoring is necessary to prevent toxicity, especially in patients with renal impairment or abnormalities of sodium balance19,20.
Molecular Targets
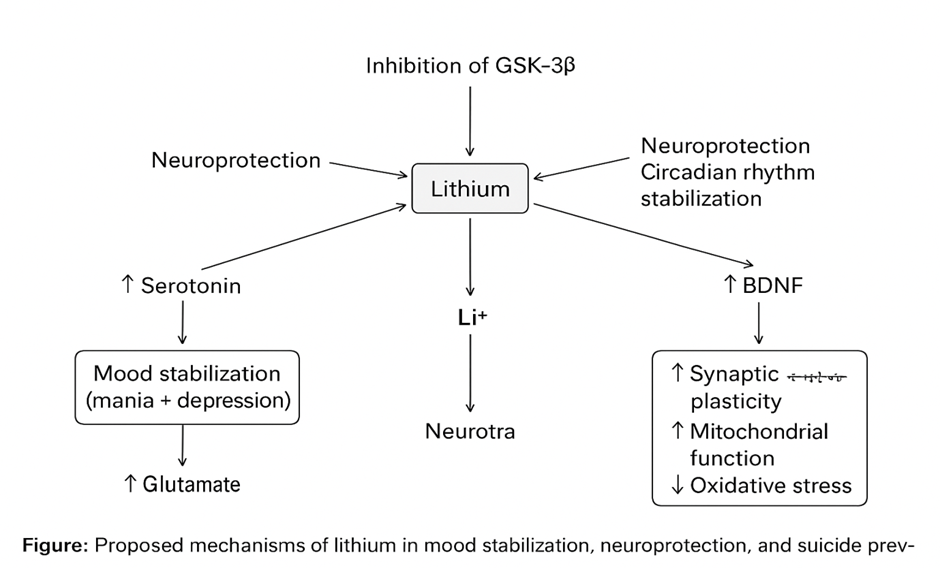
A number of intracellular processes related to mood regulation are impacted by lithium. Lithium inhibits inositol monophosphates, which lowers inositol recycling and weakens phosphatidylinositol signalling cascades, according to the inositol depletion hypothesis21,22. At the same time, lithium suppresses GSK-3, a serine/threonine kinase involved in neural plasticity, apoptosis, and circadian regulation23,24. Lithium alters neuroplasticity, neurotransmission, and stress response pathways by inhibiting GSK-325. Lithium also contributes to long-term neuronal survival by controlling calcium signalling, improving mitochondrial function, and reducing oxidative stress26,27.
Neurotrophic and Neuroprotective Effects
By increasing brain-derived neurotrophic factor (BDNF), which improves synaptic resilience and neuronal survival, long-term lithium therapy produces neurotrophic effects28. Gray matter volume preservation has been repeatedly shown in neuroimaging investigations, especially in the prefrontal cortex and hippocampus, areas linked to mood regulation and cognitive control29,30. To further support its neuroprotective profile, lithium also decreases inflammatory signalling and increases the expression of anti-apoptotic genes31. These results imply that lithium may alter the course of sickness by maintaining brain structure and function in addition to providing immediate mood stabilization32.
Mood Stabilization and Suicidality Reduction
Lithium's strong therapeutic effectiveness is based on the combination of these pharmacological and neurobiological effects. Lithium has the unique ability to lower the risk of suicide, which is not always the case with other mood stabilizers or antidepressants, in addition to reducing manic and depressed episodes33. According to meta-analyses, lithium lowers suicide rates by over 60% without affecting mood stability. This may be due to neuroprotection, serotonergic modulation, and a decrease in impulsive-aggressive behaviors32,33.
Lithium's pharmacological profile thus demonstrates why it continues to be the "gold standard" mood stabilizer, providing the ability to both regulate symptoms and change disease. Its many different mechanisms set it apart from other psychotropics and keep researchers interested in it.
