
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of Pharmacy and Research, People’s University, Bhopal, Madhya Pradesh, India 462037
Lovastatin, a potent member of the statin drug class, is primarily indicated for the management of hypercholesterolemia through the inhibition of 3-hydroxy-3- methylglutaryl-coenzyme A (HMG-CoA) reductase—an essential enzyme in the mevalonate pathway responsible for cholesterol biosynthesis. Traditionally prescribed for cardiovascular risk reduction, lovastatin has recently gained attention for its multifaceted pharmacological activities beyond lipid regulation. These include osteogenic properties promoting bone tissue regeneration, facilitation of fracture repair, and anti-inflammatory effects beneficial in dermatological conditions. However, its poor aqueous solubility and extensive first-pass metabolism have limited its systemic bioavailability and therapeutic efficacy in non-cardiovascular indications. Recent advancements in transdermal drug delivery systems, particularly microneedle- based patches, have shown promise in enhancing the dermal and systemic absorption of poorly water-soluble drugs like lovastatin. These systems offer targeted delivery, bypass first-pass metabolism, and improve patient compliance. Lovastatin’s pharmacokinetic profile reveals it is a lipophilic prodrug with high hepatic extraction and low oral bioavailability. It belongs to BCS Class II, characterized by low solubility and high permeability, and displays a high partition coefficient (Log P ~4.26). Its solubility is limited in water but adequate in organic solvents such as ethanol, DMSO, and DMF.
Wound healing is a dynamic and intricate physiological process involving hemostasis, inflammation, proliferation, and tissue remodeling. In individuals with chronic conditions such as diabetes mellitus, this process is often impaired due to persistent inflammation, poor vascularization, and oxidative stress. Recent studies have highlighted the therapeutic potential of lovastatin, a member of the statin class, not only for its lipid-lowering properties but also for its angiogenic, anti-inflammatory, and pro-reparative effects, which are particularly beneficial in promoting wound healing.
To overcome the pharmacokinetic limitations associated with oral and parenteral administration of lovastatin—namely, poor aqueous solubility and extensive first-pass metabolism—transdermal drug delivery systems (TDDS) have emerged as a viable alternative. Among these, microneedle (MN) technology has garnered considerable interest due to its ability to provide minimally invasive, painless, and targeted drug administration. Microneedles are capable of breaching the stratum corneum, the outermost barrier of the skin, thereby facilitating the efficient delivery of hydrophilic, lipophilic, and macromolecular agents into the systemic circulation or local tissue microenvironment. This approach holds particular promise for enhancing the therapeutic efficacy of agents like lovastatin in wound management.
Lovastatin is a competitive inhibitor of the enzyme 3-hydroxy-3-methylglutaryl- coenzyme A (HMG-CoA) reductase, which catalyzes the rate-limiting step in the biosynthesis of cholesterol: the conversion of HMG-CoA to mevalonate. By interrupting this critical metabolic pathway, lovastatin effectively reduces intracellular cholesterol synthesis, leading to upregulation of LDL receptors and increased clearance of low- density lipoprotein cholesterol (LDL-C) from the bloodstream. Due to its lipid-lowering action, lovastatin was among the first statins to be approved by the FDA and has since become a cornerstone in the management of hypercholesterolemia and the prevention of atherosclerotic cardiovascular diseases.
Beyond its primary use in dyslipidemia, accumulating evidence suggests that lovastatin exhibits several pleiotropic effects—biological actions independent of cholesterol reduction. These include anti-inflammatory, antioxidant, immunomodulatory, and angiogenic properties, which have expanded its potential therapeutic applications.
Specifically, lovastatin has shown promise in promoting bone tissue regeneration, accelerating fracture healing, and mitigating cutaneous inflammatory conditions through mechanisms such as enhanced vascular endothelial growth factor (VEGF) expression and suppression of pro-inflammatory cytokines.
