
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, D.Y. Patil College of Pharmacy, Kadamwadi, Kolhapur, Maharashtra, India.
Superficial skin infections caused by fungi are common across the world and involve the stratum corneum or the outer skin layer which is rich in keratin and provides a favorable environment for fungal growth. Topical drug delivery is the preferred approach for managing such infections. However, conventional topical dosage forms, including creams and gel generally have drawbacks such as poor solubility of lipophilic antifungal agents, limited penetration across the skin barrier and low therapeutic performance. In recent years, microemulsion-based gel formulations have gained attention as an advanced strategy for topical antifungal delivery due to their ability to overcome these limitations. Microemulsions exhibit isotropic properties and thermodynamic stability consisting of oil, water, surfactants, and co-surfactants. These systems facilitate improved drug solubilization, enhance penetration through the stratum corneum and promote long-term retention of the drug at the site of infection. This review presents a detailed discussion of the formulation aspects, structural features and mechanisms of action of topical antifungal microemulsions, with special focus on azole-based drugs. Various methods employed in their preparation, such as phase titration and phase inversion techniques, are described, along with the importance of pseudo-ternary phase diagrams in optimizing formulation composition. In addition, previously published studies on microemulsion-based antifungal gels are also reviewed to emphasize their therapeutic effectiveness. Overall, microemulsion-loaded topical gels offer a flexible and efficient delivery platform, demonstrating enhanced clinical performance and considerable potential for future pharmaceutical development
Fungal skin infections are generally caused by fungi that grow on or inside the body. They are very common and usually thrive in warm, moist areas of the skin. Fungal skin infections usually affect the skin as the Stratum corneum (outer-most skin layer) is keratin-rich. Keratin is a tough, fibrous structural protein found in skin, hair, and nails and it is a nutrient-rich surface for fungi. The common symptoms of a fungal skin infection include itching, redness, inflammation, scaling or flaking skin, burning or stinging sensations, dry or cracked skin and it might get worse with sweat and heat[1]. One major target place for medication application is human skin. Topical medication distribution is a suitable approach to limit the therapeutic effect on the affected area and minimize systemic incrimination, particularly when treating local disorders[2]. A prevalent fungal illness affects over two-thirds of the world's population[3]. Topical medications are a significant class of drug delivery systems and their application in treatment is expanding. Topical dose forms are used to comfortably administer medications to specific areas of injured or sick skin[4]. Because topical medications penetrate the underlying layers of skin or mucosal membranes, they have local effects at the application site. The main advantage of topical delivery systems is their ability to target medications directly to a specific area (local action). This enables the use of drugs with a narrow therapeutic range and a short biological half-life to achieve a prolonged effect.[1]. Microemulsions are gaining a lot of attention in topical drug delivery methods because of these characteristics. Various formulation experiments show how microemulsions can be used to deliver antifungal medications[5]. Due to its capacity to improve solubility, penetration, and drug retention in the skin, different evaluations further demonstrate the efficacy of microemulsions as versatile carriers for both synthetic antifungals and herbal actives[6]. When it comes to topical drug delivery, microemulsions are superior to conventional creams, gels, and solutions[1]. They are transparent, isotropic, thermodynamically stable formulations of water and oil that are stabilized by using an interfacial coating of surfactants that have been appropriately mixed with a cosurfactant[7]. One problem with applying gels or liquids on the skin to fight fungus is they often struggle to break down fat-like medicines. Surprisingly, using microemulsions helps more of the drug get absorbed. What stands out is how these mixtures soak deeper into the outer layer of skin compared to traditional creams. That stronger wetting raises chances the active agent moves effectively across barriers, speeding its delivery[1]. In order to increase its dissolving effectiveness in both oil-loving and water-loving If we create a stable emulsion, the drug permeability will increase. Conversely, microemulsion’s low viscosity decreases pain compliance and makes it very difficult to apply to the skin. Microemulsions or microemulsion based gels develop quickly when compared to solutions, gels, or formulations. Because natural polymers are easily accessible, they are inexpensive in distribution systems. Additionally, they are micro-porous, environmentally friendly, and readily approved by regulatory agencies[3]. Pseudo-ternary phase diagrams, which allow the identification of the most appropriate components and their ideal relative proportions for producing physically stable systems, are typically used in the development of ME formulations. An alternate method to more successfully identify the appropriate region of ME formulations is offered by techniques for the design and analysis of combined experiments. These techniques also allow for the identification of the best formulation within the indicated region of possible formulations[6]. Microemulsions' pharmacological applications have been widely studied as possible drug delivery systems for drugs that are poorly soluble in water. With a number of benefits such as ease of formation, spontaneous production and scaling up these systems improves thermodynamic stability. That means the microemulsion does not fall apart easily. It also helps with drug solubilization and bioavailability, which is huge because drugs that dissolve better get absorbed better by the body. They are frequently utilized as drug carrier systems for topical medication delivery. By lowering the volume of the drug delivery vehicle and significantly increasing the therapeutic efficiency of medications, microemulsions minimize harmful side effects. The cell membrane plays a big role as it can solubilize lipophilic (fat-loving) components, which makes it easier for lipophilic drugs to get absorbed[8].
1.1 Historical Background
In the middle of the 1930s, a patent was granted for the use of a third component (surfactant) to combine water and oil into a single-phase or homogeneous or only one phase system[9]. But the first scholarly research wasn't done until 1943[10]. Hoar and Schulman demonstrated that spontaneous emulsification can be induced with the use of a potent surface active chemical. Due to the extremely low interfacial tensions that the surfactants encourage, this is currently explained by the creation of microemulsions. Winsor recognized four forms of phase equilibrium after studying the phase patterns of water, oil, surfactant combinations in the presence of various additives five years later[11].
