
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Loknete Dr. J. D. Pawar College of Pharmacy Manur, Kalwan, Nashik
Microbiology might undergo a revolution because to artificial intelligence (AI), which could improve our knowledge and management of microbial system. Explore the revolutionary effects of Artificial intelligence (AI) and machine learning (ML) on the filed of microbiology in this mini-review. The paper gives a quick summary of several fields, including as clinical diagnostic, medication and vaccination development, and management of public health, where Artificial intelligence (AI) is changing practices. Our conversation focuses on the evolution of novel antimicrobial to combat strains that are resistant, the Using neural networks with convolutions for improved Identification of pathogens, and improvements at the point of care diagnostic The use of AI in forensic microbiology, microbial ecology, and epidemiology is also described, highlighting its ability to interpret intricate microbiological interaction and predicting disease epidemics. Highlight the need for interpretable artificial intelligence (AI) models that adhere to ethical and medical standards while critically examining the difficulties in applying AI, like as guaranteeing quality of the data and getting over algorithm-based limitation. We discuss the complexities of digitalizing microbiology diagnosis, highlighting the necessity of effective data management in clinical and laboratory setting. We outlined important future possibilities for artificial intelligence in microbiology, with an emphasis on creating flexible, self-updating AI models and integrating them into clinical setting. AI has the potential to transform infection control and microbiology diagnosis, greatly impacting patient care and public health.
Microbiology, the study of microorganisms such bacterial, viruses, fungi and parasites, has long been important in understanding diseases, environmental processes, and biotechnological applications [1]. The launch of artificial AI is a type of intelligence. breakthrough phase in the always evolving filed of microbes, altering the foundation of its application and study. As we enter this era, a change in perspective toward computational methodologies for meaningful interpretation of data is required due to the unprecedented influx of biological data obtained from high-throughput technologies. Form identifying microbial interactions and resistance mechanism to forecasting pharmacological targets and infectious disease diagnosis , artificial intelligence (AI), and in particular machine learning (ML), emerges as a crucial tool in tackling complicated microbiological difficulties [2]. (AI) is being incorporated into a variety of fields within microbiology, including bacteriology, mycology, parasitology, and virology. The effective use of AI in microbiology has been accelerated by its combination with sophisticated data gathering tools increased processing strength, and globally network, which are exemplified by Moore's law, the internet, and big data [2,3]. This combination is especially apparent in the files of drug design, where AI-powered techniques are leading the manner in The production of new antimicrobials
artificial intelligence (AI) has an equally transformative role In the field of clinical microbiology, improving accuracy of diagnosis and streamlining data processing. AI-enabled methods such as matrix-assisted laser ionization/desorption duration - flight MALDI-TOF mass spectrometry is transforming antibiotic opposition profiling as well as microbiological identification by offering prompt, accurate, efficient and reasonably priced fixes [5,6]. AI’s ability to process vast datasets—like genomic information and digital images generated through modern diagnostic tools— is essential to enhancing laboratory findings and speeding up diagnostic workflows. [7,8]. Ai in Microbiology can be used to health with health of the public issue including sepsis and infection disease management, where it can help with diagnosis prognosis, and individualized treatment plans. AI’s use in infection avoidance and management is also Notable because of its capacity to evaluate massive health datasets, which helps with infection control plans and epidemic identification [1,9]. Our goal in this study its to examine the various facets of artificial intelligence’s function in medical microbiology, with a focus on how it affects both clinical and research applications. We will talk about how AI is substantially advancing health care and public health by not just that changing current methods, but furthermore opening the door for new findings and advancements inside the filed of microbiology Consequently making a substantial contribution to the development of healthcare and public health. This investigation into the intersection of AI and microbiology will shed light on the cutting edge, difficulties, and the future of this multidisciplinary partnership.
1.1 Fundamentals of AI in microbiology
1.1.1 Machine learning (ML)
Microbiology is changing as a result of machine learning, a key element of artificial intelligence (AI). From microbial identification to antibiotic resistance prediction, this technology provides reliable techniques for data analysis. Making use of a dataset of more than The support vector machine (SVM) and 1500 genomes technique has been utilized to find both well-known and new Genes in Mycobacterium tuberculosis that resist antibiotics [10]. Figure 1 provides a schematic representation of machine learning applications in microbiology.