Moreover, the pharmacological repurposing of lovastatin is gaining momentum in areas such as oncology, neurodegenerative disorders, and wound healing, especially chronic wounds seen in diabetic patients. However, its clinical utility in these areas is limited by poor aqueous solubility and extensive first-pass hepatic metabolism, which reduce its systemic bioavailability. These challenges have sparked interest in novel drug delivery platforms—such as microneedle-based transdermal systems—that aim to enhance localized drug deposition and therapeutic efficacy without compromising patient compliance. This review explores lovastatin’s physicochemical and pharmacological characteristics, with particular emphasis on its emerging role in wound healing and the potential benefits of advanced delivery systems.
MATERIALS AND METHOD
Study Variables:
Concentration of Polyvinyl alcohol
Concentration of Hydroxy propyl methyl cellulose
Drug – Lovastatin
Polymer – METHOCELTM K15M, an HPMC
DRUG PROFILE
Lovastatin: A Multifunctional Lipid-Lowering Agent with Therapeutic Potential in Wound Healing
Lovastatin is a widely prescribed statin drug primarily used for lowering cholesterol levels. Beyond its lipid-lowering capabilities, it exhibits promising properties including bone regeneration, anti-inflammatory action, and enhancement of wound healing, particularly when delivered through novel systems such as microneedle patches. This section provides a comprehensive overview of the physicochemical, pharmacokinetic, and pharmacodynamic characteristics of lovastatin along with dosage and storage information.
Lovastatin is a competitive inhibitor of the enzyme 3-hydroxy-3-methylglutaryl- coenzyme A (HMG-CoA) reductase, which catalyzes the conversion of HMG-CoA to mevalonate — a key step in cholesterol biosynthesis. Originally developed as a lipid- lowering agent, recent studies have highlighted its broader therapeutic potential, including effects on bone tissue regeneration, fracture healing, and cutaneous inflammation.
Fig. 1- Structure of lovastatin
Physicochemical Properties of Lovastatin
|
Sr. No. |
Property |
Description |
|
1. |
Chemical Name |
[(1S,3R,7S,8S,8aR)-8-[2-[(2R,4R)-4-hydroxy-6- oxooxan-2-yl] ethyl]-3,7-dimethyl-1,2,3,7,8,8a- hexahydronaphthalen-1-yl] (2S)-2-methylbutanoate |
|
2. |
Molecular Formula |
C??H??O? |
|
3. |
CAS Number |
75330-75-5 |
|
4. |
Molecular Weight |
404.5 g/mol |
|
5. |
Melting Point |
174.5°C |
|
6. |
Physical State |
White to off-white crystalline powder |
|
7. |
UV-Vis λmax |
238 nm |
|
8. |
Log P |
4.26 |
Pharmacological Profile Pharmacodynamics
Lovastatin belongs to BCS Class II, characterized by poor solubility and high permeability. It effectively reduces levels of total cholesterol, low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (apoB), non-HDL-C, and triglycerides (TG), while modestly increasing high-density lipoprotein cholesterol (HDL-C). It is commonly used for the treatment and prevention of cardiovascular conditions.
Pharmacokinetics
Lovastatin (branded as Mevacor) is a fungal metabolite derived from Aspergillus terreus. It is a lipophilic prodrug that undergoes first-pass hepatic metabolism. It inhibits cholesterol biosynthesis by competitively blocking HMG-CoA reductase, leading to reduced intracellular cholesterol and increased uptake of LDL-C by the liver. This action helps in lowering cardiovascular risk, especially in patients with Type 2 diabetes and those with a history of cardiac events.
Storage Conditions
Lovastatin should be stored between 5°C and 30°C, preferably in tightly sealed containers. Under these conditions, the tablets remain stable for up to 24 months from the date of manufacture. Optimal storage is at room temperature, between 20°C and 25°C.
Dosage Guidelines
The recommended dosage of lovastatin ranges from 10 to 80 mg/day, typically administered twice daily. The starting dose may be gradually increased in 20 mg increments, with a maximum dose of 80 mg/day.
