Satyajeet College of Pharmacy Mehkar, Ta. Mehkar, Dist. Buldhana 443301
Tuberculosis (TB) is a contagious infection that usually attacks not only the lungs, but also brain and spine. More than twenty drugs have been developed for the treatment of TB, but most of them were developed some years ago. They are used in different combinations. Isoniazid and Rifampicin are examples of the five first line TB drugs, whereas, for instance, Levofloxacin, Kanamycin and Linezolid belong to the second line drugs that are used for the treatment of drug resistant TB. Several new bicyclic nitroimidazoles (e.g., Delamanid) without mutagenic effects were developed. New TB drugs need to provide several main issues such as more effective, less toxic, and less expensive for drug resistant TB. Besides polymeric, metal-based nanoparticles, polymeric micelles and polymers, dendrimer nanostructures represent ideal delivery vehicles and offer high hopes for the future of nanomedicine. In this original review, we present and analyze the development of anti-TB drugs in combination with dendrimers. Few articles have highlighted the encapsulation of anti-TB drugs with dendrimers. Due to their unique structure, dendrimers represent attractive candidates for the encapsulation and conjugation of other anti-TB drugs presenting important drawbacks (e.g., solubility, toxicity, low bioavailability) that hinder their development, including clinic trials.
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium
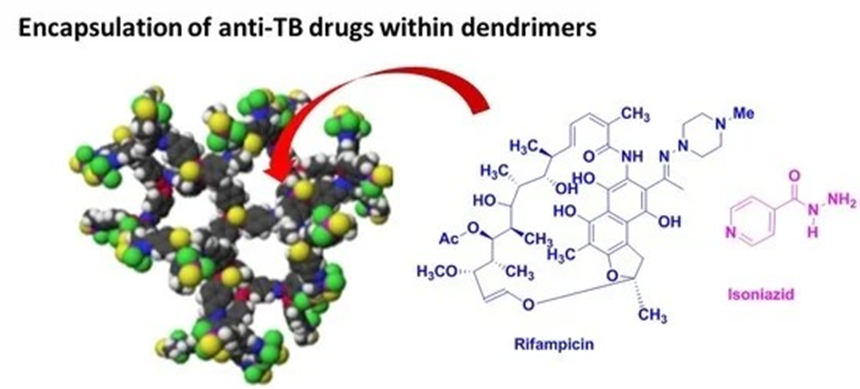
Fig no: -01
tuberculosis, also known as Koch bacillus, surviving and replicating within human alveolar macrophages and affecting other organs
* A global view of this disease can be summarized as follows:
according to the latest report of the World Health Organization (WHO), more than one third of the world’s population is infected with Mycobacterium tuberculosis, and approximately 2 million deaths by TB were reported in 2017; (2) current treatments—which are generally oral—are toxic to the patient; (3) TB is a common cause of death among HIV-positive patients; [3]. Typical TB treatment follows a 6-month administration of a cocktail of four different antibiotics: rifampicin (RIF), isoniazid, pyrazinamide and ethambutol. Along with the lengthy treatment period, several side effects can occur, such as nausea, vomiting, weight loss, hepatotoxicity, adverse skin and gastrointestinal reactions and immune responses, for instance, in the case of RIF. In addition, RIF interacts with isoniazid, which is also a major anti-TB drug, leading to the corresponding insoluble hydrazine derivative (4) resistant strains, such as multi-drug resistant (MDR-TB) and extensively drug resistant (XDR-TB), to all major anti-TB drugs have been observed and (5) the average cost of 6 to 32 months of treatment against TB, MDR-TB and XDR-TB is ~17,000, ~150,000 and ~300,000 US dollars, respectively The main drugs used (not an exhaustive list) for the treatment of TB are as follows: (1) first-line agents: rifampicin (RIF), isoniazid (INH), pyrazinamide (PZA), ethambutol (ETB) and aminoglycosides; (2) bacteriostatic second-line drugs: P-amino salicylic acid, cyclomerize and other drugs such as clofazimine, amoxicillin, clarithromycin, rifabutin and thioacetazone Chemotherapy is currently the only option for the clinical management of TB patients, with cure rates of up to 95% when given correctly to those with drug-susceptible TB. However, the majority of anti-TB medicines have subpar pharmacokinetic characteristics, which frequently prevent them from performing to their full potential in clinical situations (6) Poor bioavailability due to variable drug absorption and unwanted first-pass metabolism, lengthy regimens with high dosing frequencies, and individual and combined drug toxicity as well as severe adverse effects are some of the issues related to the therapeutic limitations of the current anti-TB regimens. These challenges contribute to low patient adherence, therapeutic failure, and the alarming emergence of multidrug-resistant (MDR) strains, all of which explain TB’s current lethal state and the pressing need to advance anti-TB treatment .(7)Advanced drug delivery systems require the development of a nanotechnological technique, which is a rapidly evolving cutting-edge scientific field that includes a wide range of disciplines such as chemistry, physics, and biology as well as special nanodimension structures with therapeutic applications in pharmacology and the biomedical field [8]. Many researchers are interested in the development and standardization of nanocarriers for various reasons, such as reduction in drug doses, minimal adverse effects, solubility and bioavailability improvement of drugs, targeted drug delivery resulting in improved patient compliance, and acceleration in recovery of patients [9]. These nanocarriers include solid lipid nanoparticles, nanostructured lipid carriers, liposomes, nano-emulsion, nanosuspension, nanoparticles, polymeric micelles, and dendrimers [10]. The nanocarriers appear to be a viable and intriguing approach to solve the limitations associated with conventional treatment associated with TB (11) Besides the above-mentioned treatment, vaccination is also another option for prevention of TB [18]. The WHO advises that, despite the Bacilli Calmette–Guerin (BCG) vaccine’s success in preventing TB and reducing mortality among infants and young children who have received vaccinations since birth, it is important to take into account the vaccine’s capacity to produce “trained immunity” by causing non-specific immune sensitization to other pathogens [12]. Additionally, it might aid in lowering the prevalence of infectious diseases, such as malaria, that are resistant to antimicrobials. Several benefits, including the large surface area of the sub-micron-sized particles, increased interaction of the vaccine with the large surface area of the respiratory mucosa and enhanced penetration into bacilli-loaded granulomas attributed to nanotechnology-based approaches, may particularly benefit in targeting the most common respiratory forms of TB against which BCG appears to be ineffective [13]. Previous research has shown the ability of the antigens implanted on nano-particulate platforms to improve immune response to other pathogens causing other infectious diseases, indicating the possibility of TB vaccines having the same capability once created [21].