Evidence in Bipolar Disorder
Acute Mania
Lithium remains the prototypical mood stabilizer in bipolar disorder and has been extensively studied for more than five decades. Its efficacy in acute mania, both as monotherapy and in combination with other agents, is well documented. Furthermore, lithium has been compared with other standard treatments such as valproate, carbamazepine, and antipsychotics, highlighting its central role in the management of acute manic episodes.
Efficacy in Monotherapy and Adjunctive Use
Clinical trials consistently demonstrate that lithium is effective in reducing manic symptoms when used as monotherapy. Early placebo-controlled studies confirmed its superiority over placebo in reducing acute manic symptoms within one to two weeks of initiation34. Furthermore, adjunctive use of lithium with antipsychotics such as haloperidol or atypical antipsychotics enhances clinical response, especially in severe manic episodes35. The combination approach is often adopted in clinical practice, where rapid symptom control is required36.
Comparative Trials
Lithium vs Valproate
Lithium has been compared extensively with valproate in acute mania. While both agents are effective, several trials suggest that lithium may be more potent in classic euphoric mania, whereas valproate may have relative advantages in mixed states and rapid cycling37. The BALANCE trial confirmed lithium’s superiority over valproate in relapse prevention, though acute efficacy was generally similar38.
Lithium vs Carbamazepine
Carbamazepine, another anticonvulsant with mood-stabilizing properties, has been evaluated against lithium. Comparative trials demonstrate broadly similar efficacy, though lithium appears to have a faster onset of action in acute mania39. Carbamazepine may be better tolerated in some patients, but it is generally reserved for second-line use due to drug–drug interactions and tolerability issues40.
Lithium vs Antipsychotics
Antipsychotics, both typical and atypical, are highly effective in acute mania and often provide faster symptom relief than lithium alone. However, head-to-head trials indicate that lithium is comparable in efficacy over several weeks, though antipsychotics achieve more rapid sedation and agitation control41. Lithium is frequently combined with antipsychotics to optimize both rapid symptom relief and long-term stabilization42.
Bipolar Disorder
The role of lithium in bipolar depression has been widely studied, though evidence presents mixed results. While lithium is a cornerstone in mania prevention, its efficacy in acute bipolar depression is less robust. Early controlled trials indicated some benefit, but effect sizes were modest compared to its strong prophylactic effects against mania43.
Monotherapy studies often report limited efficacy of lithium in treating acute depressive episodes in bipolar disorder44. Meta-analyses show that while lithium can reduce depressive symptoms in some patients, response rates are generally lower than for manic symptoms45. This has led to the frequent use of augmentation strategies, such as combining lithium with antidepressants or anticonvulsants46.
The STEP-BD study found that adding antidepressants to a mood stabilizer, including lithium, did not significantly improve outcomes compared with mood stabilizer monotherapy47. However, lithium continues to play a role in combination strategies, particularly when augmentation with selective serotonin reuptake inhibitors (SSRIs) or bupropion is attempted48.
Lamotrigine has shown superiority over lithium in preventing depressive relapses, although lithium remains more effective against manic recurrence49. The balance between these agents highlights the need for individualized treatment approaches, where lithium may serve as a base therapy complemented by other agents to address depressive polarity.
Importantly, lithium’s role extends beyond acute symptom relief. Long-term studies suggest lithium reduces recurrence of depressive episodes and contributes to overall stability, particularly when compared to placebo or some anticonvulsants50. Furthermore, its unique anti-suicidal effect provides additional justification for its continued use in patients with predominant depressive polarity51.
Maintenance Therapy
Lithium remains the gold standard for maintenance therapy in bipolar disorder, with decades of evidence supporting its role in preventing relapse into both mania and depression52. Its unique position among mood stabilizers is reinforced by long-term studies and meta-analyses showing superior prophylactic efficacy and improvement in long-term outcomes53.