Polyvinyl Alcohol (PVA)
Polyvinyl alcohol (PVA) is a synthetic, water-soluble polymer derived from the hydrolysis of polyvinyl acetate. Composed of a carbon-based backbone, it is biodegradable under both aerobic and anaerobic conditions. PVA is widely used in industrial, pharmaceutical, and nutraceutical applications due to its film-forming ability, stability, and biocompatibility.
Fig. 2- Structure of polyvinyl alcohol
|
Sr. No. |
Properties |
Description |
|
1. |
Chemical name |
Poly-vinyl alcohol |
|
2. |
Appearance |
White granules or powder |
|
3. |
Solubility |
Soluble in water, slightly soluble in ethanol |
|
4. |
Molecular formula |
[-CH2 CHOH-]n |
|
5. |
Molecular weight |
30,000 gm/mol |
|
6. |
Melting point |
200 °C |
|
7. |
pH |
5.0-7.0 (5% solution) |
|
8. |
Storage |
Store at low 30°C |
Hydroxypropyl Methylcellulose K15M (HPMC K15M)
HPMC K15M (METHOCEL™) is a hydrophilic polymer with high hydroxypropyl substitution, commonly used as a thickening, binding, and suspending agent in formulations requiring thixotropic behavior.
Fig. 3- Structure of HPMC K15M
DRUG CHARACTERIZATION
UV spectrophotometric analysis of lovastatin drug sample
A 50 mg sample of lovastatin was accurately weighed and transferred into a 50 mL volumetric flask. It was dissolved in ethanol to prepare a stock solution with a final concentration of 500 μg/mL, and the volume was made up to the mark with the same solvent. An aliquot of this stock was further diluted to obtain a working solution of 10 μg/mL. The resulting solution was analyzed using a double-beam UV-Visible spectrophotometer (Shimadzu® 1800), and the absorbance spectrum was recorded over the wavelength range of 200–400 nm.
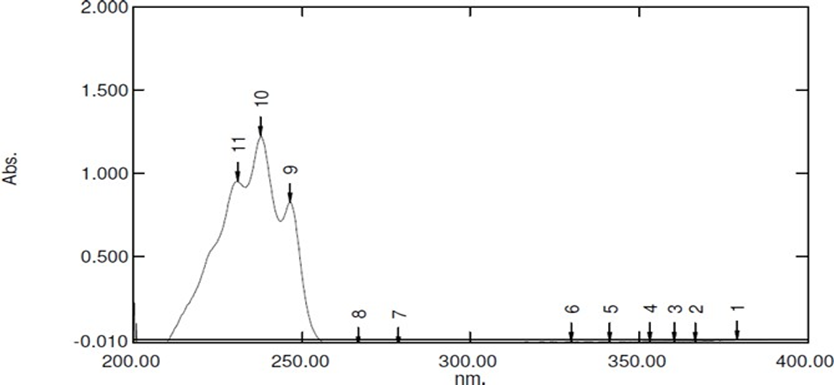
Fig. 4- UV spectra of lovastatin drug sample
Result: The drug sample for lovastatin showed a λ max in ethanol at 238 nm, which is consistent with the value documented in previous studies.
Melting point determination
The open capillary tube method was used to find the medication sample's melting point. The analogue melting point apparatus was used to determine the melting point of a medicine sample powder that had been put into a capillary tube.
Result: The lovastatin medicine sample's melting point was determined to be between 137 - 140 degrees Celsius, which is in line with the value documented in the literature.
DSC study of lovastatin drug sample
DSC analysis of the lovastatin sample was performed using a Perkin Elmer DSC-6000 instrument. Approximately 3 mg of the drug was accurately weighed and sealed in an aluminum pan. The sample was heated from 50 °C to 200 °C at a scanning rate of 10 °C/min under a nitrogen purge at a flow rate of 20 mL/min. An empty, sealed aluminum pan was used as the reference.