Conventional Treatment Options and Its Limitations:
The current vaccination used to prevent TB is called Mycobacterium bovis bacillus Calmette–Guérin (BCG), and it was first given out in 1921 [14]. The BCG vaccine protects against TB in children between 60 and 80 percent of the time, but it is ineffective against pulmonary TB in adults [15]. Instead of the BCG vaccine, which is only effective in children, the WHO advises pharmacological therapies for TB in adults; their efficacy has also been reported to differ geographically [16]. Furthermore, because BCG is a live vaccine, those with impaired immune systems may acquire a disseminated infection. There is a pressing need to create new vaccines due to these limitations [17] In most countries, some drug-susceptible TB is treated with an oral medication regimen. This treatment plan consists of two months of daily or three-times-per-week administration followed by four months of isoniazid and rifampicin [18] of ethambutol (E), isoniazid (H), pyrazinamide (Z), rifampicin (R), and HRZE [19]. Treatment regimens have become increasingly complex due to the rise in TB complications, namely MDR strains, extensively drug-resistant (XDR) strains, HIV co-infection, the presence of comorbidities such as diabetes, and TB retreatment after recurrence. Drug-resistant TB may be treated by prolonging the course of treatment with drugs that the organism is susceptible to for up to 20 months or by adding an injectable antibiotic such as kanamycin, amikacin, or streptomycin [20]. The progression of anti-TB medications that have been authorized and are used for treatment of TB has been depicted in the Figure 2. The following are the primary medications (not a complete list) used to treat TB: First-line medications include rifampicin, isoniazid, pyrazinamide, ethambutol, and aminoglycosides. Second-line medications for bacteriostatic infections include P-aminosalicylic acid, cycloserine, and other medications including clofazimine, marnicillin, clarithromycin, rifabutin, and thioacetazone (Figure 1). These medications are typically generic [5]. Without a question, TB continues to be a serious. Globel health issue, and novel medicines are urgently required to address the drug resistance situation in TB. In order to do this, a number of novel bicyclic nitroimidazoles without mutagenic properties were created, including OPC-67683 (delamanid, Otsuka Pharmaceuticals) and PA-824 (pretonamid, PathoGenesis) (Figure 2). Pretonamid (Figure 2) is presently being tested in Phase II/III clinical studies for the treatment of TB, whereas delamanid (Figure) 1) was licenced by the European Medicines Agency (EMA) in 2014 for the treatment of pulmonary multidrug-resistant TB in adult patients [6,7]. TBA-6354 was recently moved to Phase 1 by the Global Alliance for TB Drug Development and the University of Auckland, although the medication demonstrated neurotoxicity in healthy volunteers [8,9]. The FDA gave SirturoTM (bedaquiline, TMC-2017), a derivative of the diarylquinonoline, expedited approval in 2012 for the treatment of multidrug-resistant tuberculosis in adults. It is the first brand-new anti-TB medication to be licenced since Rifapentine in 1998 [10]. The combination of this medicine with other medications, such as Delamanid for the treatment of patients with pulmonary extensively drug-resistant tuberculosis, was the first to be developed expressly for the treatment of multidrug-resistant tuberculosis [11] Nanotechnology is an interdisciplinary field that includes the creation of nanodevices as well as research in chemistry, materials, biology, physics, diagnosis, and engineering. Throughout the R&D process, the pharmaceutical business uses nanotechnology [12]. Thus, the development of various nanodevices such as liposomes, nanocrystals, nanoparticles, and dendrimers has significantly impacted the delivery of therapeutic drugs and diagnostics using nanoformulations and nanocarriers. These nanodelivery platforms can increase the solubility and, consequently, the bioavailability and pharmacokinetic/ pharmacodynamic (PK/PD) ratio of carried drugs, such as small molecules, macrocycles, and peptides. They can also decrease therapeutic dosage by increasing the drug exposure level over an extended period of time, and they can minimise off-target effects (adverse side effects). In comparison to, say, medication combinations, the introduction of nanoparticles can These medicinal substances can be complexed on the surface of nanoparticles, conjugated to them, or enclosed within nanoparticles. Vaccines and genes can both be transmitted. The development of tailored nanoparticles to transport therapeutic compounds to the appropriate organs (such as the brain, kidney, and lung), cells (such as tumour cells), and inside cell compartments (such as the nucleus, mitochondria, and cytoplasm) has also received a lot of attention [14], Choi has put forth the "Choi criterion," or a comprehensive viewpoint of the modulation of a number of physicochemical properties [15]. Nanoparticle composition controls biodegradation and toxicity, surface characteristics influence targeting and biodistribution, and size and shape Along with polymeric micelles, linear polymers, and polymeric, metal-hased nanoparticles, dendrimer and dendron nanostructures are excellent delivery systems and hold great promise for the future of nanomedicine [16]. A family of nanosized macromolecules known dendrimers from the Greek words “dendros” and “meros” are distinguished by their compact, spherical geometry in solution and highly homostructural, branched three-dimensional (3D) architectureDendrimera are globular macromolecules that have a highly branching 3D architecture and can have exquisite control over their size and structure. They exhibit a central core that is surrounded by an exponential number of dendritic branches with hydrophobic and hydrophilic moieties. With each generation, the number of surface groups grows exponentially while the dendrimer diameter increases. linearly. Dendrimers of lower generation are typically flexible, but those of higher generation neration ure denser and more rigid [17],

Fig no: -02