Type I / Winsor I: Surfactant-poor oil phase and surfactant-rich or surfactant-efficient water phase (lower phase) exist.
Type II or Winsor II: There is a surfactant-dense oil phase (the upper phase) and a surfactant-deficient water phase.
Type III / Winsor III: Water (lower) and oil (upper) surfactant-poor phases interact with a surfactant-rich middle phase.
Type IV: Homogeneous mixture in a single phase.
A transparent solution known as a "microemulsion" was developed in 1959 when scholars like Schulman et al. formulated a multiphase system made up of water, oil, and surfactant with alcohol. Early on, some researchers referred to these systems as "swollen micelles", while others used the term "micellar emulsion". However, the term "microemulsion" is now widely approved[11].
1.2 Theory behind Microemulsion
According to Schulman and colleagues, anisotropic viscoelastic birefringent systems are made up of an array of cylinders when the systems are homogeneous, and fluid oil drops, clear and symmetrical, without visible chirality made up of uniform spherical droplets of either water or oil in the proper continuous phase. The interface is constantly and spontaneously changing in these dynamic systems [10]. Skin acts as a natural barrier for topical drug administration, making it challenging. Considering this, significant amount of drug gets loaded into microemulsions, minimal skin irritation, and the potential to lower the outer layer of skin or stratum corneum's diffusion barrier by dissolving the lipids present and improving drug penetration[12]. First, the formulation's high drug content increases the thermodynamics toward the skin. Second, the drug's enhanced thermodynamic activity might encourage its absorption into the skin. Third, by acting as permeation enhancers, the components of the microemulsion may lower the stratum corneum's diffusional barrier and speed up the drug's skin penetration. Additionally, the ability of formulations to permeate may be affected by the hydration effect of microemulsion on the stratum corneum[13]. Microemulsions are formed, shaped by forces or theories that hold them together or push them apart i.e., their stability and phase behavior. Their behavior shifts because hidden rules change under pressure [14].
These theories are
1. 2.1 Thermodynamic theory
The free energy of forming a microemulsion depends on amount of the surfactant that lowers the surface tension between oil and water and the change in entropy of the system. The formula is,
Gf = γ a - T S
Where,
Gf = free energy of formation
A = change in interfacial area of the microemulsion
S = change in entropy of the system
T = temperature
γ = surface tension at the oil-water interface
When a microemulsion forms, the interfacial area (A) changes a lot as we get tons of tiny droplets. Normally, A is positive, but it is really small here. The entropy (S) is all about disorder. The system’s entropy increases because one phase is mixed into another as many small droplets. This large increase in entropy offsets the positive A value. other processes like surfactant molecules moving around and swapping between monomers and micelles add to the entropy. Therefore, for a microemulsion to form spontaneously, the free energy of formation (Gf) has to be negative. That happens when surface tension drops a lot and entropy increases significantly. When that balance happens, the microemulsion forms quickly and stays stable over time. Understanding this helps explain why microemulsions are so useful in drug delivery as they keep the drug dissolved and stable, making absorption easier[15].
1.2.2 Solubilisation theory: When microemulsions form, oil and water phases mix through micelles or reverse micelles. These micelles slowly get bigger and swell until they reach a certain size range[14].
1.2.3 Interfacial Theory
A blend of film theory where low surface tension plays a key role underpins this view. Microemulsions form quickly because surfactants and co-surfactants team up, creating an urge to spread and reduce edge tension. The film at the interface, made up of surfactant and co-surfactant molecules, acts like a liquid “two-dimensional” third phase. It is in equilibrium with both oil and water. This film can be a duplex film, meaning it has different properties on the water side compared to the oil side.
According to the duplex film theory, the interfacial tension γT is given by,
γ T = γ (O/W) --- π
Where,
γ (O/W) a = Interfacial Tension (reduced by the presence of the alcohol).
γ (O/W) a is significantly lower than γ (O/W) in the absence of the alcohol[16].
1.3 components of microemulsion
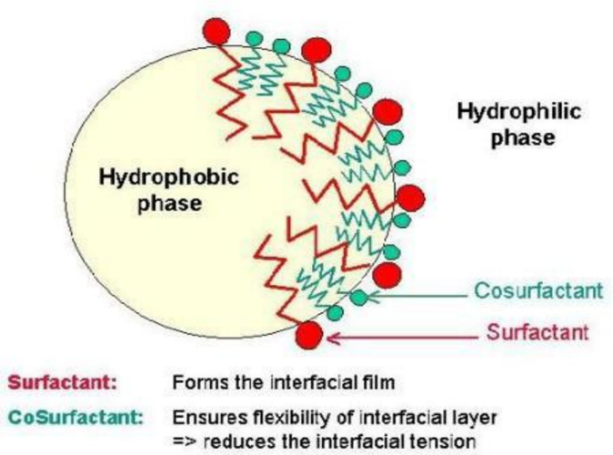
Fig. 1: Microemulsion Skeletal Structure.[11]
The microemulsion consists of hydrophobic phase (oil), hydrophilic or aqueous phase (water), emulsifying agents, gelling agents, additives[17,18].
1.3.1 Oil phase - The oil phase acts as a carrier for oil-soluble drugs. For example, light liquid paraffin which serves therapeutic or auxiliary purposes. With higher levels of the emulsifying agent, there is an observed increase in drug release.