One of lithium’s greatest strengths is its ability to reduce recurrence of both poles of illness. Early trials demonstrated lithium’s superiority over placebo in preventing manic relapses, and subsequent studies confirmed its benefit in preventing depressive recurrences as well54. Comparative studies highlight that while anticonvulsants such as carbamazepine and valproate are effective, lithium shows more consistent results across both mania and depression55.
The BALANCE trial provided robust evidence that lithium monotherapy was more effective than valproate monotherapy in preventing relapse, with combination therapy offering the strongest protection56. Similarly, long-term trials comparing lithium and lamotrigine suggest that lithium is particularly effective against manic recurrence, while lamotrigine may have a stronger effect against depressive relapse57. This underlines the importance of individualized treatment strategies, but positions lithium as the foundation for maintenance therapy.
Long-term outcomes with lithium are favorable. Patients maintained on lithium demonstrate fewer hospitalizations, longer time to recurrence, and better functional recovery compared with those treated with other mood stabilizers58. Additionally, lithium’s protective effect against suicide contributes significantly to improved mortality outcomes59.
Evidence also suggests benefits beyond bipolar disorder. In recurrent unipolar depression, lithium has been effective as a prophylactic agent and in reducing suicidal behavior60. Population-based studies further emphasize lithium’s broad utility across mood disorders, reinforcing its status as a uniquely versatile treatment61.
Suicide Prevention
Among its many therapeutic properties, lithium has the strongest evidence base for suicide prevention in bipolar disorder and related mood disorders. Unlike other mood stabilizers, lithium has demonstrated consistent reductions in suicide risk across randomized controlled trials, long-term observational cohorts, and meta-analyses62,63.
A landmark meta-analysis by Cipriani et al. found that lithium significantly reduced suicides and deliberate self-harm compared to placebo or other pharmacological agents64. This effect was evident not only in bipolar disorder but also in recurrent unipolar depression, suggesting a broad protective mechanism. Subsequent systematic reviews reinforced this finding, showing lithium reduced suicide risk by nearly 60% compared with alternatives such as carbamazepine or valproate65.
Population-based registry studies further confirm lithium’s unique anti-suicidal effect. For example, Baldessarini and colleagues reported substantially decreased suicide rates during long-term lithium treatment compared to periods off treatment66. Kessing et al. found that lithium was associated with the lowest rates of suicidal behavior among all mood-stabilizing medications in large Danish registry cohorts67.
The mechanism underlying lithium’s protective effect is not fully understood but may involve serotonergic modulation, reduction of impulsivity, and stabilization of affective dysregulation68. Additionally, lithium’s role in recurrence prevention indirectly lowers suicide risk, as relapses into depressive or mixed states are strongly linked with suicidal behavior69.
Importantly, lithium’s anti-suicidal efficacy has not been consistently replicated with other agents. Anticonvulsants such as valproate and lamotrigine lack comparable evidence, and atypical antipsychotics, while useful in mood stabilization, do not demonstrate the same reduction in suicide rates70. This positions lithium as uniquely effective among psychiatric medications for suicide prevention.
|
Domain |
Meta-Analytic Findings |
|
Acute Mania (Bipolar I) |
Lithium significantly superior to placebo; effect sizes comparable to antipsychotics, though slower onset. |
|
Maintenance Therapy (Bipolar Disorder) |
Lithium most effective single agent for relapse prevention (mania + depression); superior to valproate and carbamazepine. |
|
Bipolar Depression |
Limited acute efficacy; stronger effect in relapse prevention; often combined with lamotrigine or antidepressants. |
|
Unipolar Depression (TRD) |
Lithium augmentation increases remission rates (40–50% vs 14% placebo); accelerates antidepressant response. |
|
Suicide Prevention |
Lithium reduces suicide attempts and completions by >60%; effect independent of mood stabilization. |
|
Comparative Effectiveness |
Network meta-analyses confirm lithium’s superior balance of efficacy and long-term outcomes compared with other mood stabilizers. |
Evidence in Major Depressive Disorder
Lithium is historically recognized as the gold standard in the treatment of bipolar disorder, but its role extends into unipolar major depressive disorder (MDD). In this context, lithium is most often used as an augmentation strategy in treatment-resistant depression (TRD), where first-line antidepressants fail to produce sufficient response. Over several decades, lithium has demonstrated robust evidence not only for symptom improvement but also for reducing suicidal risk in patients with unipolar depression71.