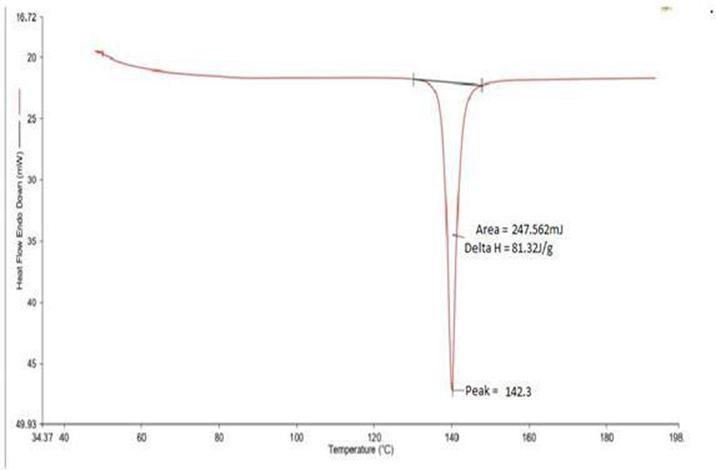
Fig. 5- DSC thermogram of lovastatin drug sample Preparation of Calibration Curve of Lovastatin in Ethanol (238 nm)
A stock solution of lovastatin (100 μg/ml) was prepared by dissolving 10 mg of the drug in ethanol and making up the volume to 100 ml. Serial dilutions were performed to obtain concentrations ranging from 5 to 25 μg/ml. Absorbance was measured at 238 nm using a double-beam UV-visible spectrophotometer (Shimadzu® 1800), and a calibration curve was constructed.
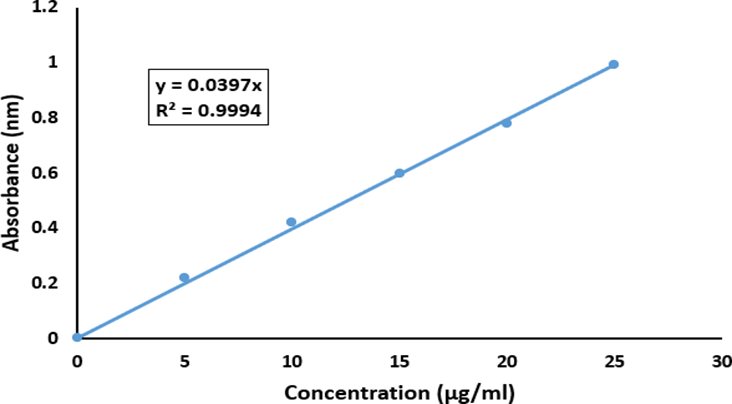
Fig. 6- Calibration curve of lovastatin in ethanol at 238 nm
Preparation of calibration curve of lovastatin in phosphate buffer saline (pH- 7.4) at 238 nm
A 100 ml volumetric flask holding 10 mg of lovastatin was carefully weighed, transferred, and then the lovastatin was dissolved in enough phossphate buffer saline (pH-7.4) to fill the flask to the appropriate level, creating a stock solution containing 100 μg/ml. The produced stock solution was diluted in the range of 5 μg/ml to 25 μg/ml using the same phosphate buffer, and measured at 238 nm on a Shimadzu 1800 UV-visible spectrophotometer.
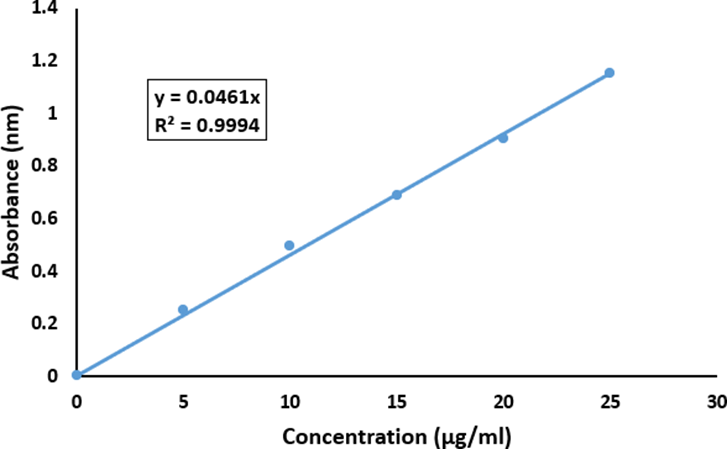
Fig. 7- Calibration curve of lovastatin in 0.1 M phosphate buffer (pH 7.4) at 238nm.