1.3.2 Aqueous phase - Freshly boiled and cooled water is an aqueous phase for emulsion. When the drug or additive is soluble in water, it is dissolved in it before mixing with the oil phase.
1.3.3 Emulsifying agents - The emulsifying agents can be classified as
(i) Polysaccharides
Natural: acacia, tragacanth, starch.
Semi-synthetic: methyl cellulose, SCMC.
(ii) Surfactants
Anionic: alkali soaps, alkali sulphates.
Cationic: quaternary ammonium compounds.
Non-ionic: spans and tweens.
(iii) Finely divided solids
Clays, Milk of magnesia.
(iv) Sterol containing components
Wool fat, Beeswax, wool alcohols.
1.3.4 Gelling agents - These are classified into
(i) Natural gum
Alginates, Carrageenan, Tragacanth, Xanthan gum etc.
(ii) Carbomer
Carbopol 940, 941, and 934.
(iii)Cellulose derivative
Sodium Carboxy Methyl Cellulose (SCMC), Methyl cellulose (MC), Hydroxyl Propyl Cellulose (HPC) and Hydroxyl Propyl Methyl Cellulose (HPMC).
(iv) Poly ethylene
PEG 200, PEG 8000.
1.3.5 Additives
(i) Antioxidants: Rancidity is the usual problem associated with emulsions containing unsaturated fats and oils. Oil soluble antioxidants such as tocopherol, BHA, BHT are most suitable.
(ii) Preservative: The water phase is more sensitive to microbial growth and the preservative should concentrate more in the aqueous phase. e.g. sodium benzoate, benzoic acid, methyl paraben and propyl paraben, non ionic surfactants like Tween 20, Span 20.
1.4 Types of Microemulsion


Fig 2: Types of microemulsion structures [18] Fig 3: Winsor classification of microemulsion systems [19]
Although they are thermodynamically stable, microemulsions can only exist in particular conditions. Microemulsion phases, commonly known as Winsor phases, come in four different varieties. They are:
1.4.1 O/W microemulsion or Winsor I
Floating inside water, oil blobs get wrapped by surfactant molecules, often along with co-surfactants. Unlike emulsions where oil floats separately, this setup lets the covered droplets spread widely[11].
1.4.2 W/O microemulsion or Winsor II
Around each water drop floats a steady stream of oil in water-in-oil microemulsions. These setups go by the name “reverse micelles,” where the dense parts of the surfactant point inward toward the grease pool. Meanwhile, what would normally be the outer layer now reaches into the tiny water blob[16].
1.4.3 Bicontinuous microemulsion or Winsor III
In a bicontinuous microemulsion, there's roughly equal water and oil. Here, one is the continuous phase while the other forms separate domains. Instead of a single mixture, you see an uneven layer where oil and water blend like a "sponge-phase". When oil-in-water emulsions change to water-in-oil, that bridge can open. Inside this new phase, behavior bends like soft material. This slipperiness helps drugs get absorbed through skin without fuss. Not every form works so smoothly under real conditions. Yet this fluidity lends itself well to delivering medicine locally[20].
1.4.4 Single phase homogeneous mixture or Winsor IV
Mixed together, oil, water, and surfactants form one steady blend called Winsor IV, where everything mixes evenly without separation into layers[11].
1.5 Difference between Microemulsion and Macroemulsion [21, 22, 23]
|
Parameters |
Microemulsion |
Macroemulsion |
|
Appearance |
It is a transparent or translucent or clear solution (like water). |
It is an opaque or Milky White solution (like lotion). |
|
Globule Size |
Very small: 10-100 nm (nanometers). |
Large: 1-100 µm (micrometers). |
|
Stability |
Thermodynamically stable system (does not separate on its own). |
Kinetically stable system (Eventually, it might get separated). |
|
Preparation |
Forms spontaneously when components are mixed (No high energy needed). |
High energy is required (stirring vigorously/homogenizer). |
|
Viscosity |
Low (runny like water). |
High (thick like cream). |
|
Structure |
A dynamic structure with a constantly fluctuating interface. |
Hard droplets are dispersed in a continuous phase. |
|
Drug Penetration |
Very High (Due to small size and surfactants). |
Moderate (Larger globules penetrate the skin slowly). |
1.6 Advantages of Microemulsions
1.7 Disadvantages of Microemulsions
1.8 Skin

Fig 4: skin[25,26]
Various topical preparations are intended for dermatological application hence knowledge about skin is essential for formulating topical dosage form. The cutaneous membrane, which is the skin covering the external surface of the body, boasts an average adult surface area of approximately 2m² [25,26]. It consists of three distinct layers-
1.8.1 Epidermis
The outer layer of the skin, known as the epidermis, consists of stratified squamous epithelial cells, with the stratum corneum serving as its outermost layer[27]. The primary barrier function of the skin is facilitated by the interlocking platelet-like structure of highly keratinized corneocytes. It comprises various cells viz., melanocytes, merkel cells, langerhans cells, epidermotropic lymphocytes and dendritic epidermal cells. Melanocytes provide protection against ultraviolet radiation induced skin damage[27].
1.8.2 Dermis
The supportive connective tissue layer beneath the epidermis primarily comprises bundles of collagen and elastic fibers, establishing a reticular framework to support lymphatics and vasculature, nerves[27]. Fibroblasts, constituting a major portion of the dermis, collaborate with mast cells, which synthesize and secrete numerous active inflammatory mediators.
