Sai School of Pharmaceutical Education and Research, Sri Sai University Palampur
Diabetic retinopathy (DR) is a leading cause of vision loss globally. This review discusses the molecular mechanisms underlying DR, its global prevalence, and current treatment strategies. We explore the role of hyperglycemia-induced pathways, including the polyol pathway, protein kinase C activation, and advanced glycation end-product formation, in the development of DR. Additionally, we examine the potential of emerging therapeutic targets, such as inhibitors of vascular endothelial growth factor (VEGF) and neurotrophic factors, in preventing DR progression.
Diabetes mellitus (DM) characterized by chronic circulating hyperglycemia due to resistance or impaired insulin secretion found in all age groups of people. DM having high prevalence & societal impact globally. Due to the significant number of patients year by year. Due to chronic circulating hyperglycemia gradually knowingly- unknowingly face the secondary complication. Diabetes related complications affect almost all organs & systems and are responsible for the high morbidity and mortality. It is a leading cause of renal failure, blindness, nerve damage, foot ulcers and various cardiovascular disorders and more than that. Early diagnosis of DM requires vision loss. Chronic circulating hyperglycemia causes irreversible pathological alteration such as microangiopathy, microaneurysm, hemorrhages and basement membrane thickening in retina eye globe & kidney(Antonetti. et al 2012). Due to high circulating hyperglycemia, microvascular complication in the kidney leads to proteinuria, decreased glomerular filtration & interstitial fibrosis & secondary infections. Some cases also observed cystitis and asymptomatic bacteriuria & pyuria. Long standing DM leads to proliferating diabetic nephropathy (DN), neovascularization & diabetic macular oedema. Mechanisms for vascular disease in diabetes includes the pathologic change of glycation end product and leads to accumulations. Impaired vasodilator response and leakage and attributes to nitric oxide formulation leads to chronic inflammation and enhanced platelet aggregation. Vascular changes in some patients include leakage of fluid into the rear of the eye macular oedema. Diabetic retinopathy (DR) is the most frequent cause of new cases of blindness among adults in developed countries. Glaucoma, cataracts and other disorders of the eye occur earlier and more frequently in people with DM. Diabetic nephropathy mainly occurs due to pathological alteration in the glomeruli and thickening of mesangial and basal layers. Rodent models are mostly studied to develop the DR model. Rodents have a short life span, small gestational period, small size, easy to handle and most of the genetic studies were carried out. DN is considered as an end stage disease therefore its need to study the molecular mechanism. This model will help in well understanding of the pathogenesis of DR and DN from DM for the development of novel therapeutic molecules.
International Status:
DMs have a very high socio-economic impact and it’s found globally. DM is prevalent in all communities irrespective of race, age and sex. Worldwide prevalence of DM is 9.2% in women and 9.8% in men. Due to change in the lifestyle & habit DM high prevalence in the developed countries as compared to developing countries. DM may find double the during next 2 decades. Global Status of DM, 382 million currently which may rise to 592million humans by 2035(Nanidta et al 2016). The DM has 25 times more chances of vision impairment as compared to non-diabetes. Diabetic retinopathy is 1/3 among the DM population. Type 1 diabetes possesses more DR than type 2. Due to chronic circulating hyperglycaemia for more than 20 years all the population of type 1 DM & more than 60% of the population of type 2 population have some degree of retinopathy or vision problem. Proper management of DM calls to avoid vital secondary complications including cataract, retinopathy, nephropathy, neuropathy & cardiovascular. Diabetic retinopathy is the leading cause of blindness globally. Body will produce very little endogenous insulin. Therefore, it needs to take the insulin either by subcutaneous injection or remedies by oral. Blood glucose level should be periodically monitored and managed otherwise chronic hyperglycemia leads to secondary complications. Affected populations with type 2 diabetes are at high risk to develop secondary complications.
National Status:
Nowadays DM is highly prevalent, across all sections of society from villages to urban areas but more common in urban areas in India. India accounted for approximately one sixth of the global burden of DM in 2011. It is increasing day by day and projected to increase to 101 million by 2030 making it the 'Diabetes Capital' of the world(Salil S Gadkari, Quresh B Maskat et al)Aetiology of DM in India is multifactorial. It includes genetic factors, influence of the environmental factors, lifestyle and food habits.
The level of morbidity and mortality due to DM and its potential complications are enormous and found significant healthcare burdens on both families, society and on the country. In India, there is continuous migration of people from rural to urban areas due to less job opportunity. The stress, economic boom, corresponding change in life-style and food habits of urban people have accelerated DM prevalence. In India several herbal companies export the fenugreek seeds extract as dietary supplement to benefit the diabetic patients. Still, no studies are reported about fenugreek seeds extracts or its constituent i.e. 4-hydroxyisoleucine for secondary complications of diabetes.