Drug-excipient interaction studies
Lovastatin was mixed with individual excipients in a 1:1 ratio and stored in sealed glass vials under different conditions: ambient (25 °C), refrigerated (2–8 °C), and accelerated (40 °C) for one month. After the storage period, samples were examined for any changes in physical appearance and color to assess compatibility.
Drug Excipient interaction study
|
Sr. No. |
Drug-excipients nature |
Initial appearance |
Storage condition |
|||
|
Refrigerated (2-8°C) and Room temp 25 ?C |
||||||
|
Weeks |
||||||
|
1 |
2 |
3 |
4 |
|||
|
1. |
Lovastatin |
White |
N |
N |
N |
N |
|
2. |
Lovastatin + Polyvinyl alcohol |
Slightly yellow |
N |
N |
N |
N |
|
3. |
Lovastatin+ HPMCK15M |
White |
N |
N |
N |
N |
FORMULATION DEVELOPMENT OF MICRONEEDLE PATCH LOADED WITH LOVASTATIN
Fabrication of microneedle mold
Microneedle molds can be fabricated using various techniques such as photolithography, laser ablation (UV, CO?, IR), 3D printing, ion etching, atomic layer deposition, metal molding, and electro-deposition, using materials like PMMA, PDMS, tungsten, Teflon, ceramics, and photoresists. These methods enable precise surface morphology and dimensional control essential for microneedle formation without producing toxic byproducts.
For this study, master molding and solvent casting were chosen due to their simplicity and minimal equipment requirements. Epoxy resin was used as the casting material, prepared by mixing resin and a curing agent. Lancets were employed to form cavities in the uncured resin, creating a negative microneedle array. The resin was poured into an Eppendorf tube, centrifuged, and leveled with a glass rod for uniformity. A 6×5 array (30 cavities) was created by puncturing the resin with lancets. After curing for 8 hours, the hardened mold served as a template for casting polymeric dissolving microneedles.
Selection of polymers
To create drug-loaded microneedles, the polymers should have the following properties:
Selection of solvent
A suitable solvent is essential for microneedle fabrication to dissolve both the drug and polymer while remaining inert to the mold material. Since both lovastatin and polyvinyl alcohol are water-soluble, and epoxy resin is water-insoluble and chemically inert, water was selected as the solvent for formulation development.
Formulation of tip-loaded microneedle by solvent casting method
Tip-loaded microneedles were fabricated using a two-step casting process. First, a lovastatin solution (200 µg/ml) was prepared, and 50 µl (containing 10 µg of drug) was added to the mold and centrifuged at 5000 rpm for 5 minutes to localize the drug at the needle tips. Subsequently, 400 mg of 30% w/v polyvinyl alcohol (PVA) slurry was added and centrifuged for 15 minutes at the same speed to form the structural base. A total of 15 formulations were developed using PVA (MW 114,000 and 125,000) with varying weights to optimize mechanical strength and drug loading, while keeping the drug concentration constant.
Formulation of different batches of microneedles
|
Batch No. |
Composition of Excipients and drug |
||
|
PVA |
HPMC K15M |
Drug |
|
|
LMP1 |
150 |
10 |
20 |
|
LMP2 |
150 |
15 |
30 |
|
LMP3 |
200 |
20 |
25 |
|
LMP4 |
175 |
30 |
30 |
|
LMP5 |
200 |
25 |
35 |
|
LMP6 |
250 |
10 |
30 |
|
LMP7 |
150 |
15 |
40 |
|
LMP8 |
175 |
20 |
30 |
|
LMP9 |
175 |
20 |
30 |
|
LMP10 |
175 |
20 |
30 |
|
LMP11 |
170 |
30 |
20 |
|
LMP12 |
200 |
10 |
25 |
|
LMP13 |
150 |
20 |
40 |
|
LMP14 |
175 |
15 |
35 |
|
LMP15 |
250 |
25 |
40 |
Drying of microneedles
Microneedles were dried in a vacuum desiccator over a calcium chloride bed, significantly reducing drying time to 8–10 hours, compared to 32 hours at ambient temperature.