1.1.2 Basics of machine learning
Computers may get knowledge from data and make judgments on their own thanks to machine learning. In microbiology, this is especially advantageous since it opens up new avenues for microbial investigation and greatly improves our comprehension of microbial behavior and disease outcomes [10].
1.1.3 Supervised learning.
Using labelled datasets to train algorithms is known as supervised learning. This approach works well in microbiology for objectives like forecasting the behaviour of microorganisms or the course of diseases. To detect antibiotic resistance in different bacterial species, adaptive boosting classifiers are created [11,12].

Figure 1. General Workflow And Example For Machine Learning Applications In Microbiology.
1.1.4 Unsupervised learning.
Analyse unlabelled data to find hidden patterns in intricate microbial is known as unsupervised learning. datasets Our comprehension of various microbial communities and their interactions can be greatly improved by using this technique [13–17]. The original dataset is symbolized by the specimens on a pink background. A wide range of molecular characteristics, including DNA, RNA, and proteins, as well as phenotypic characteristics, such as cellular shape, motility, and acidity levels, are noted from every specimen. These characteristics, represented by F1 through make up a comprehensive collection of traits. The machine learning model will try to predict certain goal outcomes that are identified concurrently with feature gathering. These targets, which have a blue backdrop and are connected to the features by bidirectional black arrows, are created from extra data that is correlated with the specimen. The training stage, which follows, is characterized through a violet colour and entails analysing the input data, which comprises parameters such gene activity patterns, metabolic product quantification, and the relative abundance of microbial communities. This crucial stage involves a number of systematic actions, including choosing a suitable model for machine learning, adjusting its conditions to improve precision, and creating the finished model as it identifying most important characteristics. Following During training, the model is ready for the forecast. stage, during which it comes into contact with fresh, unlabelled biological samples that have been identified by a yellow backdrop. The same features that were utilized in the training phase are extracted from these data through processing. Lastly, the model predicts the unknown goal outcomes—which are still marked as question marks—by applying its learnt patterns to these features. This predictive ability advances our knowledge of microbial interactions and behaviour by allowing the extrapolation of important findings from new biological data. Microbiological research and public health both heavily rely on microbial behaviour or disease transmission [18, 19].
1.1.5 The role of deep learning.
Neural networks are used in deep learning, an advanced subfield of machine learning, to analyse large datasets. Models for deep learning such as ARGs (deep antibiotic resistance genes) [18], which are utilized in microbiology to predict antibiotic resistance genes, which helps with environmental monitoring [30].
1.1.6 ML in Microbial data analysis and Predictive Modelling.
Significant quantities of microbiological Data processing is possible. and analyse a machine learning. Its application to predictive modelling, specifically for predicting patterns microbial behaviour or the transmission of illness, is essential to microbiological research and public health. [18,22].
1.1.7 Challenges in ML for microbiology.
There are difficulties when using machine learning in microbiology, especially when it comes to The amount and calibers of information. Large, varied Datasets are necessary for reliable instruction and prediction of effective machine learning models [11]. Predictive machine learning models can also have certain disadvantages. For example, because training data may contain bias that influences outcomes, it may be challenging to identify and minimize bise in AI models used for microbiological applications, Inadequately structure detraining data may contain bias that influences outcomes, it may be challenging to identify and minimize bias in AI models used for microbiological applications. Inadequately structured datasets for training machine learning models and the availability of low quality microbiological data [23]. with data management arise form the digitization of microbial diagnostic processes and include collecting, guaranteeing quality, storing, and safeguarding data. Future developments in AI and ML in microbiology will likely include more in-depth conversation and potentially new regulations pertaining to patient authorization, data protection, and ethical concerns. [24]. Furthermore, laws and regulations are lagging behind scientific advancements in area like genome editing and synthetic biology, which poses risks and uncertainties. in addition to the few case studies, several among these technologies require an external data source in order to validate their specific algorithms in a medical scenario [25].