1.8.3 Subcutaneous layer: Provides cushion for dermis and epidermis. It consists of a sheet of fat rich areolar tissue.
1.9 Classification of Anti-fungal agents
Anti-fungal agents are classified based on their chemical structure and mechanism of action. They are,
1.9.1 Azoles
Imidazoles (like ketoconazole) and triazoles (like fluconazole, itraconazole, and voriconazole) are the two categories of azole antifungals. By inhibiting the lanosterol 14-alpha-demethylase enzyme, these medications prevent the synthesis of ergosterol by interacting with the development of cell membranes. Because of their wide range of activity and oral absorption, azoles are frequently employed[28].
1.9.2 Polylene
Fungal cell death results from the polyene's binding to ergosterol, which causes the fungal cell membrane to break down and intracellular chemicals to flow out. Nystatin and amphotericin B (AmB) are among them[29].
1.9.3 Echinocandins
Biosynthesis of the fungal cell wall is something that is missing in mammalian cells and this is where echinocandins like caspofungin, anidulafungin, and micafungin aim. Together, they prevent the fungus from producing 1,3-β-glucan synthase. As a result, the fungal cell wall loses 1,3-β-glucan, one of its primary constituents, causing osmotic formation and cell death[29].
1.9.4 Allylamines
Another enzyme in the ergosterol production pathway, squalene epoxidase, is inhibited by terbinafine, the most well-known allylamine. It is mostly used to treat skin diseases, like onychomycosis (fungal nail infection) and tinea pedis (athlete's foot)[28].
1.9.5 Pyrimidine analogues
Fungal cells transform flucytosine into fluorouracil, which prevents the formation of DNA and RNA. To treat serious infections like cryptococcal meningitis, it is usually used in conjunction with other antifungals such amphotericin B[28].
1.10 Mechanism of action of Anti-Fungal agents
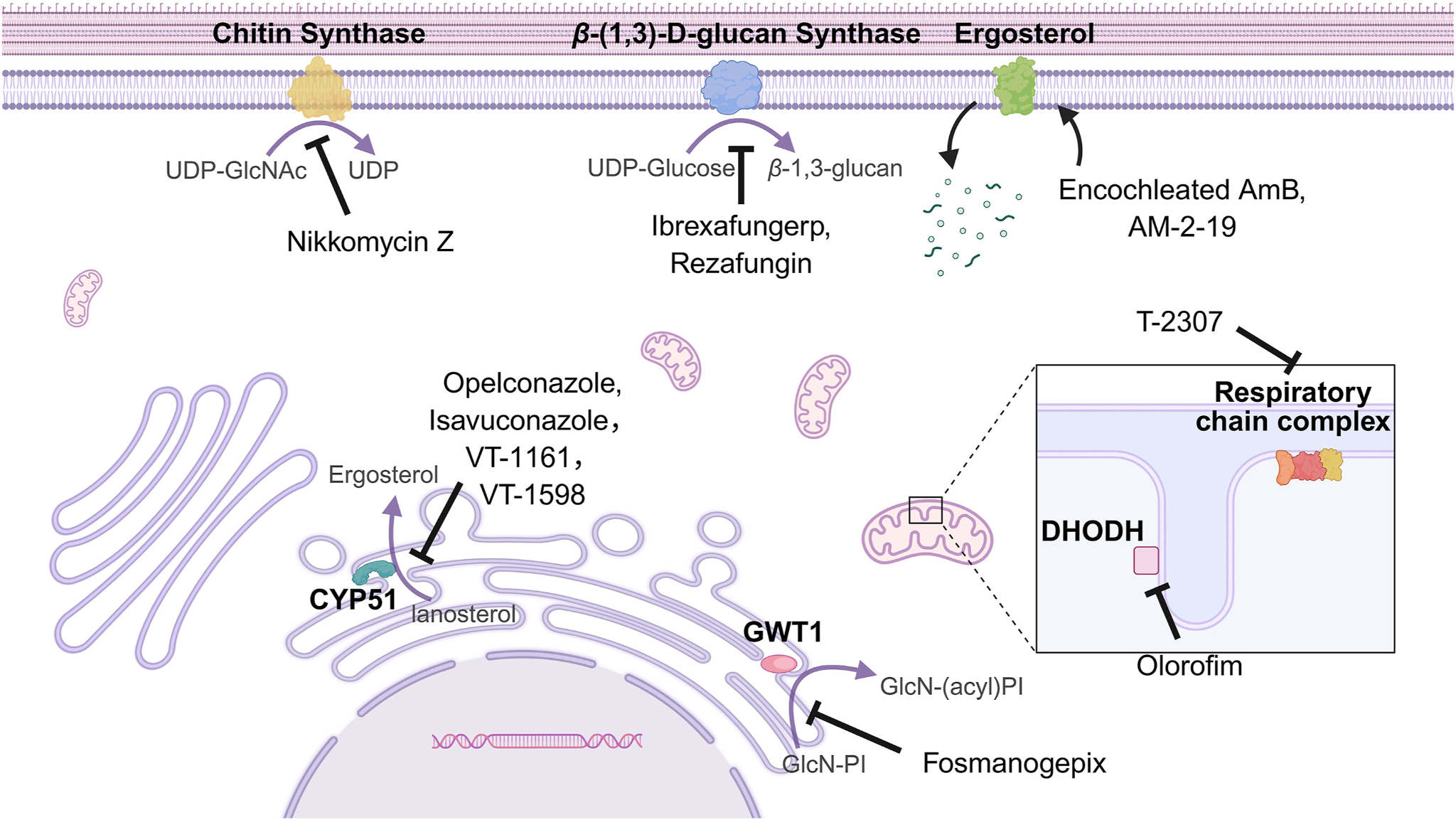
Fig 5: Mechanism of action of anti-fungal drugs [30]
Stratum corneum is the outermost layer of epidermis and it is formed by well keratinized cells. Fungal infection mostly affect the outermost layer as it a nutrient rich surface for fungi.[1,31] When antifungals are applied topically, the therapeutic ingredients must cross the stratum corneum, the skin's outermost layer, in order to reach the skin's lower layers, especially the viable epidermis.[25] To ensure effective drug concentrations after topical administration, medications must penetrate through all layers of the skin.[32] Mostly, Azole derivatives are used as they are suitable for this type of formulation. By interacting with the phospholipids in the cell membrane of fungus, azole antifungals change the permeability of the cell membrane and selectively prevent the formation of ergosterol in fungal cells by inhibiting their synthesis.[33] Antifungal azoles mainly affect ergosterol production by inhibiting the cytochrome P450-dependent process that converts lanosterol to ergosterol by targeting 14'-lanosterol demethylase, which is produced by the ERG11 gene. In addition to interfering with ergosterol's general functions as a membrane component, severe ergosterol depletion may also interfere with ergosterol's properties, resulting in decreased fungal cell growth[34]. The formulation's capacity to penetrate the stratum corneum barrier and improve absorption in deeper skin layers determines the therapeutic efficacy[35]. Microemulsions' oils and surfactants act as enhancers for medication penetration through the stratum corneum. The internal structure of phases and the microemulsion formulation components increase the drug's diffusion and it can improve the drug's partition to the stratum corneum[36].