Separation of microneedle from mold
Lovastatin-loaded microneedles were carefully separated from the mold using forceps. The removal process was non-destructive and preserved the structural integrity and dimensions of the microneedles.
Application of microneedles patch
The fabricated microneedle patch was applied by placing it on the skin and securing it with surgical dressing tape to maintain contact with the application site.
Evaluation of prepared batches of microneedles
|
Formulation Batch |
Dimensional Analysis |
Strength evaluation |
% Drug release |
|||
|
Needle length (µm) |
Tip diameter (µm) |
Base diameter (µm) |
Total breaking strength (N) |
Breaking strength per needle (N) |
||
|
LMP1 |
500-600 |
20-25 |
150-200 |
1.25 |
0.153 |
89.5% |
|
LMP2 |
200-300 |
30-35 |
250-300 |
1.30 |
0.089 |
92.8% |
|
LMP3 |
300-450 |
40-50 |
150-200 |
1.25 |
0.065 |
90.7% |
|
LMP4 |
270-350 |
25-35 |
200-250 |
1.80 |
0.080 |
88.9% |
|
LMP5 |
250-300 |
20-30 |
250-300 |
2.12 |
0.116 |
93.1% |
|
LMP6 |
350-450 |
30-40 |
150-200 |
1.92 |
0.051 |
88.2% |
|
LMP7 |
400-500 |
40-45 |
70-100 |
2.64 |
0.155 |
92.9% |
|
LMP8 |
400-450 |
35-45 |
80-120 |
1.78 |
0.180 |
97.1% |
|
LMP9 |
200-250 |
35-45 |
80-120 |
1.78 |
0.180 |
97.1% |
|
LMP10 |
200-250 |
35-45 |
80-120 |
1.78 |
0.180 |
97.1% |
|
LMP11 |
400-450 |
25-35 |
100-120 |
2.81 |
0.160 |
94.6% |
|
LMP12 |
250-300 |
30-40 |
50-120 |
1.68 |
0.157 |
96.8% |
|
LMP13 |
400-500 |
35-45 |
100-150 |
1.82 |
0.092 |
95.4% |
|
LMP14 |
350-400 |
40-50 |
120-180 |
2.52 |
0.138 |
96.2% |
|
LMP15 |
200-250 |
20-30 |
150-200 |
1.66 |
0.125 |
92.1% |
Prediction of optimized lovastatin-microneedles patch formulation
The optimized formulation was identified using Design Expert® software based on two critical parameters: maximizing axial fracture force and minimizing cumulative drug permeation. Among 67 predicted solutions, the batch with the highest desirability score (0.872) was selected as the optimal formulation Tables shows that the selected formulation had optimal amounts of composition to formulate microneedles of lovastatin.