2. CURRENT DEVELOPMENTS AND APPLICATIONS OF AI IN MICROBIOLOGY.
2.1 Developments in Clinical Diagnosis and Illness Identification.
A revolution in medical microbiology is being brought about by artificial machine learning (ML) and artificial intelligence (AI), which offer quick and accurate diagnosis as well as treatments For contagious diseases. Machine learning (ML), for example approaches similar to convolutional neural network (CNNs) significantly increase the accuracy of computer-aided diagnostics (CADX) software. Identifying cells afflicted by malaria [26,27]. Similar techniques have improved the sensitivity of parasite detection in samples, outperforming convention human slide testing [28]. The capability of automated tools to analyses laboratory examples that are shows as images has transformed the identification of species and genera of bacteria. These technologies, they are crucial in a number of industries, including the food, veterinary, and medical sectors, identify bacterial based on their form, colour, and colony patterns [29,30].
2.2.1 Epidemiology and disease prognosis.
In epidemiology, machine learning (ML) models such as logistic regression (LR) as well as artificial ANNs, or neural networks, are utilized to forecast patient results for illnesses like Ebola is a viral illness. Instruments such as the Ebola Care app analyse test data and clinical symptoms to give medical professionals vital information for treatment decisions. [31]
2.2.2 Point-of-care (POC) diagnostics.
ML has a revolutionary effect on point-of-care (POC) diagnostics. ML algorithms use routine test findings, such urine, to distinguish between positive and negative instances for diagnosing sexually transmitted illnesses like trichomoniasis [32]. This method works very well in environments with limited resources. Additionally, the creation of mobile microbiological laboratories has been made possible by advancements in smartphone technology, increasing accessibility to diagnoses. [33,35] Artificial intelligence (AI)-enabled diagnostic tools are being created more frequently In order to be utilized in the hospital, offering prompt outcomes that guide therapy choices without requiring a lot of laboratory processing. These gadgets are especially useful in places with limited access to centralized lab facilities, including isolated or resource-constrained locations. For instance, at the bedside or in the field, AI-powered devices can do quick diagnostic tests for infectious diseases like COVID-19, TB, or malaria. Healthcare professionals can start therapy right away because to these gadgets' ability to test samples, such blood or sputum, and offer precise results in a matter of minutes. By delivering top-notch ability to diagnose straight to patients, eliminating the need of referrals to specialist laboratories, and enhancing Gaining access to prompt Take care, AI-powered Diagnostics at the point of care have the ability to revolutionize the way medical care is delivered. [36]
2.2.3 Drug and vaccine discovery.
Finding novel chemicals and potential vaccines is made much easier with machine learning. Its ability to speed up drug discovery has been demonstrated by its usage to examine data from open databases such as the Opportunistic Infection and Tuberculosis Therapeutics Database (Chem DB) for possible antiviral compounds against the human immunodeficiency virus (HIV) [37,38]. For Apicomplexan pathogens, silico vaccine candidate selection with ML classifiers has shown promise [39,41].
2.2.4 Antimicrobial resistance and outbreak prediction.
In order to comprehend and address antimicrobial resistance (AMR), ML, or machine learning is essential. This has been crucial detecting medication resistance in diseases like HIV and tuberculosis (TB), creating new opportunity for managing and predicting resistance [42,48]. Furthermore, ML has demonstrated its potential in real-time infection disease tracking by being used to forecast disease outbreak utilizing data form unconventional sources like social media and search engines [49,52].