The currently available drugs for treatment of TB are distributed throughout the body via systemic blood circulation after being ingested or administered intravenously, and many molecules aggregate in other body regions rather than reaching the intended site, leading to adverse effects such as nephrotoxicity, hepatotoxicity, ocular toxicity, and ototoxicity. The majority of anti-TB medications are taken orally, which causes pharmacokinetic problems such as reduced bioavailability and a low therapeutic index [21]. Drug therapy used in the traditional manner requires a protracted therapy regimen that involves the continuous and frequent administration of several medications, which lowers patient adherence to current therapies. This is a crucial marker of infection recurrence, as well as the development of both the more serious XDR-TB and MDR-TB [21] In addition, patients are less likely to adhere to existing medications as a result of time duration concerns in conventional pharmacological therapies, which accounts for infectious recurrence and the emergence of MDR and XDR-TB. MDR-TB is a growing problem for the healthcare sector in developing countries [23]. Although current anti-TB therapies are effective, it is urgently necessary to develop new short-course regimens with additional drugs to address the various challenges associated with drug and target selection as well as patient commitment. Additionally, contemporary strategies such as nanoparticles, liposomes, dendrimers, etc. Must be developed to address the conventional therapeutic challenges. Sense
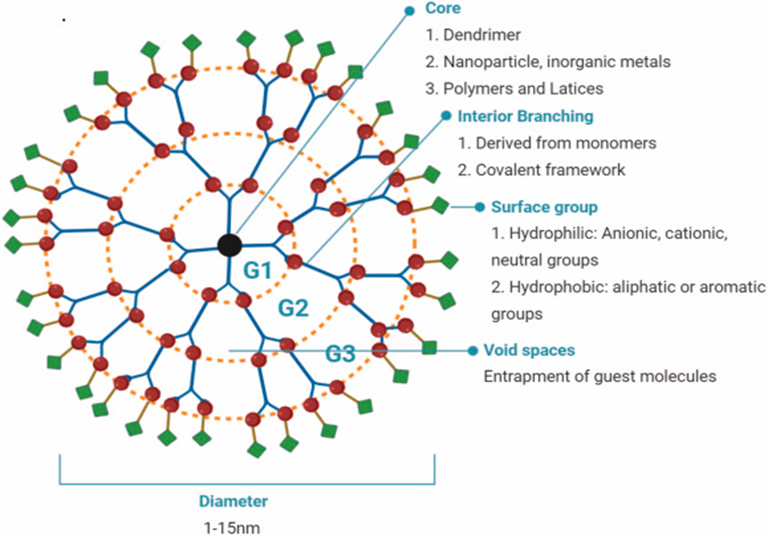
Fig no: -03
In TB Therapy:
Suitable for encapsulating or conjugating anti-TB drugs such as:
Dendrimers that include anti-TB drug encapsulation the creation of mannosylated dendritic structures (GS EDA-PPI dendrimers) for the targeted delivery of RIF to alveolar macrophages was first studied by Palanirajan Vijayaraj Kumar and colleagues [23]. A fifth-generation poly(propyleneimine) (PPI) dendrimer with an ethylene diamine (EDA) core and about 30 D-mannose groups grafted on the surface is known as the mannosylated GS EDA-PPI dendrimer (Figure 4). As seen in Figure 1, RIF in a crucial part of the mixture of anti-TB combination medications. The inhibition of the bacterial RNA polymerase component, which prevents gene transcription, is connected to the mechanism of action of RIF. It is noted that a number of RIF side effects are connected to the drug’s poor pharmacokinetic profile, primarily because of how poorly it dissolves in water. Additionally, RIF is degraded into the less soluble molecule 3-formyl-rifampicin in stomach circumstances (pH 4-5). Mannose was chosen because it is recognised by lectin receptors on the surface of phagocytic cells, which increases the uptake of medicines by immune system cells by nanocarriers containing mannose on their surfaces and in their void spaces. About 37 RIF have been integrated into PPI dendrimers using the widely used dissolving approach According to SEM analyses, the mannosylated dendrimers had an irregular form and a median diameter of less than 5 m. According to tests using differential scanning calorimetry, loaded mannosylated PPI dendrimers did not physically combine. A drop-in solubility was seen when RIF was enclosed in a mannosylated dendrimer (5 mg/mL), although this solubility level is still double that of the aqueous solubility of RIF alone. The nanodevice created by including RIF within the PPI dendrimer had a solubility of around 50 mg/ml. RIF and the mannosylated dendrimer were seen to interact non-covalently. We detected both hydrogen bonding and hydrophobic interactions (about 37%) with the core. The GS EDA-PPI mannosylated dendrimer’s hemolytic toxicity was assessed against red blood cells, with particular attention paid to the significant decrease in toxicity of the mannosylated versus non-mannosylated dendrimers (2.8% versus 15.6%), which was caused by the inhibition of the charged quaternary ammonium ion’s interaction with cells. Unmodified PPI dendrimers with all of their surface-bearing amino groups have a severe hemolytic toxicity, preventing clinical use. Similar modifications must be made to PAMAM dendrimers surfaces by adding groups that lessen their toxicity and cationic surface feature. At a concentration of 100 g’ml. Both mannosylated dendrimers and the mannosylated dendrimer loaded with RIF exhibited low eytotoxicity (85% viability). The group of RIF alone demonstrated a viability of 50% in the same assay at the same concentration. According to the authors, RIF stayed in the internal cavities of mannosylated dendrimers for a considerable amount of time (around 120 h) as opposed to about 10 h with the PPI dendrimer at physiological pH of 7.4. It’s significant to note that a large drug release rate was seen at pH 5, which mimics the pH of phagolysosomes. Alveolar macrophages (AM) from rat lungs clearly took up more RIF-loaded mannosylated PPI dendrimers (intracellular concentration) compared to RIF alone. It was found that the quantity of RIF absorbed into AM and the amount of RIF followed a fairly linear curve. For the transport of hydrophobic medicines like RIF in the TB domain, the mannosylated G5 EDA-PPI dendrimer thus constitutes a suitable nanocarrier system. The authors used 40 and SG PEGylated PPI dendrimers for the sustained delivery of RIF and described effects using the same methodology [24]. The capacity of 4G and SG PPI dendrimers to entrap drugs was significantly improved by grafting PEG chains onto their surfaces, going from 28% and 39% to 57% and 61% for G4 and G5 dendrimers, respectively. A cumulative release of 97.3% and 46.3% for G4 for G4 and G5 dendrimers, respectively, was achieved after 36 hours thanks to the addition of PEG chains, which further improved the control of RIF release. Additionally, PEGylated PPI Dendrimers and Non-PEGylated PPI Dendrimers with the same generations (14-20%) showed mild and severe hemolytic toxicitics, respectively (1-3%). Rifampicin (RIF), anti-tuberculosis medication, was linked to the G4-PAMAM dendrimer in investigations using molecular dynamics (MD) simulations [25]. It is well recognised that molecular dynamics (MD) modelling is an effective tool for researching several kinds of molecular systems, including association systems. This study demonstrated that 20 RIF molecules can be loaded to their maximal capacity per G4-PAMAM dendrimer experimentally. This discovery agrees with Kumar et alfindings, ‘s which highlighted the connection of up to 37 RIF molecules per mannosylated GS-PPI dendrimer (vide supra) Additionally, the scientists looked at the drug quantities of RIF and ibuprofen, a related substance that both fall under the FDA’s class II biopharmaceutical classification