Suggested formulation variables of lovastatin-loaded microneedle patch with highest desirability
|
Sr. No. |
Variable |
Quantity |
|
1. |
PVA |
170 |
|
2. |
HPMCK15M |
30 |
|
3. |
Lovastatin |
20 |
Characterization of optimized batch of lovastatin-loaded microneedles
The optimized batch of optimized lovastatin-loaded microneedle patches was assessed and verified using a predicted parameter. Using the projected value from the program, the in-vitro drug release research was evaluated. The cumulative percentage of drugs released was computed, and the resulting graphs
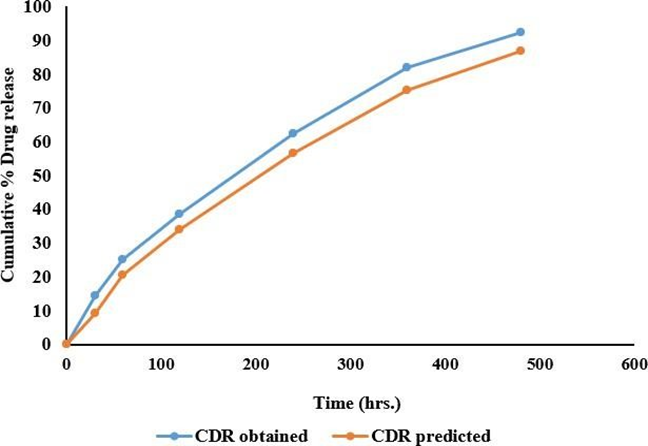
Fig. 8- Predicted vs observed in-vitro release data of optimized microneedle batch of lovastatin
Dimension Analysis using laser confocal microscopy
Dimensional properties of the optimized microneedle batch—height, tip diameter, and base diameter—were evaluated using a Zeiss laser confocal scanning microscope. The system utilized a multiline argon laser source (400–500 nm) for high-resolution imaging and measurement
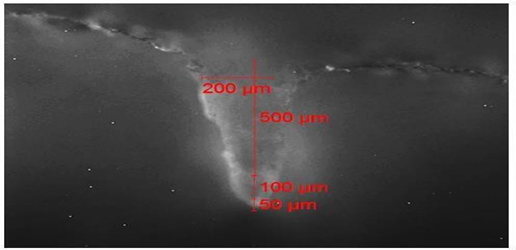
Fig. 9- Laser confocal images of an optimized microneedle patch of lovastatin
Result: The dimensions of the prepared formulations were tested, and it was discovered that the prepared batch of microneedle had the specified dimensional measurements of needle length, tip diameter, and base diameter
Strength (axial needle force) evaluation - The axial force of tip-loaded microneedles was measured using a TA-XT Plus texture analyzer. A 5.5 × 5.5 microneedle patch was affixed to the cylindrical probe using double-sided tape. The test was conducted in compression mode with a trigger force of 0.052 N, a test speed of 0.1 mm/s, and a test distance of 2.5 mm.
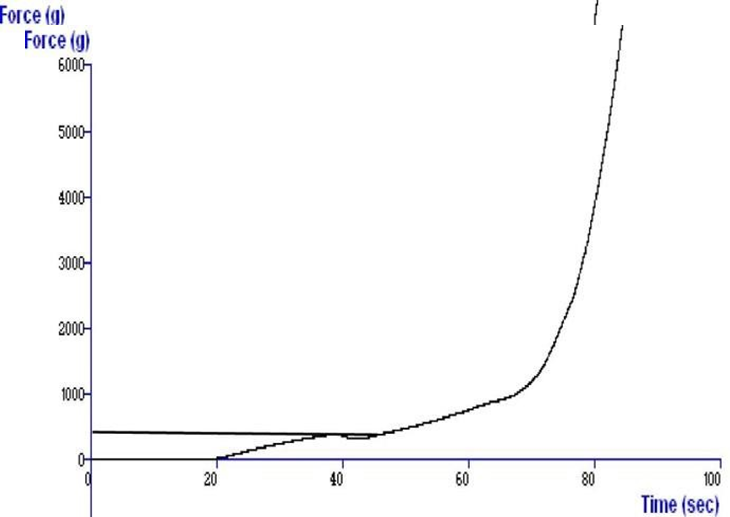
Fig. 10- Graph showing axial needle strength of optimized batch of lovastatin- loaded microneedle patch
Result: The optimized batch's breaking strength (axial needle force) was determined to be 152.8 N (15.30 kg), which is quite close to the target value of 150.45 N.