2.2.5 Microbial ecology and forensics.
ML is used in microbial ecology to help comprehend the dynamics and interaction of microbial population. Ecosystem interaction have been predicted using methods such as random forest (RF) [53,54]. ML helps forensic microbiology analyse post-mortem microbiomes, which greatly advance both public health diagnostic and forensic science [51]
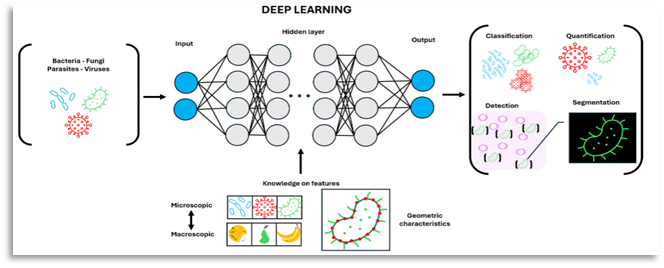
Figure 2 is a schematic picture that shows how deep learning algorithms are used to analyse microscopic photographs of microorganisms, with an emphasis on evaluating their geometric qualities and macroscopic similarities.
2.2.6 improving medical microbiology's efficiency and accuracy.
The contribution of AI to improving accuracy and productivity in medical microbiology is significant. Automatic susceptibility examinations and the pathogen identification simplify lab procedures while tackling the difficulties associated with manual processing of intricate data, such as pictures, spectra, and DNA-RNA sequences, particularly when staff members are present. shortage and complex analyses [55,56].
Applications of AI in microbiology are many and include:
3. AI IN HEALTHCARE AND MICROBIAL DIAGNOSIS.
Through Natural language processing (NLP), deep learning, and machine learning (ML), artificial intelligence (AI) plays a varied role in healthcare, including microbial diagnosis. It works especially well for onco-radiology and structure data processing form hospital labs [68]. NLP makes it easier to create and maintain electronic medical records (EMRs) and allows for the analysis of voice and text diagnose a variety of illnesses [69].Creating sophisticated algorithms for culture identification and improving the effectiveness of microbial culture analysis are two example of AI used in culture interpretation [70,71]. Methicillin-resistant staphylococcus aures (MRSA) identification and sophisticated culture analysis in urine samples are made possible by automated methods such as the independence and PhenoMatrix automated plate assessment system (APAS) [72,73]. Helps identify and treat drug-resistant infections early forecasting patterns of antimicrobial susceptibility [74]. AI’s incorporation into extensive laboratory operations is exemplified by solutions for complete laboratory automation, such as WASP Lab and Kiestra Total Laboratory Automation (TLA) [75].
3.3.1 Sepsis management.
models in which anticipate the start of sepsis in advance, outperforming traditional scoring techniques, demonstrate AI's critical role in sepsis early warning systems [76]. Regular clinical factors have been added to these models, enhancing the viability of predicting sepsis in a variety of contexts [77,80]. By using machine learning and big data- based on screening techniques that incorporate unstructured textual data for greater accuracy, AI has also improved the detection of sepsis [81,82]. Clinical research links early warning systems to lower mortality and shorter hospital stays, confirming AI's efficacy in managing sepsis [83]. AI also helps in subtyping sepsis by classifying several phenotypes with various clinical traits [84]. AI systems swiftly identify typical bacteria and fungi in pathogen identification and antimicrobial susceptibility testing, improving empirical antibiotic therapy [85]. With prediction models for urine production upon resuscitation and fluid reactivity, artificial intelligence (AI) models direct fluid resuscitation and management in the treatment of sepsis [86,87]. Frameworks for causal inference calculate the effects of treatments, enabling more individualized healthcare [88]. In the prediction of sepsis, AI models have dramatically decreased hospital stays and increased in-hospital death rates [89,90]. To validate these models and incorporate them into clinical practice, more study is necessary [91].
3.3.2 Advancing infection surveillance and control.
AI is enhancing the prevention and management of infections (IPC) By altering the monitoring of healthcare-associated infections (HAIs). Its use in deciphering intricate datasets from electronic health records (EHRs) is essential for tracking infection patterns and assessing intervention tactics [92]. The application of deep learning to chest radiography for tuberculosis diagnosis exemplifies AI's role in identifying infections with implications for IPC [93]. In laboratories, improved microscopy and machine learning algorithms are used for targeted antimicrobial treatment and quick diagnosis [94,95] Even with AI’s revolutionary potential, finding high-quality datasets for model building continues to be difficult [96]. However, AI promises to have a significant effect on patient treatment plans as well as public health management, well as increase the effectiveness of infection surveillance.