Lithium Augmentation in Treatment-Resistant Depression
Treatment-resistant depression, typically defined as non-response to at least two adequate antidepressant trials, presents a significant clinical challenge. Lithium augmentation is one of the best-validated strategies in this population72. Early randomized controlled trials (RCTs) demonstrated that lithium significantly improves response rates when combined with tricyclic antidepressants73. Later research extended this efficacy to selective serotonin reuptake inhibitors (SSRIs) and serotonin–norepinephrine reuptake inhibitors (SNRIs), making lithium augmentation a standard second-line approach in clinical guidelines74.
The proposed mechanisms include modulation of serotonergic neurotransmission, regulation of glutamatergic signaling, and neuroprotective effects via glycogen synthase kinase-3 (GSK-3) inhibition75. These mechanisms may explain lithium’s ability to potentiate antidepressant effects and promote mood stabilization even in unipolar depression.
Meta-Analyses: Effect Size and Remission Rates
Meta-analyses consistently support the efficacy of lithium augmentation. A meta-analysis by Bauer and Döpfmer reported a pooled response rate of 41.2% with lithium augmentation compared to 14.4% with placebo76. Crossley and Bauer further confirmed that lithium provides both faster onset and higher remission rates compared to placebo when added to antidepressant therapy77.
Subsequent systematic reviews reinforced these findings, reporting effect sizes in the moderate-to-large range, with remission rates often exceeding 40% among patients with TRD78. Importantly, lithium appears to maintain its efficacy across different classes of antidepressants, suggesting a broad applicability as an augmentation agent79.
Role in Reducing Suicidal Risk in Unipolar Depression
Lithium’s most distinctive benefit lies in its anti-suicidal properties. Suicide risk is significantly elevated in MDD, and long-term lithium treatment has been associated with marked reductions in both suicide attempts and deaths80. A comprehensive meta-analysis by Cipriani et al. showed that lithium reduced suicide risk by more than 60% compared to placebo or alternative treatments81. This effect seems to extend beyond symptom relief, indicating a unique mechanism that directly influences suicidality.
Population-based studies confirm these findings, showing lower suicide rates in patients with unipolar depression treated with lithium compared to other mood stabilizers or antidepressants82. This property alone makes lithium a uniquely valuable option in MDD, especially for patients at high risk of suicide.
Clinical Implications
Despite strong evidence, lithium remains underutilized in MDD due to concerns about tolerability, narrow therapeutic index, and the need for serum monitoring. However, its proven efficacy in TRD, robust meta-analytic support, and unparalleled role in suicide prevention highlight its importance. Clinical guidelines consistently recommend lithium augmentation as a key second-line or third-line treatment in resistant depression, and as a first-line consideration in patients with elevated suicide risk83.
Evidence Across Psychiatric Disorders
Lithium has mostly been utilized as a mood stabilizer for people with schizoaffective disorder who exhibit strong emotional characteristics. When used alongside antipsychotic medicine, lithium has been shown in clinical trials to enhance the control of affective symptoms. Lithium augmentation in schizoaffective disorder, especially the manic subtype, has been linked to improved mood stabilization and decreased relapse risk, according to controlled studies84-85. Instead of being used as a monotherapy, this evidence supports its use as an adjuvant treatment for neuroleptics.
Lithium plays a smaller part in schizophrenia. Systematic reviews and meta-analyses reveal no consistent impact on functional outcomes86-87 and no improvement in core psychotic symptoms. Lithium has, however, demonstrated modest but clinically significant reductions in mood lability, aggressiveness, and hostility in schizophrenia patients with high levels of impulsivity or behavioral dysregulation88. Lithium is therefore not advised for the regular treatment of schizophrenia, but it may be taken into consideration as an adjuvant in some situations.