In-vitro and Ex-vivo Drug Release Studies - The drug release profile of the optimized lovastatin-loaded microneedle patch was evaluated using a Franz diffusion cell with parafilm as the membrane at 32 ± 0.5 °C in phosphate buffer (pH 7.4). The patch was placed with the base facing the donor compartment and the microneedle tips facing the receptor compartment. The receptor medium was stirred at 200 rpm using a magnetic bead. Samples were withdrawn at predetermined intervals and analyzed using a Shimadzu 1800 UV-visible spectrophotometer at 238 nm. A graph was plotted between cumulative drug release (%) and time (min). Ex-vivo permeation was assessed using full-thickness excised pig ear skin mounted on a Franz diffusion cell. Phosphate-buffered saline (pH 7.4) at 37 ± 0.5 °C was used as the receptor medium, stirred at 250 rpm. The microneedle patch was applied over the skin, and samples were withdrawn at specific time points. After each withdrawal, 5 ml of receptor fluid was replaced with fresh buffer. Drug content was analyzed spectrophotometrically at 238 nm. The cumulative drug release was calculated and compared with that of a control drug solution (5 mg in PBS), equivalent to the therapeutic dose. Steady-state flux was determined from the slope of the linear region of the release profile.
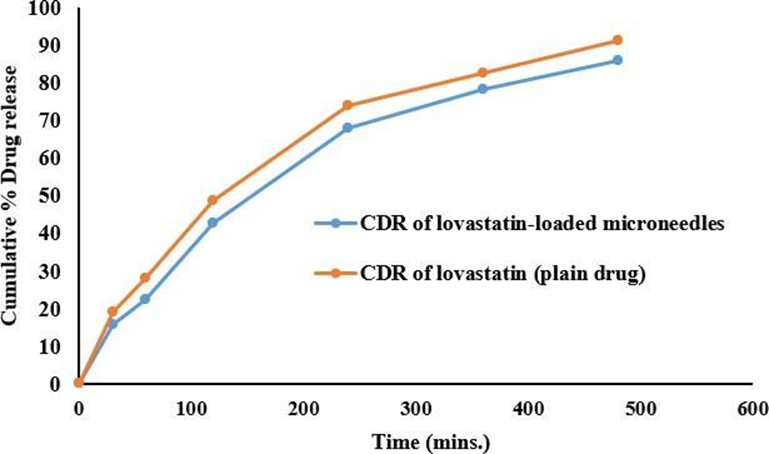
Fig. 11- Comparative ex-vivo release of optimized microneedle patch of lovastatin and lovastatin drug
CONCLUSION
The present study aimed to address the limitations of conventional formulations by developing a tip-loaded lovastatin microneedle patch, with the goals of enhancing drug permeability, reducing side effects, and improving patient compliance.
Characterization of the pure drug was performed using melting point analysis (137– 140 °C), DSC (peak at 142.3 °C), and UV spectrophotometry (λmax at 238 nm), all consistent with literature data, confirming drug purity. Preformulation studies indicated that lovastatin was soluble in methanol, chloroform, PBS (pH 7.4), and water, with a partition coefficient of 4.07. Calibration curves demonstrated good linearity (R² ≈ 1) over the concentration range of 5–25 µg/ml.
Formulation optimization was carried out using a Box-Behnken design through Design Expert® software. Based on axial fracture force, dissolving time, and drug release, 15 batches (LMP1–LMP15) were formulated. The optimized batch, with a desirability of 0.872, comprised PVA (170 mg) and HPMC K15M (30 mg).
Mechanical characterization revealed that the microneedle patch had an overall fracture force of 152.8 N, with higher strength attributed to the use of high molecular eight polymers. Dimensional analysis showed consistent microneedle geometry: height 400–500 µm, tip diameter 50–60 µm, and base diameter 200–250 µm. The drug content of the optimized formulation was found to be 98.25%.
Ex-vivo skin permeation studies using pig ear skin demonstrated that microneedles delivered 86.13% of the loaded drug over 8 hours, significantly outperforming topical drug solutions. These findings highlight the potential of microneedle systems for effective and sustained transdermal delivery of lovastatin in wound treatment.
REFERENCES

Rani Namdev, Rajni Dubey, Dr. Bhaskar Kumar Gupta, Mariya Beg, Lovastatin: A Multifunctional Lipid-Lowering Agent with Emerging Therapeutic Potential in Wound Healing, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1643-1654. https://doi.org/10.5281/zenodo.17120168
 10.5281/zenodo.17120168
10.5281/zenodo.17120168