3.3.3 AI in antibiotic discovery against MRSA.
The development of novel antibiotic to combat MRSA has been greatly aided by AI and ML applications in microbiology [97]. The identification of possible antibiotic candidates has hastened due to AI’s capacity to process and analyse large data sets (figure-3) using features calculated by RDKIT [98,99]. The study technique entails training, validating, and evaluating ML models. Performance is assessed using AUPRC [99]. AI's capacity to analyse and show the chemical space of a molecule, which aids in differentiating between antibiotic that are effective and those that are not [100,101] certain structural classes that show how antibiotics work are identified Using algorithms for deep learning and monte and searches [102,103]. The synergy between computational predications and conventional experimental approaches is highlighted by the rigorous experimental confirmation of AI-driven forecast. AI-guided research sheds light on the pharmacological characteristics, resistance mechanisms, and general effectiveness of the substance [104,109].

(Figure 3) Large databases are used in computer-aided drug design to sort through and find important pharmacological characteristics that affect a compound's functioning and effectiveness.
Regardless of the methods utilized, the collected data constitute the cornerstone for designing a suite of new chemicals. These new substances are put through a thorough testing process, and the findings give new information about their pharmacological characteristics. The compounds are refined through a series of steps in this recurrent cycle until a reliable scoring system produces potential antibiotic medicines. Following optimization, these candidates are critically assessed to look at their safety and effectiveness characteristics in vivo. then put through a rigorous assessment that looks at their safety and effectiveness characteristics in vivo.
4. ISSUES, DEVELOPMENTS, AND PATHS FOR MICROBIOLOGICAL APPLICATIONS OF AI AND ML.
A new era in prevention and management of infections (IPC) and diagnostic capacities is ushered in by the application of AI and ML in microbiology. Nevertheless, in order to fully utilize their potential, these limits and difficulties must be resolved.
4.4.1 Data quality and algorithm challenges.
The effectiveness of training data determines how well ML algorithms work in microbiology. Due to data sources' frequent imperfections and potential for noise introduction, obtaining high-quality data is a constant struggle. It is anticipated that sophisticated data cleaning and normalization methods will lessen problems associated with noisy and imbalanced data. Future developments will probably concentrate on creating strategies to raise the effectiveness of training information and increase the algorithms' capacity to be generalized. Furthermore, XAI, or explainable AI initiatives seek To develop additional visible and interpretable models of in order to increase user trust [110].
4.4.2 AI in IPC: Challenges and Prospective Evaluation.
AI has several benefits for IPC, including the ability to handle big datasets and produce reliable results. However, there are issues with AI's reliance on high-quality data and the lack of strong reference standards in IPC. In order to guarantee clinical relevance and sensitivity to the subtleties of healthcare data, future directions include carrying out more prospective investigations in clinical settings and establishing strong frameworks for collaboration between AI developers and IPC specialists [111,113].
4.4.3 AI models' clinical integration and universal application.
A hurdle is The restricted adoption of Medical AI experts because of Its intricate reasoning and incompatibility with traditional medical logic. The upcoming trends include creating AI simulations that can oneself -update along with adjust to various medical care settings, increasing their applicability and efficiency. Through education and alignment with medical thinking, efforts will be made to increase healthcare professionals' adoption of AI [114,120].
4.4.4 Digitalization in diagnostic processes.
The digitization of microbiology diagnostic procedures presents data management issues with regard to security, storage, quality assurance, and collection. With a growing emphasis on handling the deluge of data using cutting-edge analytics tools and complex data visualization strategies, the trend toward digitalization will continue. Another important trend is the training of laboratory staff in digital skills for efficient management and analysis of this data [121,128].
