
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
DrNB Neuroanesthesia, Freelance neuroanesthesiologist and neurointensivist, Bengaluru.
Neuroleptic Malignant Syndrome (NMS) is a rare but potentially life-threatening complication of antipsychotic medication. I present the case of a 67-year-old man who developed NMS following haloperidol administration for ICU delirium. The patient exhibited the classic tetrad of symptoms: altered mental status, muscle rigidity, hyperthermia, and autonomic instability, along with elevated creatine kinase indicating rhabdomyolysis. This case highlights the importance of careful antipsychotic use in critically ill patients, early recognition of NMS, and prompt intervention. I discuss the pathophysiology, diagnosis, and management of NMS in the context of neurocritical care, with particular emphasis on the risk-benefit assessment of antipsychotic use in delirium management.
Delirium affects up to 80% of patients in intensive care units (ICUs) and is associated with increased mortality, prolonged hospital stays, and long-term cognitive impairment[1,2]. Antipsychotics, particularly haloperidol, have historically been used for the symptomatic management of delirium despite limited evidence supporting their efficacy [3]. Neuroleptic Malignant Syndrome (NMS) represents a potentially fatal complication of antipsychotic therapy, with mortality rates estimated between 5-20%[4]. The syndrome is characterized by a tetrad of symptoms: altered mental status, muscle rigidity, hyperthermia, and autonomic instability. The reported incidence of NMS ranges from 0.02% to 3% among patients receiving antipsychotics[5]. In the critical care setting, diagnosing NMS presents unique challenges, as many features overlap with other common conditions in critically ill patients, including sepsis, malignant hyperthermia, and serotonin syndrome[6]. Here, I present a case of NMS following haloperidol administration for ICU delirium, highlighting the importance of judicious antipsychotic use and prompt recognition of this serious complication.
Case Presentation
Mr. X, a 67-year-old man with a medical history of hypertension, type 2 diabetes mellitus, and coronary artery disease, was admitted to the ICU following emergent decompressive craniectomy for a subdural hemorrhage. His post-operative course was complicated by respiratory failure requiring mechanical ventilation and vasopressor support for hemodynamic instability. On post-operative day 3, despite appropriate sedation adjustments and optimization of environmental factors, the patient developed signs of hyperactive delirium, including agitation, disorientation, and pulling at lines and tubes. His Confusion Assessment Method for the ICU (CAM-ICU) was positive. After non-pharmacological interventions proved insufficient, haloperidol 5 mg intravenously was administered, followed by a scheduled regimen of 2.5 mg every 6 hours. Within 48 hours of initiating haloperidol therapy, the nursing staff noted progressive muscle stiffness and a low-grade fever of 38.2°C (100.8°F). By the following morning, the patient's condition had deteriorated significantly. Clinical findings included:
Laboratory investigations revealed:
Computed tomography of the brain showed no acute intracranial pathology. Based on the clinical presentation, laboratory findings, and temporal relationship to haloperidol initiation, a diagnosis of NMS was made.
Management and Outcome
Haloperidol was immediately discontinued, and supportive care was initiated with the following measures:
The patient was monitored in the ICU with continuous electrocardiography, hourly vital signs, and serial laboratory evaluations including creatine kinase, comprehensive metabolic panel, and urinalysis to assess for myoglobinuria.
Within 72 hours of initiating treatment, the patient's temperature normalized, and muscle rigidity began to resolve. By day 5, CK levels had decreased to 1,250 U/L. Dantrolene was discontinued after 3 days, while bromocriptine was continued for a total of 10 days with gradual tapering. For the management of his underlying delirium, non-pharmacological approaches were emphasized, including early mobilization, sleep promotion, and frequent reorientation. When pharmacological intervention became necessary, low-dose quetiapine was cautiously introduced with close monitoring for recurrence of NMS symptoms. The patient was eventually discharged from the ICU on post-operative day 15 and transferred to a neurorehabilitation facility on day 22. At his 3-month follow-up, he demonstrated complete resolution of NMS sequelae with no residual neurological deficits.