Diabetic retinopathy is the leading cause and common cause of visual loss in the world and it is a potentially blinding complication of diabetes that damages the eyes retina. Diabetic retinopathy is a burning problem globally. It is progressive disease that results from vascular injury due to chronic hyperglycemia. It is a vascular disorder affecting the microvasculature of the retina. DR occurs both in type 1 and type 2 diabetes mellitus and has been shown that nearly all type 1 and 75 percent of type 2 diabetes will develop DR after 15 yr duration of diabetes. In India with the epidemic increase in type 2 diabetes mellitus as reported by WHO, diabetic retinopathy is fast becoming an important cause of visual disability. Non-insulin dependent diabetes mellitus may be the most rapidly growing chronic disease in the world. Its long-term complications include retinopathy, nephropathy, neuropathy and accelerated macrovascular disease which causes major morbidity and mortality. Diabetic retinopathy is a complication of diabetes that affects the blood vessels of the retina.
Induction Models
Pancreatectomy
One of the oldest techniques used to induce diabetes in animal models is pancreatectomy, the elimination of the pancreas or removal of ? cells from the pancreas. Pancreatectomy was observed in 1922 to increase blood sugar level in dogs. In case monkeys, pancreatectomy at various ages between 6 and 15 years resulted in insulin dependency and hyperglycemia, which was then deliberately uncontrolled. This was observed to lead to BRB leakage within 1 year of hyperglycemia onset.
Alloxan
The first drug found to result in diabetes, alloxan, was discovered by Dunn and McLetchie in 1942. Alloxan is a derivative of uric acid and directly targets ? cells located in the pancreas Alloxan-directed cell demise is mediated through inhibition of glucokinase, an enzyme concerned in the glucose-insulin regulatory pathway and expressed in the liver and pancreas. (Maria Olivares et al.
Diabetes mellitus induced by ferric nitrilotriacetate
This is an uncommon procedure. After approximately 60 days of treatment, rats and rabbits treated parenterally with a high daily dose of ferric nitrilotriacetate developed diabetic symptoms such as hyperglycemia, glycosuria, ketonemia, and ketonuria.
Blood insulin response to oral glucose loading was inadequate (Awai et al., 1979). Diabetes mellitus induction with ditizona or anti-insulin serum has never been reported.
Diabetes mellitus model with streptozotocin
Streptozotocin (STZ) is a synthetic nitrosoureido glucopyranose derivative isolated from Streptomyces achromogenes fermentations that is used as an antitumor antibiotic and is chemically related to other nitrosoureas used in cancer chemotherapy.
As a chemotherapy agent, sterile powders of streptozotocin are provided and prepared. Each sterilized Streptozotocin powder vial contains 1 gram of Streptozotocin active ingredient 2-Deoxy-2[(methylnitrosamino)-carbonyl] amino]. -Glucopyranose, as well as 200mg Streptozotocin is available as a dry-frozen, pale yellow sterilized product for intravenous use. Diabetes mellitus induction with STZ takes time, and experiments performed at appropriate time intervals after administration of the agent will provide additional information about the mechanism of action of the tested compound. During the early stages of this induction period, hypoglycemic action of plant extract may be due to stimulation of residual activity of -cells; however, after induction of the diabetic state, hypoglycemic activity will be due to some other mechanism, because insulin activity is thought to be negligible in this model of diabetes. A single dose of STZ in a sterile citrate buffer (e.g., pH 4.5 0.1M) may be effective.
Pathogenesis
Normal retinal endothelial possess specialized barrier properties similar to those characterizing the blood-brain barrier, which are absent in the vasculature of most non-neural tissues. These properties include ultra structural features(complex tight junctions, absence of fenestrations, paucity of pinocytotic vessels) and speci?c antigen expressions most notably that of the glucose transporter protein isoform 1 (GLUT1) (North et al 2003).Hyperglycemic changes occur in nonvascular cell type that play important role in development and progression of diabetic retinopathy. Ischemia-induced angiogenesis and expansion of extracellular matrix (ECM) in association with the outgrowth of ?brovascular membranes at the vitreoretinal interface is the pathological hallmark in proliferative diabetic retinopathy (PDR)(Abu.et al 2013). Proliferative vitreoretinopathy (PVR) is a process of ?brocellular proliferation on either side of the retina that may complicate hegmatogenous retinal detachment. The mechanisms that regulate angiogenesis and ?brosis in proliferative vitreoretinal disorders are incompletely characterized (Abu.et al 2011). A role for angiogenic and ?brogenic factors is under increasing evaluation.Vascular endothelial growth factor (VEGF), a major proangiogenic mediator, is thought to be the major angiogenesis factor in PDR (Spranger& Pfeiffer 2001). DR is classified mainly in 2 categories i.e. earlier stage of nonproliferative diabetic retinopathy (NPDR) and chronic and advanced cases of proliferative diabetic retinopathy (PDR). In NPDR visible features, including microaneurysms, retinal hemorrhages, intraretinal microvascular abnormalities (IRMA), prominent vasculature, peripheral increase in vasculature, and venous caliber changes (Fig. 1), while PDR is characterized by the hallmark feature of pathologic preretinal neovascularization(Stitt. Et al 2016).