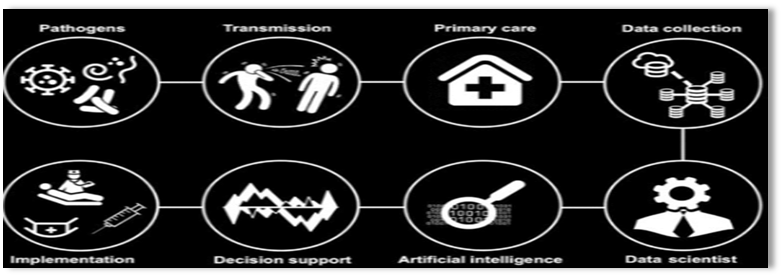
Figure 4: Management of infectious illnesses and AI.
4.4.5 Legal and ethical considerations.
Microbiology data must be collected, analysed, and shared in accordance Considering legal and regulatory regulations, such as Europe's General Data Protection Regulation, or GDPR. More in-depth conversations and possibly new laws pertaining to patient consent, ethical issues, and data protection With relation to AI and ML in microbiology will be discussed in the future. It is crucial to define universal standards for data exchange and usage, informed by ideas like FAIR, and to harmonize legal frameworks [129,132].
4.4.6 uses of machine learning in microbiological labs.
In microbiology labs, Machine learning is able to greatly improve The diagnostic procedure. Algorithm integration across From pre-analytics to post-analytics, the diagnostic procedure will be the main focus of future developments in machine learning applications. The focus will be on developing algorithms capable of deciphering intricate interactions within bacterial networks and offering subtle insights on pathogenicity and microbial resistance [133,140].
4.4.7 Artificial neural network (ANN) and Deep learning (DL).
The algorithmic system known as artificial neural networks (ANN) functions similarly to organic neurons. It consists of an output-generating function (similar to an axon), an activation function applied to the sum of weighted input vectors (similar to a cell body), and an input vector of numerical values multiplied by weights (similar to dendrites in a neuron). Multiple hidden layers are added to the neural network model in order to handle a complex problem [141]. Growing or lowering how many nodes there are in the intermediate levels (also known as concealed layers) may increase or decrease the data size. Therefore, huge data can be subjected to classification analysis. The use of a multi-layered neural network modelling technique is known as deep learning (DL). When gathering and disseminating data, there are crucial factors to take into account; Data developers are required to make sure patients are informed and that their consent is acquired. consider the numerous national and international regulations that safeguard the confidentiality of medical records [142].
5. INFECTION DISEASE DIAGNOSIS AND DISEASE PREVENTION.
Clinicians use artificial intelligence to help them make clinical decisions. It is possible to predict Using data, determine which hematological patients with febrile neutropenia will develop infections caused by multidrug-resistant Gram-negative bacteria (MDR-GNB). gathered from electronic health records (EHRs). EHR benefits include quicker access to test findings and medical care, as well as central storage of all patient data. Numerous factors, including the patient's microbiota state, hospital environment, and history of antibiotic treatment, are linked to the likelihood of acquiring a multidrug-resistant infection (143). Artificial AI initiatives for infectious illness early detection.
Figure 5. AI and infectious diseases management.
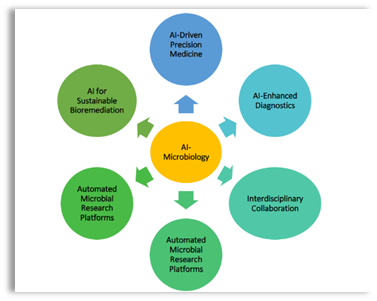
Figure.6 Potential future advancements of AI in Microbiology
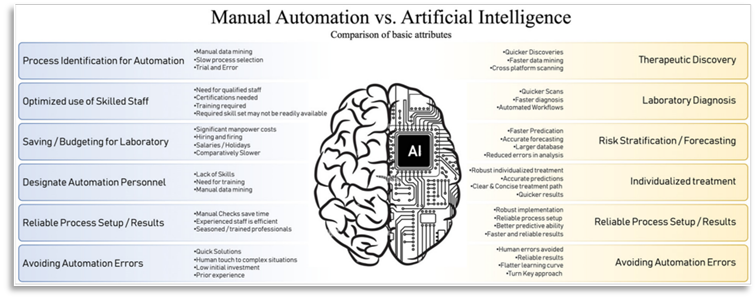
Figure 7. Guide Artificial Intelligence (AI) against Automation: Although automation increases productivity, it necessitates modifications to the laboratory's infrastructure and a change in the requirements for employee training.