Additionally, lithium has been researched in relation to borderline personality disorder (BPD), focusing on affective instability, aggression, and impulsivity. Lithium use has been linked to decreases in hostile and self-harming behaviors, according to preliminary controlled research89. Subsequent evaluations, however, revealed inconsistent and conflicting results, with small study numbers and methodological problems restricting generalizability90. As a result, lithium is not regarded as a conventional treatment for BPD; nonetheless, it might be a viable alternative for patients who are resistant to treatment and exhibit significant impulsivity or violence.
Lithium has been tested for a number of ailments besides mood and psychotic disorders, including:
Treatment-resistant OCD: Lithium augmentation with SSRIs or clomipramine was investigated in small controlled studies. The evidence is still weak and contradictory generally, even though some patients saw slight improvements91.
Cluster Headaches: Studies have shown that lithium is effective in lowering the frequency of attacks, especially in chronic cluster headache subtypes. Although early observational studies indicated significant clinical benefit, widespread use is limited by side effects and narrow therapeutic margins92.
Adverse Effects, Monitoring, and Challenges
Lithium is known to have a number of acute adverse effects, even when taken within prescribed limits. These include the most often reported gastrointestinal disturbances (diarrhea, vomiting, and nausea), fine tremor, and polyuria/polydipsia93. Serum levels above 1.5 mmol/L cause clinical signs of toxicity, such as lethargy, ataxia, disorientation, dysarthria, and coarse tremor94. If severe intoxication is not treated right once, it can cause seizures, unconsciousness, and even death (>2.5 mmol/L)95. NSAIDs, ACE inhibitors, thiazide diuretics, and renal impairment increase the risk of these toxicities, as does dehydration96.
Long-term lithium use has been associated with negative consequences on multiple systems.
Effect on the endocrine system: Long-term users and women are more likely to develop hypothyroidism as a result of lithium's interference with the production and release of thyroid hormones97. Additionally, reports of hyperparathyroidism and hypercalcemia have been made98.
Long-term treatment raises the risk of chronic renal disease, tubulointerstitial nephropathy, and decreased concentration99. Early onset and persistence of polyuria and nephrogenic diabetic insipidus are possible100.
Weight gain has been linked to lithium use, which has a detrimental influence on long-term results and adherence101.
Effects on the nervous system and skin: Some patients have experienced memory problems, acne, psoriasis flare-ups, and cognitive slowing102.
These toxicities highlight the significance of ongoing observation and prompt problem identification.
Lithium has a limited therapeutic window, therefore careful and ongoing monitoring is crucial. According to current recommendations,
Serum lithium levels should be monitored every three to six months after starting or changing a dose, and then every five to seven days until they stabilize103.
Serum creatinine, eGFR, and urinalysis are examples of renal function tests that should be performed at baseline and subsequently every 6 to 12 months, or more frequently in older or at-risk populations104.
Given the high prevalence of hypothyroidism, thyroid function tests (TSH, free T4) should be performed at baseline and at least once a year105.
Parathyroid hormone and calcium: sometimes, particularly during long-term treatment106.
One of the most practical issues in clinical settings, particularly when resources are scarce, is this monitoring load.
Lithium is still underutilized globally despite a solid body of research supporting it.
Physician hesitancy: A lot of psychiatrists are reluctant to prescribe lithium because they are worried about its toxicity, the possibility of legal action, and the availability of substitutes107.
Patient adherence: Adherence is greatly decreased by side effects like weight gain, polyuria, and tremor, as well as the inconvenience of repeated blood tests108.
Pharmaceutical dynamics: Despite lithium's unparalleled long-term advantages, the marketing of more recent mood stabilizers and atypical antipsychotics has helped to reduce its use109
Limitations in resources: Lithium is less practical than alternatives in low-resource environments because frequent monitoring infrastructure may not be possible110.