It can be used as tools for prognosis of ongoing pathogenesis. Due to breakdown of blood-retinal barrier (BRB) leads to Diabetic macular edema (DME) which is found in both NPDR & PDR. Due to DME the extravasation of fluid leads to abnormal retinal thickening caused by cystoid edema of the macula(Zhang, et al 2014).
The accumulation of certain advanced glycation end products (AGE) in the long-lived proteins that are found at higher retinopathy risk (Genuth S, et al.2015). The loss of memory phenomenon showed support from studies in animal models of diabetic retinopathy that are returned to normoglycemia (achieved using insulin therapy) due to reversal of hyperglycemia-mediated oxidative damage (Zhong. et al 2011)

Fig: 1. Figure showing the difference between normal eye vessels and diabetic retinopathy eyes
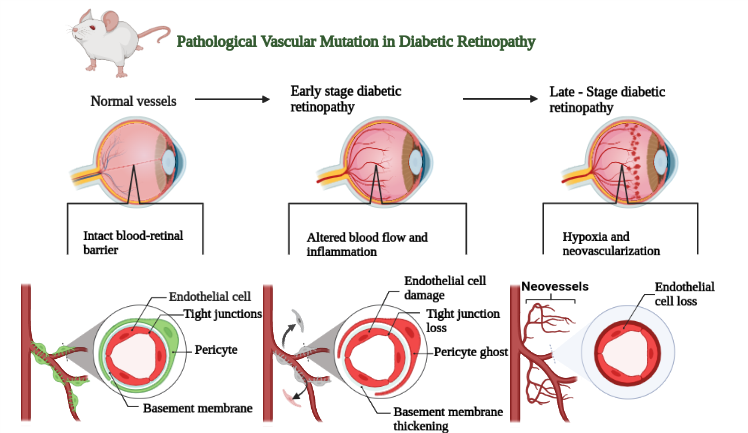
Fig: 2. Figure showing the pathological vascular changes in diabetic retinopathy
Prevention therapy
CONCLUSION
Diabetic retinopathy (DR) is a leading cause of vision loss and blindness worldwide. It is a complication of diabetes that affects the small blood vessels in the retina, the light-sensitive tissue at the back of the eye. DR can cause a variety of vision problems, including blurred vision, floaters, and difficulty seeing at night. In severe cases, DR can lead to complete vision loss.
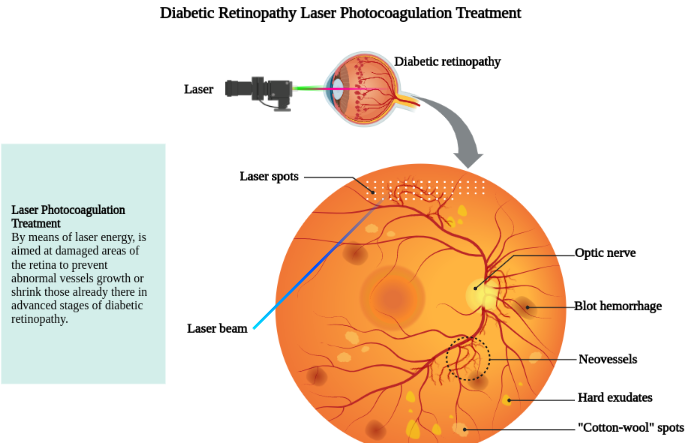
There is no cure for DR, but early diagnosis and treatment can help prevent vision loss. Treatment options include laser surgery, anti-VEGF injections, and corticosteroid injections. In some cases, surgery may be needed to remove scar tissue or restore blood flow to the retina.
If you have diabetes, it is important to see an eye doctor (ophthalmologist) for a dilated eye exam at least once a year. Early detection and treatment of DR can help prevent vision loss.
Here are some tips for preventing DR:
REFERENCES



Shoket Ali*, Chirag Mehra, Aditya Singh Chaudhary, Molecular Review on Modern Perceive, Mechanism, Global Recurrence and Treatment Plans for Diabetic Retinopathy, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 1969-1974. https://doi.org/10.5281/zenodo.14462207
 10.5281/zenodo.14462207
10.5281/zenodo.14462207