The most effective way to deal with large skin dermatophytes is mostly the topical application of antifungal medications, it provides direct access and a high retention rate at the target[37].
Several Anti-fungal microemulsions containing drugs such as clotrimazole, itraconazole, and ketoconazole, are applied topically to the skin by rubbing or spreading. [38,39,40]
1.11 Microemulsion based hydrogel or Emulgel
Water-loving molecules start as monomers in hydrogels. These chains link together through chemical bonds, creating a porous structure. A special helper called a crosslinker guides how the strands connect. Over time, these links form a gel-like material that traps water. The result is a network of polymer chains soaked in moisture. The hydrogel's capacity to absorb significant amounts of water through hydrogen bonding is improved by void defects and a net-like structure. [18]. Despite having benefits for skin application, microemulsions often lack stability due to thin consistency. A fix comes through blending them into gel form using natural binders like xanthan gum or substances like HPMC and Carbopol that enhance structure and control release[1]. Microemulsions have both emulsion and gel properties. Their unique behavior comes from two active layers working together. Water stays trapped better because less escapes into the air. This formula works without causing harm as it is non-toxic [5].
Chapter 2. Study carried out on various anti fungal drugs
|
Sr No. |
Drug |
Oil |
Smix |
References |
|
1. |
Itraconazole
|
Milletia pinnata (Karanj) oil (5%) |
Carboxymethyl -Tamarind gum (CMTG), Carbpol (1:1) |
Ansair N A et al. (2022)[3] |
|
Isopropyl myristate
|
Tween 80 and PEG 400Smix ratio of 3:1 |
Gangotri Yadav et al. (2023)[41] |
||
|
Eucalyptus oil |
Tween 20 and methanol |
Patel et al. (2018)[42] |
||
|
Karanj oil |
Tween-80, Carbopol-934 |
Gadave B et al. (2021)[43] |
||
|
2. |
Miconazole nitrate |
Isopropyl palmitate (10-13 %) |
Span 80(2-5%), PEG400 (0.5-0.7%) |
Bhonge A et al. (2024)[44] |
|
Oleic acid |
Tween 20 and propylene glycol |
Iram Shahzadi et al. (2014)[45] |
||
|
Liquid Paraffin- 3% |
Tween 20, SPAN 20 – 0.6% |
Ashish Bhaumik et al. (2024)[46] |
||
|
3. |
Ketoconazole |
Rose oil (2.5 %) |
Cremophor RH 40, Tween 20 and carbopol 971P (2.5 %) |
Jain P et al. (2023) [5] |
|
Nigella oil |
Transcutol and Propylene glycol |
Kesrin Amra et.al (2019)[47] |
||
|
4. |
Amphotericin B 0.1% (w/w) |
Isopropyl Myristate 5% (w/w) |
Tween 80 and Propylene glycol Smix (3:1) 35% (w/w) |
Butani D et al. (2014)[48]
|
|
5. |
Croconazole |
Eucalyptus oil (20 % v/v) |
Tween 80, ethanol or propylene glycol. (30 % v/v) |
El-Badry M et al. (2013)[49]
|
|
6. |
Curcuma longa, Azadirachta indica |
Olive oil |
Tween 80 and PEG 600 |
Giri S et al. (2024)[50] |
|
7. |
Bifonazole (1%)
|
Oleic acid (6.25)% |
Tween 80, IPA (55%, 3:1) |
Sabale V et al. (2012) [1] |
|
8. |
Fluconazole
|
Isopropyl Myristate (5%) |
Labrasol, plurol oleique (45%, 4:1) |
Magdum C et al. (2009)[18]
|
|
Clove oil and lemon grass oil |
Tween 20, Tween 80 and Propylene glycol |
Pavankumar K M et .al ( (2021)[ 51] |
||
|
9. |
Sertaconazole |
Oleic acid (8.75%, w/w) |
Tween 80 and Propylene glycol (33.35%, w/w) |
Sahoo S et al. (2014)[21]
|
|
10. |
Luliconazole |
Linseed oil (5%) |
Tween 20 and Span 20 |
Dandagi, et al.(2019)[5] |
|
11. |
Griseofulvin |
Oleic acid (5%)
|
Tween 80 and ethanol (1:1) |
Aggarwal N et al. (2013)[52]. |
|
12 |
Naftifine hydrochloride (naftifine) |
oleic acid (oil) |
Kolliphor RH40 + Transcutol |
Erdal MS et al. (2020)[53] |
|
13 |
Terbinafine HCl |
Ajowan oil + peppermint oil |
Tween 80, Propylene Glycol |
Mehta and Bhatt, IJPSR, (2011)[54] |
|
Oleic acid |
Labrasol S and Transcutol P |
S. Baboota et.al (2007)[55] |
||
|
14 |
Itraconazole and clotrimazole |
benzyl alcohol |
Tween® 60 and propylene glycol |