FUTURE DIRECTIONS
Even after decades of therapeutic practice, there are still a number of unanswered questions on how to best understand and utilize lithium's function as a mood stabilizer for a variety of mental illnesses. Finding trustworthy biomarkers to forecast treatment response, recurrence risk, and unfavourable outcomes is one of the most urgent needs111. Developments in neuroimaging and genetics could lead to the discovery of molecular signals unique to each patient that account for lithium responsiveness112. Lithium's molecular mechanisms, such as its impact on neurotrophic factors, inflammation, and circadian control, also need further investigation to elucidate how these pathways support mood stabilization113.
Another issue that needs careful investigation is long-term safety monitoring. Lithium is well known, but large-scale prospective studies with standardized outcome reporting are necessary due to concerns about renal, thyroid, and cognitive effects114. The development of new formulations, including targeted delivery systems or sustained-release preparations, may be able to lower toxicity without sacrificing therapeutic efficacy115.
The use of lithium in precision psychiatry is a new area of study. By combining clinical, genetic, and digital health data, it may be possible to identify patients who will benefit from lithium the most while reducing exposure in non-responders116. Another promising tactic for enhancing therapeutic results is the use of digital tools and mobile health platforms to track blood levels, adherence, and early warning indicators of relapse117.
Future studies should compare lithium's efficacy to that of more recent mood stabilizers and adjunctive therapies, particularly in populations with conditions other than bipolar disorder, like schizoaffective disorder and treatment-resistant unipolar depression118. Since no other mood stabilizer has shown such strong effects, it is especially important to increase study into lithium's anti-suicidal qualities119. Lastly, to guarantee consistent clinical use, monitoring, and integration into individualized treatment frameworks, cooperative efforts are required to create international recommendations and standardized protocols120.
CONCLUSION
Lithium continues to be one of the most reliable and long-lasting mood stabilizers, with strong prophylactic effects for bipolar disorder and increasing evidence for other mental illnesses such major depressive disorder, schizoaffective disorder, and suicidality121. Lithium's capacity to lower suicide risk and relapse rates is unmatched, even with the advent of more recent medications122. Preclinical and clinical investigations have also shown its neuroprotective qualities, emphasizing effects on oxidative stress, neurogenesis, and cellular resilience123. As a result, lithium is being investigated as a possible supplemental treatment for neurodegenerative diseases like Parkinson's and Alzheimer's disease124. However, the medication's limited therapeutic range and potential for thyroid, renal, and metabolic issues make careful observation necessary125. Patient adherence is still a problem, which emphasizes the necessity of digital tools, education, and streamlined formulations to maximize long-term results126.
Recent developments in pharmacogenetics raise the possibility that genetic and molecular markers could predict treatment response to some extent, opening the door to customized lithium use in precision psychiatry127. However, despite the growing usage of atypical antipsychotics and anticonvulsants, comparative efficacy studies continue to support lithium's utility as a first-line treatment for mood disorders128.
Lithium is distinguished from other mood stabilizers and antidepressants by its distinct anti-suicidal properties, which are consistently supported by the evidence base129. Stronger clinical recommendations, better monitoring techniques, and fair access to lithium therapy especially in low-resource settings all depend on ongoing international cooperation130.
To sum up, lithium remains a key component in the management of mental and emotional illnesses. Advances in precision psychiatry, digital monitoring, and biomarker identification provide promise for enhancing its usage in future clinical practice, even though safety management and patient selection still present problems.
REFERENCES




Shanila Thankam Suresh, Nandini Goswami, Alvina Christiana B, Jona Joy, Lithium as a Mood Stabilizer: Evidence Across Psychiatric Disorders, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2056-2075. https://doi.org/10.5281/zenodo.17154091
 10.5281/zenodo.17154091
10.5281/zenodo.17154091