system (BCS), which is distinguished by high permeability and low solubility [26]. The highest number of ibuprofen molecules that can fit inside a dendrimer is 78, which is roughly four times more than RIF can fit inside a G4 PAMAM dendrimer. It’s crucial to remember that RIF has a molecular weight that is almost four times greater than ibuprofen’s (MW 822 versus 206), and thus RIF is roughly four times larger than ibuprofen (1.086 versus 0.276 nm3). Molecular dynamic sinulations at neutral and low pH were produced based on the docking of RIF molecules within the G4 PAMAM cavities (20 RIF molecules per dendrimer measured experimentally, see supra). At a pH of 7, the complex was found to be quite stable, but at a pH of 4, RIF molecules were swiftly and simultaneously ejected into the solvent bulk. This finding highlights the potential of PAMAM dendrimers as nanocarriers for drug delivery in alveolar macrophages and other acidic cellular structures. Recently, RIF loaded PEGylated 5G EDA-PAMAM dendrimers were addressed by P. Dinesh Kumar and colleagues [27]. (Figure 5). The PEGylation of 5G PAMAM dendrimers was verified by 1H-NMR spectra and the Fourier Transform Infrared Spectrophotometry (FTIR) method. It was discovered that the PEGylated Dendrimer’s RIF entrapment efficiency was 99%. For PEGylated (in 120 h) and non-PEGylated (in 72 h) PAMAM dendrimers, respectively, the drug release rate of RIF is 81% and 98% Due to the inhibition of red blood cell interaction with quaternary ammonium groups on the surface of dendrimers, hemolytic studies revealed that non-PEGylated PAMAM dendrimer revealed 11.6 to 25.3% of toxicity, whereas the PEGylated PAMAM dendrimer strongly showed lower toxicity effects (less than 2.5%). Early investigations using dendrimers with cationic groups on their surface indicated similar results. Interesting pharmacokinetic (PK) features of PEGylated SG EDA-PAMAM dendrimers loaded RIF versus RIF alone were discovered in vivo experiments carried out in Wistar albino rats [27]. The PK profile of 5G EDA-PAMAM dendrimers loaded with RIF and RIF is shown in Table 1. (0.5-120 h). RIF stopped being present in plasma after 6 hours, while it persisted in SG EDA-PAMAM dendrimers for 120 hours. In comparison to free RIF, PEGylated 5G EDA-PAMAM dendrimers loaded with RIF showed lower and longer plasma drug concentration-time curve (AUC), half-life (t1/2), and mean residence time (MRT) values. After three months (40 °C) of storage, no changes were seen in the 5G EDA-PAMAM dendrimers loaded with RIF, either in appearance or in RIF release. Introduction and State-of-the-Art in the Development of Nano-Based Drug Delivery of Anti-TB Drugs Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis, also known as Koch bacillus, surviving and replicating within human alveolar macrophages and affecting other organs [1,2]. A global view of this disease can be summarized as follows: (1) according to the latest report of the World Health Organization (WHO), more than one third of the world’s population is infected with Mycobacterium tuberculosis, and approximately 2 million deaths by TB were reported in 2017; (2) current treatments—which are generally oral—are toxic to the patient; (3) TB is a common cause of death among HIV-positive patients; (4) resistant strains, such as multi-drug resistant (MDR-TB) and extensively drug resistant (XDR-TB), to all major anti-TB drugs have been observed and (5) the average cost of 6 to 32 months of treatment against TB, MDR-TB and XDR-TB is ~17,000, ~150,000 and ~300,000 US dollars, respectively [3]. Typical TB treatment follows a 6-month administration of a cocktail of four different antibiotics: rifampicin (RIF), isoniazid, pyrazinamide and ethambutol. Along with the lengthy treatment period, several side effects can occur, such as nausea, vomiting, weight loss, hepatotoxicity, adverse skin and gastrointestinal reactions and immune responses, for instance, in the case of RIF. In addition, RIF interacts with isoniazid, which is also a major anti-TB drug, leading to the corresponding insoluble hydrazine derivative [4]. The main drugs used (not an exhaustive list) for the treatment of TB are as follows: (1) first-line agents: rifampicin (RIF), isoniazid (INH), pyrazinamide (PZA), ethambutol (ETB) and aminoglycosides; (2) bacteriostatic second-line drugs: P-aminosalicylic acid, cycloserine and other drugs such as clofazimine, amoxicillin, clarithromycin, rifabutin and thioacetazone (Figure 1). Many of these drugs are generics [5]. Introduction and State-of-the-Art in the Development of Nano-Based Drug Delivery of Anti-TB Drugs Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis, also known as Koch bacillus, surviving and replicating within human alveolar macrophages and affecting other organs [1,2]. A global view of this disease can be summarized as follows: (1) according to the latest report of the World Health Organization (WHO), more than one third of the world’s population is infected with Mycobacterium tuberculosis, and approximately 2 million deaths by TB were reported in 2017;
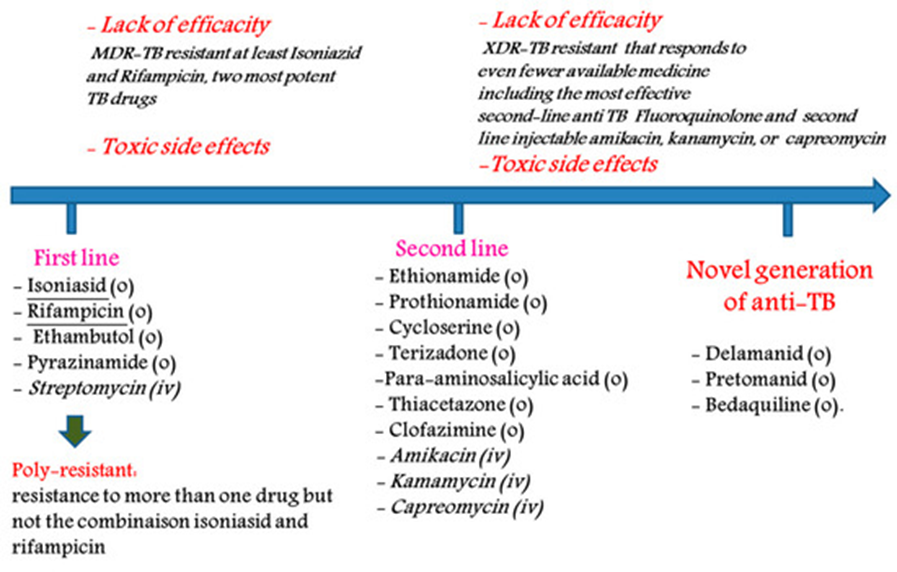
Figure 04. Main treatments to tackle tuberculosis (o: oral, iv: intravenous administration).
There is no doubt that TB remains a major global health problem, and new treatments to combat the crisis of drug resistance in TB are urgently needed. To this end, several new bicyclic nitroimidazoles without mutagenic effects were developed, such as OPC-67683 (delamanid, Otsuka Pharmaceuticals) and PA-824 (pretonamid, PathoGenesis) (Figure 5). Delamanid was approved by the European Medicines Agency (EMA) in 2014 for pulmonary multi drug-resistant TB in adult patients [6,7], whereas pretonamid (Figure 5) is currently in Phase II/III clinical trials for the treatment of TB. Recently, the Global Alliance for TB drug development and the University of Auckland advanced TBA-6354 to Phase I, but the drug showed neurotoxicity in healthy volunteers [8,9]. In 2012, the FDA granted accelerated approval to the diarylquinonoline derivative, SirturoTM (bedaquiline, TMC-2017) for treatment in adults of multidrug-resistant tuberculosis. It is the first new anti-TB drug to be approved after 1998 (Rifapentine) [10]. This drug was the first to be introduced specifically for the treatment of multidrug-resistant tuberculosis in combination with other drugs such as Delamanid combination for the treatment of patients with pulmonary extensively drug-resistant tuberculosis [11].