Patricia Garcia Ferreira et.al(2019)[56] |
|
15 |
Butenafine hydrochloride |
compritol 888 ATO labrasol |
Tween 80 |
Mahdi WA et al. (2021)[57]. |
|
16 |
Lidocaine HCl and ketorolac |
Jojoba oil |
Brij 97 and hexanol |
Assaf, Shereen Mashhour, et al.(2021)[58] |
|
17 |
Ibuprofen |
Miglyol 840 |
Labrasol and Triton X 100 |
Salunkhe S S et al. (2014)[59]. |
|
18 |
Posaconazole |
Cinnamon oil (0.2%) |
Tween-80 (0.4%), poloxamer-188, transcutol (0.2%) |
Gorle A et al. ( 2022)[60]. |
|
19 |
Limonene |
Limonene oil |
Polysorbate 80 ,Poloxamer |
Budiarto, R., Khalisha, A., Sari, D.N. et al. (2024)[61] |
|
20 |
Quercetin |
Olive oil |
Tween 80,Chitosan |
Alsaleem MA et al. (2024)[62] |
|
21 |
Ezetimibe |
Semisynthetic oil |
Tween 20, Poloxamer |
Yadav P, Rastogi V, Verma A[63] |
|
22 |
Cymbopogon citratus |
Essential oil |
Citral ,Carbopol |
Wen J et al. (2023)[64] |
|
23 |
Clotrimazole |
Liquid Paraffin - 4%
|
Tween 20, span 20, Propylene glycol (0.5%), Carbopol 934 (1%) |
Ghada E. Yassin1(2014)[65]
|
|
Isopropyl myristate |
Labrasol and Cremophor |
Zhang, Ji at.el (2018)[66] |
||
|
Clove oil (~15 %) |
Brij -35 (~30%)
|
Yasir Siddique M et al. (2021)[67] |
||
|
24 |
Curcumin |
Coconut oil |
Tween 80, Poloxamer |
Patil V et al. (2022)[68] |
|
25 |
Lycopene |
Olive oil |
Tween 80 , Carbopol |
Bhalke RD et al. (2022)[69] |
|
26 |
Acorus calamus |
Calamus oil |
Pearl powder, Carbopol |
Peng L et al (2023)[70] |
|
27 |
6-Gingerol |
Ginger oil , corn oil |
Tween 80 , labrafrac |
Aziz EK et al.(2025)[71] |
|
28 |
Nystatin |
Oleic acid |
Tween?20, Propylene glycol |
Pak. J. Pharm. Sci., Vol,, July (2019)[72] |
|
29 |
Thiobarbituric acid |
Shrimp oil |
Tween 20, Carbopol |
Takeung Wongtrakul S et al. (2013)[73] |
|
30 |
Thiophene derivative 5CN05 |
Iso-propyl myristate |
LAS, Plurol Oleique |
Guimarães GP et al. (2014)[74]. |
|
Caspofungin |
Liquid Paraffin |
Tween 20, Span 20 and Propylene glycol |
Sonawane N D et al. (2025)[75].
|
|
|
32 |
Cyclodextrin |
Volatile oil |
Tween 80,Carbopol |
Singh, J., Dhamija, I., Meehenian, H. et al(2022)[76] |
|
33 |
Candesartan citexetil |
Oleic acid |
Labrafac PG ,Proniosomal |
Ali, H.H., Hussein, A.A (2017)[77]. |
|
34 |
Cyclosporine |
Oleic acid |
Tween 80 and Transcutol |
Marta Benigni et.al (2018 )[78]. |
|
35 |
Voriconazole |
benzyl alcohol (10 %) |
N-methyl-2-pyrrolidone, ethanol/phosphatidylcholine mixture (3:2) |
Kim Y H et al. (2014)[79]. |
|
36 |
Econazole Nitrate |
Oleic acid |
Propylene glycol and tween 20 |
Sukre, M et.al (2022)[80] |
|
37 |
Efinaconazole |
Tee tree oil |
Tween20, Tween80, Propylene glycol |
Mamatha G T et al. (2022)[81].
|
|
38 |
Tavaborole |
Caprylate/Capric glycerides (21.45% w/w) |
Glyceryl Caprylate/Caprate (7.8%), Polyethylene glycol-8, Diethylene glyol monoethyl ether (21.45%) |
Agrawal V et al. (2022)[82]. |
Chapter 3. Experimental Methods
3.1 Methods of preparation of microemulsion
3.1.1 Phase Titration method (Spontaneous emulsification)
When mixing different ingredients, a phase diagram helps explain microemulsions, one example being phase titration[20]. Building these diagrams reveals how various forces connect during composition. The way substances interact depends on their makeup and proportions, the compatibility of the ingredients shapes the behavior of microemulsions[83]. Figuring out where the different phases meet matters in science work. A pseudoternary phase diagram where every corner shows 100 % of one ingredient helps map out the areas making up a microemulsion. This avoids the trouble of handling complex four component graphs (Figure 4). When looking only at mix ratios, like whether water or oil dominates, the blend splits clearly into O/W or W/O form. While observing, care must be taken so that the unstable systems are left out[24].