New diagnostic and prognostic models will be created by applying AI to huge clinical datasets produced by increased automation. The move to individualized medicine will be made possible by automation and artificial intelligence.
6. Digital Microbiology
As Topol said in 2019, the arrival of digitalization and AI has raised expectation in the healthcare business [141]. Theses expectations are mostly driven by the increased focus on cost reduction and quality optimization. But it’s important to understand that the full advantages of digitization will only be achieved by significantly improving healthcare procedure, especially with regard to quality improvement. As highlighted by Dolen et al. in 2017 this cells for an increased need for high quality digital laboratory data, including microbiological information in diagnoses [142].
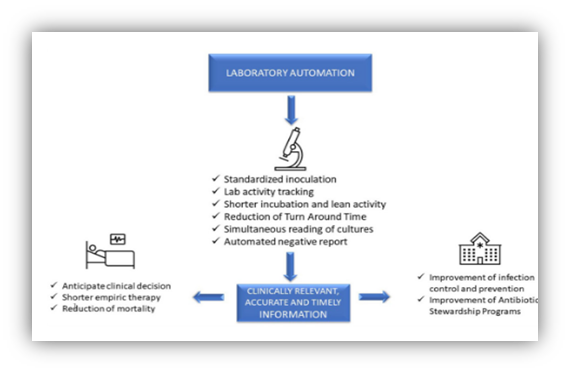
Figure: 9. Mencacci A, De Socio GV, Pirelli E, Bondi P, Cenci E. Laboratory automation, informatics, and artificial intelligence: present and future views in clinical microbiology. Effects of automation on laboratory, patient, and hospital administration. Microbiol Front Cell Infection. PMID: 37441239; PMCID: PMC10333692. doi: 10.3389/fcimb.2023.1188684. 2023 Jun 27;13:1188684
7. Artificial intelligence, informatics, and laboratory automation
The automation of the complete diagnostic process, including agar plate inoculation, incubation, reading of culture findings, identification (ID), and antimicrobial susceptibility testing (AST), is referred to as "Total Laboratory Automation" (TLA) in clinical microbiology. In a conventional laboratory, each of these procedures is typically carried out by hand using a sample-centric methodology. There are currently Two methods for laboratory automation (LA) on the market: Copan Diagnostics' WASPLAB system Murrieta, CA as well as the BD KiestraTM Becton Dickinson's system Sparks, MD) [143].
CONCLUSION
A revolutionary change in biomedical research and clinical practice is represented by the incorporation of AI and ML in microbiology. Numerous uses for these technologies have been revealed by this investigation, ranging from improving clinical microbiology diagnostic accuracy to leading the way in drug discovery and improving public health management. Significant progress has been made in pathogen identification, antibiotic resistance prediction, and infectious disease management thanks to AI's capacity to process and evaluate complicated biological data. Notwithstanding these developments, issues including algorithmic constraints, data quality, and ethical considerations continue to be significant. AI models that are flexible, interpretable, and can be easily incorporated into clinical settings are desperately needed in order to match computing power with medical knowledge and moral principles. Imagine a time in the future when microbiological research and practice are heavily reliant on AI and ML. It is essential to construct self-updating, flexible AI models that can operate in a variety of medical environments. Furthermore, healthcare workers will need greater education and training in AI-based technologies to include AI into medical procedures. To sum up, ML and AI have the power to completely microbiology and present previously unheard-of chances to enhance public health and patient care results. For AI and ML to dramatically improve healthcare and usher in a new era of precision medicine in microbiology, it is imperative that present issues be addressed and future advancements be prioritized.
REFERENCES



Siddhi Gangurde, Poonam Gangurde, Yashpal More, Microbiology in The Era of Artificial Intelligence Transforming Pharmaceutical Microbiology, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2660-2682. https://doi.org/10.5281/zenodo.17441860
 10.5281/zenodo.17441860
10.5281/zenodo.17441860