Figure 05. Chemical structures of Rifampicin (RIF), Isoniazid (INH), Delamanid, and Pretonamid.
Nanotechnology represents a multidisciplinary field encompassing various domains such as chemistry, materials, biology, physics, diagnosis and engineering, including the synthesis of nanodevices. The pharmaceutical industry adopts nanotechnology throughout the R&D process [12]. Thus, nanoformulations and nanocarriers have made a significant impact on the delivery of therapeutic agents and diagnostics through the development of several nanodevices such as liposomes, nanocrystals, nanoparticles and dendrimers. These nanodelivery platforms can improve the solubility and, consequently, the bioavailability and pharmacokinetic/ pharmacodynamic (PK/PD) ratio, reduce the therapeutic dosage (by increasing the drug exposure level over a long period of time) and minimize off-target effects (adverse side effects) of carried drugs such as small molecules, macrocycles and peptides. Finally, the use of nanoparticles can simplify the treatment versus, for example, drug combinations [13]. These therapeutic agents can be encapsulated within nanoparticles, conjugated to them or complexed on their surface. Genes and vaccines can also be carried. In addition, many efforts have been devoted to developing targeted nanoparticles to deliver therapeutic agents to the right tissues (e.g., brain, kidney, lung), cells (e.g., tumor cells) and inside cell compartments (e.g., nucleus, mitochondria, cytosol) [14]. A global view of the modulation of several physicochemical properties has been proposed by Choi, named ‘Choi criteria’ [15]. Composition of the nanoparticles manage their biodegradation and toxicity effects, surface properties control their targeting and biodistribution properties, whereas size and shape govern their excretion and clearance profiles. Besides polymeric, metal-based nanoparticles, polymeric micelles and linear polymers, dendrimer and dendron nanostructures represent ideal delivery vehicles and offer high hopes for the future of nanomedicine [16]. Dendrimers (from the Greek words “dendros” and “meros”) are a family of nanosized macromolecules characterized by a highly homostructural, branched three-dimensional (3D) architecture and compact, spherical geometry in solution. Dendrimers represent globular macromolecules, with a highly branched 3D architecture, whose shape and size can be precisely controlled. They display an exponential number of dendritic branches (hydrophobic and hydrophilic moieties) radiating from a central core. The dendrimer diameter increases linearly, while the number of surface groups increases exponentially with each generation. Low-generation dendrimers are usually flexible, while higher generation compounds are denser and increasingly rigid [17]. A schematic of a typical dendritic structure for biomedical applications is illustrated in Figure 6.
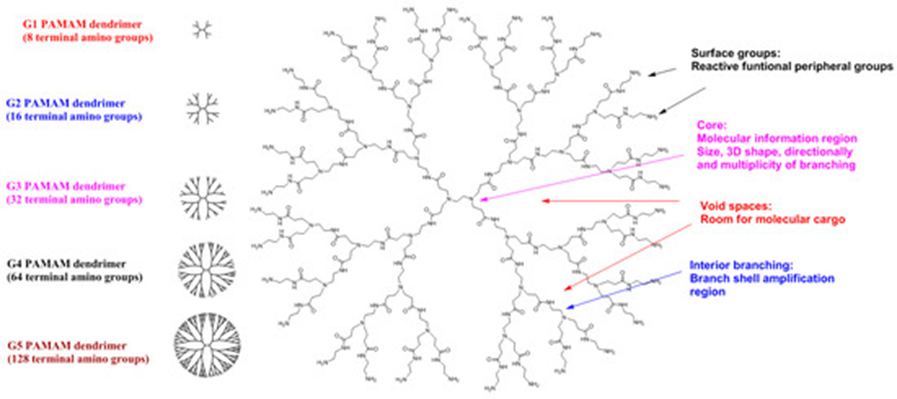
Figure 06. Schematic 2D representation of G3 PAMAM dendrimer as a typical dendritic structure
The dendritic macromolecular structure can be divided into four main components: (a) a central core moiety; (b) interior layers (generations, Gn, where n is 0, 0.5, 1, 1.5, …) made of regularly repeating branching units attached to the core; (c) terminal functionalities distributed in a 3D space; (d) void spaces, which are rooms for molecular cargo, such as anti-cancer agents [18]. The main dendrimer types used are PAMAM dendrimers (Starbust®), poly-etherhydroxyl-amine (PEHAM) dendrimers (Priostar®), PPI dendrimers (Astramol®) carbosilane dendrimers, and phosphorus-based dendrimers developed by J-P. Majoral and A-M. Caminade [19]. In 2012, Starpharma initiated two pivotal Phase III trials for the treatment of bacterial vaginosis with VivaGel® (SPL7013 Gel) [20]. This active polyanionic G4-poly(l-lysine)-type dendrimer has 32 naphthalene disulphonate groups on the surface and showed potent topical vaginal microbicidal activity. Starpharma has now received Food and Drug Administration Phase III approval. Starpharma/AstraZeneca has recently advanced from Phase I to Phase II with a poly(lysine)-dendrimer-based nanocarrier encapsulating docetaxel (DEP® docetaxel), which shows superior anticancer activity against several solid cancer types, including breast, prostate, lung and ovarian tumors [21]. With the aim of improving the bioavailability of anti-TB drugs in general and RIF in particular, several studies have been developed using drug delivery system approaches (nanoformulations) such as (1) nanodispersions including nanosuspensions, nanoemulsions, solid dispersions and niosomes; (2) polymeric and non-polymeric nanoparticles; (3) polymeric micelles and analogues and (4) liposomes and dendrimers (vide infra). The main anti-TB drugs carried by liposomes are streptomycin, gentamycin, sparfloxacin, amikacin, clofazimine, INH, RIF, PZA, rifabutin (RFB) and capreomycin; by niosomes, RIF and by nanoparticles and microparticles, INH, RIF, PYZ, ETB, streptomycin, moxifloxacin, PZA, ETB and econazole [22]. In this original review, we present and analyze the development of anti-TB drugs in combination with dendrimers. To our knowledge, there have been few articles featuring this nanoformulation. Importantly, similar to the development of nanocarriers in the oncology domain, lodging of M. Tuberculosis strains in the phagosome compartment of macrophages with an acidic pH (~4.5) allows the strategy of developing nanocarriers, such as tunable dendrimers, as a pH-based vectorization system that retains the anti-TB drugs in the blood (pH 7.4) and effectively release them in an acidic environment. Due to their unique structure and diverse route of administration, dendrimers represent attractive candidates for the encapsulation and conjugation of anti-TB drugs presenting important drawbacks (e.g., solubility, toxicity, low bioavailability) that hinder their development, including clinic trials.