Fig 6: Phase Titration[20].
3.1.2 Phase Inversion method
When more of the dispersed phase goes into a mix or if temperature shifts, microemulsion phase inversion occurs. This can bring big shifts like alterations in particle dimensions that influence how drugs let go during lab tests and body trials[24]. These shifts are driven as there is a tweak in the surfactant's built-in curvature shape. This can be achieved for non-ionic surfactants by changing the system's temperature, resulting in a change from an oil-in-water microemulsion at low temperature to a water-in-oil microemulsion at high temperature. The formation of finely dispersed oil droplets is supported when the system reaches a point of zero spontaneous curvature and low surface tension during cooling.[16] This is called as Phase inversion temperature method. Instead of just heat, salt concentration or pH level is also considered. Amount of water which fills the blend can tweak where it naturally bends. Droplets form mostly within oil when water gets mixed into it step by step. As more water is added, the way surfactants bend, space changes too. Instead of holding water inside oil, they start shaping oil around water. This shift happens when water makes up a larger share of the mixture. At that moment, surfactants at the oil-water boundary form loose layers that quietly arrange themselves into two separate oily spaces threaded by water channels. That structure appears exactly where the inside and outside swap roles[83].

Fig 7: Phase Inversion[84].
3.1.3 Agitation method
The drug dissolves in the oil or lipophilic portion of the microemulsion, which is the oil and water phases. A cosurfactant is then added gradually while stirring the mixture until it becomes transparent. The Pseudoternary phase diagram is used to determine the exact amount of surfactant and co-surfactant as well as the percentage of oil phase that can be included. Finally, the required size range for dispersed globules can be obtained by using an ultrasonicator.[83]

Fig 8: Agitation[20].
3.2 Methods of preparation of Microemulsion based gels
3.2.1 Formulation of gel base
Starting off with water, some polymer gets added either by soaking or dissolving exactly the right amount. It is mixed gently using a magnetic stirrer at moderate speed. At this stage, acid or base might come into play, helping shape the balance just right across the pH scale [53].
3.2.2 Formulation of emulsion
Oil phase and aqueous phase are prepared separately. The surfactants and emulsifiers are added to these phases. They are heated separately and then oil gets mixed into water under steady stirring until it reaches room temperature, forming an emulsion[80].
3.2.3 Emulgel formulation
With continuous stirring, the prepared emulsion is slowly added to the gel in different proportions and it is stirred continuously[85]. The emulgel is prepared and it is adjusted for the texture, stability and viscosity.
3.3 Characterization of microemulsions / emulgels
Microemulsions or emulgels are characterized using various techniques such as,
3.3.1. Visual Appearance and physical test
Ideally, microemulsions should be transparent, they should have a uniform appearance with no formation of lumps or clumps, their phases should not separate, they should have a uniform viscosity and no turbidity. Hence, their appearance, consistency, grittiness, colour, texture, homogeneity, phase separation, viscosity and optical clarity are visualized with naked eyes[16,86]. These physical tests can confirm whether they are stable, safe and suitable for topical application.
3.3.2. Droplet size and poly dispersity index (PDI)
The size of the droplet should be small so that it penetrates well and shows better optical clarity. The PDI tells us whether the droplets are all similar in size or not. Their values should be from 0.3 to 0.7 which gives uniform droplets, high PDI can lead to droplet aggregation. The average droplet size and PDI is determined with accurate dilution in distilled water with the help of photon correlation spectroscopy (Zetasizer Nano ZS90, Malvern Instruments, UK)[21].
3.3.3. Viscosity determination
The uniform viscosity ensures easy spreading on the skin. Microemulsions should have a low viscosity which is not runny like water but close to water. Whereas, microemulsion based gels (emulgels) should have a moderate to high viscosity. A Brookfield Viscometer, specifically model LVDV-II+pro, takes care of measuring this property. From there, it moves on to picking the correct spindle. Then comes adjusting both speed turns per minute and twisting force levels. Ready specimens stay prepared throughout the process while results emerge through flow behavior checks[69].
3.3.4. Drug content study
It is important to check the exact amount of drug present in formulated microemulsion (accurate drug loading) and also whether it is uniformly distributed or not. This prevents under-dose or over-dose of the drug. In this method, a known quantity of formulation is added to a suitable solvent, it is then stirred, filtered and analyzed using a UV-visible spectrophotometer[69].
3.3.5. Determination of pH and percent transmittance
The pH should be close to skin pH, i.e. 5.5 - 6.5 to avoid skin irritation and drug degradation. The percent transmittance indicates the amount of light passed through the formulation which tells that the formulation is clear or turbid. The formulation is diluted with distilled water and the pH is measured using a digital pH meter (Lab India PICO+). The percent transmittance is measured by UV visible spectrophotometer at 550-650 nm wavelength against continuous phase or distilled water as blank. If the % transmittance is more than 90% than it shows goof optical clarity but if it is less than 90% then it shows turbidity[26].