2. Encapsulation of Anti-TB Drugs within Dendrimers
Early studies were performed by Palanirajan Vijayaraj Kumar and co-workers on the development of mannosylated dendritic architectures (G5 EDA-PPI dendrimers) for the selective delivery of RIF to alveolar macrophages [23]. The mannosylated G5 EDA-PPI dendrimer is a fifth-generation poly(propyleneimine) (PPI, 64 amino groups on the surface) dendrimer with an ethylene diamine (EDA) core and grafted on the surface with ~30 D-mannose groups (Figure 7). RIF is an essential component of the cocktail of anti-TB combination drugs, as shown in Figure 1. The mechanism of action of RIF is related to the inhibition of the subunit of the bacterial RNA polymerase, which inhibits gene transcription. It is emphasized that several side effects of RIF are related to its poor pharmacokinetic profile, mainly due to its low solubility in water. In addition, under gastric conditions (pH 4–5), RIF is hydrolyzed into the less soluble compound 3-formyl-rifampicin. Mannose was selected because this sugar molecule is recognizable by lectin receptors on the surface of phagocytic cells and consequently improves the uptake of nanocarriers bearing mannose on their surface and drugs in their void spaces by the cells of the immune system.

Figure 07. Schematic 2D of mannosylated G5 EDA-PPI dendrimer and RIF Me.
Using the very well-known dissolution technique, about 37 RIF have been incorporated into PPI dendrimers. SEM studies showed an irregular shape and agglomerated mannosylated dendrimers with a median diameter less than 5 μm. Differential scanning calorimetry studies suggested that loaded mannosylated PPI dendrimers did not form a physical mixture. The solubility of the nanodevice obtained by the incorporation of RIF within the PPI dendrimer is ~50 mg/mL, while a decrease in solubility was observed when RIF was encapsulated in a mannosylated dendrimer (~5 mg/mL), but this solubility level is twice that of the aqueous solubility of RIF alone. Non-covalent interactions between RIF and the mannosylated dendrimer were observed. Both hydrogen bonding and hydrophobic interactions (~37%) with the core were observed. Hemolytic toxicity of the G5 EDA-PPI mannosylated dendrimer was evaluated against red blood cells emphasizing the significant decrease in toxicity of mannosylated versus non-mannosylated dendrimers (2.8% versus 15.6%) due to inhibition of the interaction of the charged quaternary ammonium ion with cells. The high hemolytic toxicity of unmodified PPI dendrimers, with all the surface bearing amino groups, precludes their clinical applications. Similarly, PAMAM dendrimers must be modified on their surface by the introduction of groups that decrease the cationic surface aspect and, consequently, toxicity. Mannosylated dendrimers displayed negligible cytotoxicity against Vero cells at a concentration of 100 μg/mL, as did the RIF-loaded mannosylated dendrimer (~85% viability). In the same assay, the group of RIF alone showed a viability of ~50% at the same concentration. The authors mentioned that RIF remained for a long duration (~120 h) in the interior cavities of mannosylated dendrimers at physiological pH of 7.4 versus <10 h with the PPI dendrimer. Importantly, a high drug release rate was observed at pH 5, which simulates the pH of phagolysosomes. A clear increase (intracellular concentration) in the cellular uptake of RIF-loaded mannosylated PPI dendrimers by alveolar macrophages (AM) from rat lungs versus RIF alone was observed. A quite linear curve amount of RIF incorporated in AM versus the amount of RIF was observed. Consequently, the mannosylated G5 EDA-PPI dendrimer represents a good nanocarrier system for the delivery of hydrophobic drugs such as RIF in the tuberculosis domain. Using the same approach, the authors described similar effects using 4G and 5G PEGylated PPI dendrimers for the sustained delivery of RIF [24]. The grafting of the PEG chains on the surface of 4G and 5G PPI dendrimers strongly increased their drug entrapment capability from 28% and 39% to 57% and 61% for G4 and G5 dendrimers, respectively. Also, the introduction of PEG chains improved the control of release of RIF after 36 h, with a cumulative release of 97.3% and 46.3% for G4 and G5 dendrimers, respectively. In addition, low and high hemolytic toxicities were observed (1–3%) for PEGylated PPI dendrimers and non-pegylated PPI dendrimers, respectively, with the same generations (14–20%). Bellini and co-workers described molecular dynamics (MD) simulation studies of the association of the anti-tuberculosis drug rifampicin (RIF) with the G4-PAMAM dendrimer [25]. It is well known that molecular dynamics (MD) simulation represents a powerful tool to study several types of molecular systems, such as association systems. This study showed that, experimentally, the maximum number of RIF molecules loaded is 20 RIF molecules per G4-PAMAM dendrimer. This result is concordant with the work of Kumar et al. Emphasizing the association of a maximum of ~37 RIF molecules per mannosylated G5-PPI dendrimer (vide supra). In addition, the authors studied the drugs occupied volumes of RIF and that of a similar compound ibuprofen, which together belong to the class II biopharmaceutical classification system (BCS) as defined by the FDA, which is characterized by low solubility and high permeability [26]. The maximum number of ibuprofen molecules is 78 per dendrimer, approximately four times higher than the number of RIF per G4 PAMAM dendrimer. It is important to note that the molecular weight of RIF is approximately four times higher than that of ibuprofen (MW 822 versus 206), and RIF is approximately four times larger than ibuprofen (1.086 versus 0.276 nm3). Based on the docking of RIF molecules within the G4 PAMAM cavities (20 RIF molecules per dendrimer determined experimentally, vide supra), molecular dynamic simulations were generated at neutral and low pH. Reasonable stability of the complex at neutral pH was observed, whereas at low pH, RIF molecules were rapidly and simultaneously expelled to the solvent bulk. This result underlines the potential role of PAMAM dendrimers as nanocarriers to deliver drugs in acidic cellular structures such as alveolar macrophages. Recently, P. Dineshkumar and co-workers emphasized the development of RIF loaded PEGylated 5G EDA-PAMAM dendrimers [27] (Figure 5). The PEGylation of 5G PAMAM dendrimers was confirmed by Fourier Transform Infrared Spectrophotometry (FTIR) technique, and 1H-NMR spectra. The RIF entrapment efficiency in PEGylated dendrimer was found to be ~99%. The drug release rate of RIF is 81% and 98% for PEGylated (in 120 h) and non-PEGylated (in 72 h) PAMAM dendrimers, respectively. The hemolytic studies showed that non-PEGylated PAMAM dendrimer revealed 11.6 to 25.3% of toxicity, whereas the PEGylated PAMAM dendrimer strongly showed lower toxicity effects (less than 2.5%) due to the inhibition of interaction of red blood cells with quaternary ammonium groups on the surface of dendrimers. Similar effects were highlighted in early studies with dendrimers bearing cationic groups on their surface [28].

Figure 08. PEGylated 5G EDA-PAMAM dendrimers and RIF.
Interestingly, in vivo studies were performed in Wistar albino rats, and revealed interesting pharmacokinetic (PK) parameters of PEGylated 5G EDA-PAMAM dendrimers loaded RIF versus RIF alone [29]. Table 1 highlights the PK profile of 5G EDA-PAMAM dendrimers loaded RIF and RIF (0.5–120 h). After 6 h there was no presence of RIF in plasma, whereas in 5G EDA-PAMAM dendrimers, RIF remained for 120 h. Low and prolonged release of RIF were observed inducing higher area under the plasma drug concentration-time curve (AUC), half-life (t1/2) and mean residence time (MRT) values for PEGylated 5G EDA-PAMAM dendrimers loaded RIF versus free RIF. No change either in appearance or in RIF release from 5G EDA-PAMAM dendrimers loaded with RIF were observed after 3 months (~40 °C) storage.
Table 1. Pharmacokinetic (PK) profile of 5G EDA-PAMAM dendrimers loaded rifampicin (RIF) and RIF.

Another very important anti-TB drug has been also loaded with dendrimers, isoniazid (IND) [28]. N. Singh et al. Described the loading of IND with 1.5G PAMAM dendrimer using dialysis method (Figure 8). UV spectroscopy and FTIR techniques confirmed the loading of IND. This formulation revealed that around 93.25% of IND was constantly released up to 24 h. In addition, drug release kinetic studies demonstrated that the kinetic is zero order corresponding to a non-Fickian diffusion probably due to the sharp boundary separating the void spaces, where IND is encapsulated, and the surface of the dendrimer [30].
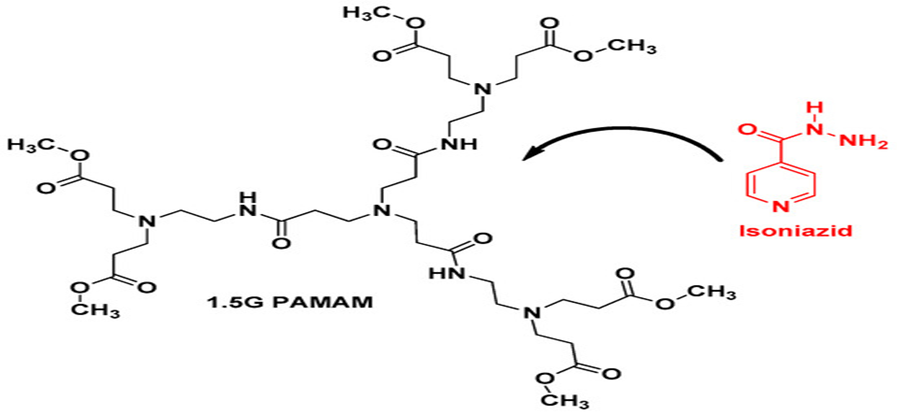
Figure 09. Chemical structure of 1.5G PAMAM dendrimer and Isoniazid (IND).
The chronic pulmonary infectious disease TB is the second most deadly infectious disease, causing approximately 2 million deaths per year. Despite curative treatments that have been available for over 50 years, the treatment is complex and lasts for up to 9 months. Unfortunately, anti-TB drugs revealed side effects and adverse events associated with medications inducing, for instance, a change in the dosage of drugs, discontinuation of treatment and additional treatment. Several complications increased morbidity and mortality. Very importantly, to increase treatment efficacy, including avoiding resistance (MDR-TB and XDR-TB), it is necessary to utilize multidrug regimens, which have also been associated with an increased incidence of side effects. Consequently, the risks of treatment failure and relapses are higher. Clearly, monitoring treatment and developing new strategies will be crucial to decreasing the cost of treatment and the incidence of serious drug-related adverse effects. In this direction, the development of effective nanotechnology represents a very important domain in the TB field. Several techniques, such as nanodispersions, polymeric nanoparticles, polymeric micelles, liposomes and dendrimers, have been used. Dendrimers have a polymeric architecture with tunable defined structures and represent versatile drug delivery systems. Thus, in the dendrimer domain, few articles have highlighted the encapsulation of anti-TB drugs such as RIF (vide supra). No conjugation of anti-TB drugs was described to date. Extensive application of dendrimers as nano carriers has been described essentially in the oncology domain. We believe strongly that a new avenue has appeared in the development of biocompatible dendrimers as nanocarriers in the TB domain. Dendrimers can potentially entrap and/or conjugate high-molecular-weight hydrophilic/ hydrophobic chemical entities or a combination of chemical entities, which generally suffer from various limitations like low aqueous solubility and short half-lives, by host-guest interactions and covalent bonding (a prodrug approach), respectively. Consequently, it is necessary to design new biodegradable, biocompatible, water-soluble and nontoxic dendrimers which can deliver a drug or a mixture of drugs, such as anti-TB drugs, efficiently through an endocytosis process to improve treatment efficacy and, consequently, patient compliance. One other advantage of dendrimers is their use in both therapeutic and diagnostic applications, and they represent a new generation of nanoparticle-based therapies. Regarding the toxicity of dendrimers, in vitro and in vivo studies are crucial to evaluating cell viability, hematological toxicity, immunogenicity, biocompatibility and biodistribution, to establish risk/benefit ratios and to assure their clinical development. Importantly, Good Manufacturing Practice (cGMP) requirements are indispensable for Investigational New Drug approval, to ensure the quality, reproducibility and reliability of in vitro and in vivo data and to secure successful development. The successful translation from research to the clinic should be performed by the development of such biocompatible dendrimers to jump the ‘valley of death’ successfully. To this end, several of us (S.M., J.-P.M., X.S.) recently proposed a simple set of guidelines to move towards an Investigational New Drug application [31].
Dendrimers can act as nanocarriers to deliver anti-TB drugs more effectively.
Key Advantages:
Improved solubility of poorly soluble TB drugs (e.g., rifampicin, isoniazid). Controlled and sustained release of drugs. Targeted delivery to infected macrophages (where Mycobacterium tuberculosis resides). Reduced toxicity and side effects by minimizing systemic drug exposure.
Examples:
PAMAM dendrimers (polyamidoamine) have been used to encapsulate rifampicin and enhance its bioavailability and cellular uptake.
PLGA-dendrimer hybrids show promise in controlled release formulations for TB treatment.
Controlled and targeted delivery reduces the likelihood of sub-therapeutic drug levels, a major factor in the development of multidrug-resistant TB (MDR-TB). Co-delivery of multiple drugs in one dendrimer system ensures synchronized delivery, helping prevent resistance.
Dendrimers can deliver small interfering RNA (siRNA) or DNA to downregulate TB-related host genes or modulate immune responses. This can potentially enhance the host immune system to better combat TB infection.
Dendrimers can be engineered to act as vaccine adjuvants or carriers for TB antigens, boosting the immune response. This may aid in therapeutic vaccination or immune-boosting strategies in TB therapy.