3.3.6. Stability study
It is necessary to check whether a formulation is physically, chemically and therapeutically stable over time and hence, it is evaluated by storing the formulation under different storage conditions to confirm its shelf life. It is tested by mixing or centrifuging small amount of sample and it is examined if there occurs any phase separation or other changes. Further, the stability is tested at different temperature and humidity conditions for months as per ICH guidelines[69].
3.3.7. Spreadability studies
Spreadability is an important parameter of a formulation as it is the ability to spread easily and uniformly during the topical application and therefore, it should have a reasonably higher spreadability value. It ensures uniform drug distribution. TA-XT plus texture analyzer (Stable Microsystem, UK) is used to determine the spreadability of the formulation[8].
3.3.8. In-Vitro Drug Release Studies
It predicts the amount and rate of drug released from a formulation into a release medium under laboratory conditions. It ensures controlled and sustained drug release. It is done using a Franz diffusion (FD) cell and buffer solutions such as phosphate buffer, acetate buffer, citrate buffer, etc[3,5,87]. Fitting results against different models helps reveal how drugs leave the system, it includes zero order, first order, Higuchi matrix, or Korsmeyer-Peppas patterns. The one showing the strongest match, based on data points, becomes the main choice when R2 values stand highest[88].
3.4 Construction of Pseudoternary Phase Diagram [17,89]
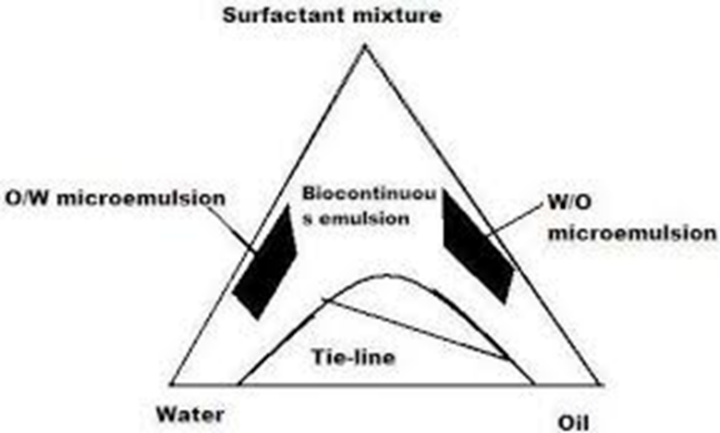
Fig 9: Ternary phase diagram showing microemulsion regions[11]
The water titration method is generally used to make these pseudoternary phase diagrams involving oil, water, and surfactant or co-surfactant[11]. The water dilutes the oil and surfactant or co-surfactant mixtures at certain weight ratios. First, mix oil, surfactant, and co-surfactant in a specific ratio. Stir it for about five minutes until the mixture looks clear and uniform. Then, start adding water slowy*, this is the titration part. As we add water, we have to observe how the mixture flows and check if it stays clear or gets cloudy. After weighing everything carefully, the exact water concentration where the mixture changes from clear to cloudy or vice versa is figured out[89]. This helps calculate the surfactant or co-surfactant mixing ratio and defines the boundaries of the microemulsion region for the chosen oils. Also, to see how adding a drug affects this microemulsion boundary, phase diagrams are plotted again with drug-enriched oil as the hydrophobic part
CONCLUSION
Topical antifungal gel-based microemulsions have proven themselves to be a novel and successful method for treating superficial fungal skin infections. Conventional dosage forms like creams and ointments may have limited penetration, poor drug solubility and frequent application requirements, all of which can lower patient compliance and treatment results. Microemulsions help get around these limitations by providing a number of benefits. Both lipophilic and hydrophilic medications can be dissolved by these transparent, stable solutions composed of oil, water, surfactant and co-surfactant. The medication can more successfully penetrate deeper into the layers of skin because of its small droplet size. The addition of microemulsions to a gel or emulgel basis improves the formulation's consistency, spreadability and application ease which makes it more comfortable and appropriate for topical use. According to the studies evaluated in this paper, antifungal medications developed as microemulsion-based gels show better drug release, greater skin penetration, and better drug retention as compared to conventional formulations. Various formulations showed better therapeutic effects and antifungal activity. Azole antifungal drugs such as clotrimazole, ketoconazole, itraconazole, fluconazole etc., were found to be effective when they are administered through microemulsion-based gel systems.
The appropriate selection and optimization of oils, surfactants, co-surfactants, and gelling agents is essential for the successful formulation of microemulsion-based gels. It is made sure that there is no phase separation, instability and skin irritation due to these gels. That is why a well-balanced composition is formulated. These systems are evaluated based on the evaluation parameters like droplet size, viscosity, pH, spreadability, stability, and in-vitro drug release.
Overall, topical antifungal microemulsion-based gels represent a promising approach for a patient-friendly drug delivery system. They provide improved stability, enhanced skin penetration, and better therapeutic effect as compared to traditional topical formulations. With continued research and formulation optimization, these systems have strong potential for future pharmaceutical development and greater clinical use in the management of fungal skin infections.
REFERENCES




C. Apeksha, J. Samruddhi, G. Arya, D. Snehal, Dr. Jangme C. M., Microemulsion-Based Gels: A Hybrid Platform for Enhanced Anti-fungal Therapeutic Delivery, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4534--4557. https://doi.org/10.5281/zenodo.18810891
 10.5281/zenodo.18810891
10.5281/zenodo.18810891