Dendrimers tagged with imaging agents can help in diagnostic imaging to locate TB lesions. This supports theranostic approaches — combining therapy and diagnosis.
Monodispersity: Dendrimers have a well-defined, branched, tree-like architecture with uniform size and shape.
Predictable Functionality: The surface and core can be precisely modified to tailor their behavior for specific drug delivery purposes.
Multivalent Surface: The high number of terminal functional groups allows for multiple drug molecules or targeting ligands to be attached.
Encapsulation Ability: Hydrophobic or hydrophilic drugs can be encapsulated in the internal cavities, improving solubility and stability.
Dendrimers enhance the solubility of poorly water-soluble drugs, thus improving their bioavailability and therapeutic efficacy.
Functionalization of dendrimers allows for stimuli-responsive release (pH, temperature, enzymes). Targeting ligands (e.g., antibodies, peptides) can be added for site-specific delivery, reducing off-target effects.
Targeted delivery and controlled release reduce the required dosage and exposure of non-target tissues, minimizing side effects.
Surface groups (like amines, carboxyls, hydroxyls) can be chemically modified to adjust biocompatibility, circulation time, or target specificity.
Certain generations and types of dendrimers (e.g., PEGylated or polyester-based) are biocompatible and biodegradable, making them suitable for in vivo use.
Dendrimers can be conjugated with imaging agents (e.g., MRI contrast agents) for diagnostics. Can be used in theragnostic, combining therapy and diagnostics in one platform.
Challenges of Dendrimers in Nanocarriers
Issue: Positively charged dendrimers (e.g., PAMAM) can interact with cell membranes, causing cytotoxicity.
Effect: Limits clinical application due to potential damage to healthy cells and tissues.
Issue: Cationic dendrimers can disrupt red blood cells, leading to hemolysis.
Effect: Incompatible with intravenous drug delivery without modification.
Issue: Smaller generations may have insufficient space for drug encapsulation.
Effect: Reduces therapeutic payload and efficacy.
Issue: Synthesis involves multiple, labour-intensive steps with purification challenges.
Effect: Increases cost and scalability problems for large-scale production.
Issue: Some dendrimers can trigger immune responses
Effect: Potential allergic reactions or reduced therapeutic efficiency.
Surface Charge Toxicity: Dendrimers, especially those with positively charged amine groups (e.g., PAMAM dendrimers), can be cytotoxic due to interactions with cell membranes.
Accumulation: Poor biodegradability can lead to accumulation in tissues, raising concerns over long-term toxicity.
Hemolytic Activity: Some dendrimers can cause hemolysis, damaging red blood cells.
2. Complex and Costly Synthesis
Multistep Synthesis: Dendrimers require controlled, multi-step synthesis, increasing production time and complexity.
High Cost: The synthesis is labor-intensive and expensive, especially at high generations or for large-scale production.
3. Limited Drug Loading Capacity
Interior Space Constraints: The internal cavities of dendrimers may not accommodate large or hydrophobic drugs efficiently.
Burst Release: Some drug–dendrimer systems suffer from premature or uncontrolled drug release.
In Vivo Instability: Dendrimers may degrade or change structure in physiological environments.
Aggregation: Dendrimers can aggregate under certain conditions, reducing their effectiveness as nanocarriers.
Regulatory Hurdles: Due to their complex nature and lack of long-term toxicity data, gaining regulatory approval can be difficult.
Reproducibility: Achieving consistent batch-to-batch quality is challenging, affecting clinical translation.
Future Prospects of Dendrimers in TB Therapy
Ligand-functionalized dendrimers (e.g., mannose, folate, or antibodies) can selectively target macrophages, the primary host cells for Mycobacterium tuberculosis. This enhances therapeutic efficacy while reducing systemic toxicity.
Dendrimers can potentially co-deliver multiple anti-TB drugs (like isoniazid, rifampicin, pyrazinamide) in a single system.
This helps maintain drug synergy, reduce pill burden, and improve patient compliance.
Dendrimer-drug conjugates or encapsulations can enable long-acting release profiles, reducing dosing frequency and enhancing adherence, particularly important for TB’s lengthy treatment regimens.
Functionalized dendrimers may be used to target and bypass drug resistance mechanisms, such as efflux pumps or bacterial cell wall barriers. Their use can be extended to deliver new chemical entities or gene-editing tools targeting resistant strains.
Inhalable dendrimer formulations (e.g., aerosols, dry powders) could deliver drugs directly to the lungs, the primary site of TB infection, offering high local concentration with fewer systemic side effects.
Key Research Directions: -
? Biodegradable and Less Toxic Dendrimers
? Stimuli-Responsive Dendrimers
? Gene Delivery for TB Vaccination or Therapy
Exploration of dendrimers as nucleic acid carriers for TB DNA vaccines, RNA interference, or CRISPR/Cas-based therapeutics.
? Nanohybrid Systems
Combining dendrimers with other nanomaterials (e.g., liposomes, nanoparticles, or carbon nanotubes) to enhance delivery, imaging, and therapy.
? In Vivo Studies and Clinical Translation
More extensive in vivo testing and toxicity studies are needed for preclinical validation. Development of scalable, reproducible synthesis protocols for clinical-grade dendrimer formulations.
CONCLUSION: -
Dendrimer-based nanocarriers represent a promising advancement in the fight against tuberculosis, particularly in addressing the limitations of conventional drug delivery systems. Their well-defined, highly branched architecture allows for efficient drug encapsulation, targeted delivery, and controlled release, which can enhance the bioavailability and therapeutic efficacy of anti-TB drugs. Moreover, dendrimers offer the potential to overcome drug resistance and reduce systemic toxicity, thereby improving treatment outcomes and patient adherence. Despite these advantages, further research is needed to fully understand their pharmacokinetics, long-term safety, and scalability for clinical use. As the global burden of tuberculosis persists, dendrimer nanocarriers hold significant potential to contribute to more effective and innovative TB treatment strategies. dendrimers, as nanocarriers, offer a promising approach to improve tuberculosis (TB) therapy by enhancing drug delivery, targeting, and efficacy. Their unique properties, such as high surface area, tailorable properties, and multivalent interactions, make them an attractive platform for developing novel TB treatments. By leveraging dendrimers, researchers can design targeted and controlled-release delivery systems that improve the therapeutic efficacy of anti-TB drugs, reduce side effects, and potentially shorten treatment durations. Further research and clinical trials are necessary to fully realize the potential of dendrimer-based TB therapies and bring them to the clinic.
REFERENCES

Prafulla Patil*, Dr. Shivshankar Mhaske, Pankaj Fitave, Dipak Sontakke, Om Lole, Akash Parihar, Vaibhav Chaudhary, Nanocarriers Dendrimers for New Tuberculosis Therapy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4659-4680. https://doi.org/10.5281/zenodo.15542547
 10.5281/zenodo.15542547
10.5281/zenodo.15542547