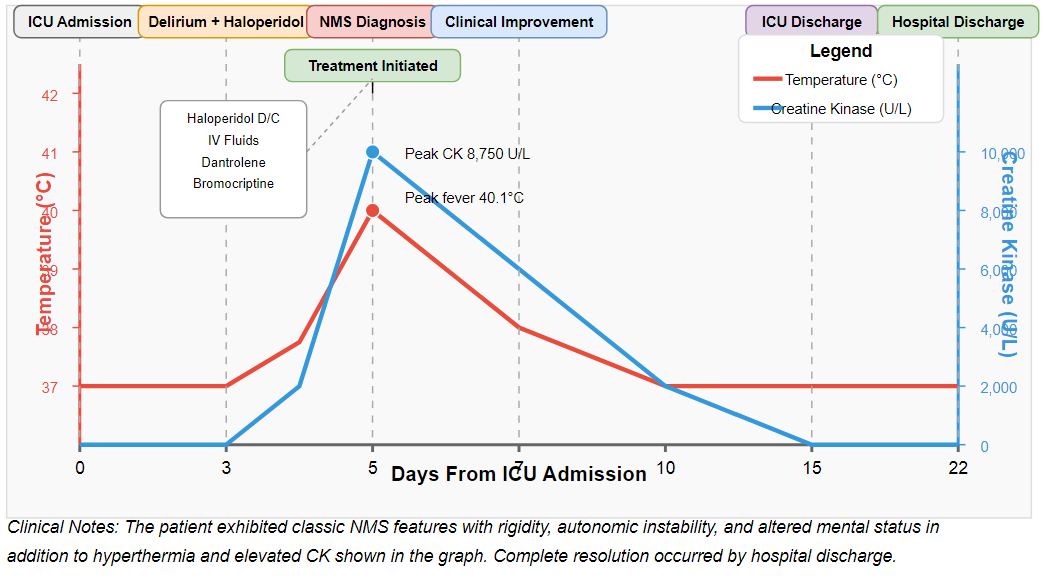
Figure 1: Clinical Course of Neuroleptic Malignant Syndrome case
DISCUSSION
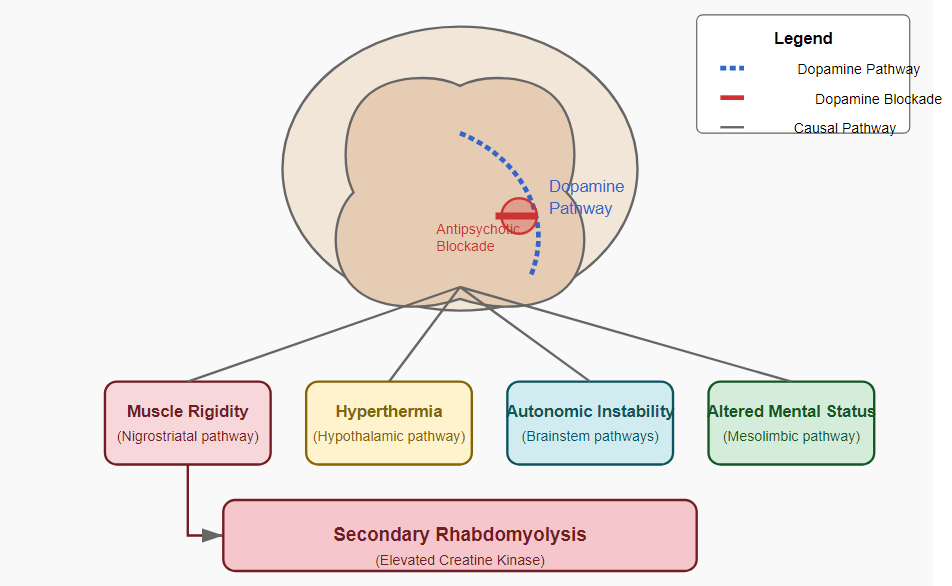
This case illustrates the potential risks associated with antipsychotic use in the management of ICU delirium, particularly highlighting the development of NMS as a serious iatrogenic complication. NMS is believed to result from sudden, profound dopamine blockade in the nigrostriatal, hypothalamic, and mesolimbic/mesocortical dopaminergic pathways[7]. The pathophysiology of NMS relates to the central role of dopamine in regulating muscle tone, thermoregulation, and autonomic function. Haloperidol, a high-potency typical antipsychotic, carries a particularly high risk due to its strong dopamine D2 receptor antagonism[8]. Critically ill patients may be especially vulnerable to developing NMS due to several risk factors:
Our patient exhibited all four cardinal features of NMS: altered mental status, rigidity, hyperthermia, and autonomic dysfunction, meeting the diagnostic criteria established by both the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and the International Expert Consensus Diagnostic Criteria for NMS[10].
Early recognition and prompt intervention are crucial for favourable outcomes in NMS. The initial management involves immediate discontinuation of the offending agent and supportive care focusing on cooling, hydration, and electrolyte correction. Pharmacological interventions target different aspects of the pathophysiology: benzodiazepines for anxiety and rigidity, dantrolene for hyperthermia and muscle rigidity through inhibition of calcium release from the sarcoplasmic reticulum, and dopaminergic agents like bromocriptine to reverse central dopamine blockade[11]. This case raises important considerations regarding the approach to delirium management in critically ill patients. Recent evidence suggests limited efficacy of antipsychotics in reducing delirium duration or severity, leading to updated guidelines emphasizing non-pharmacological strategies as first-line interventions[12]. When pharmacological management is deemed necessary, clinicians should carefully weigh the risks and benefits of antipsychotic use, particularly in patients with risk factors for NMS.
Several recent studies have explored alternative approaches to delirium management, including alpha-2 agonists like dexmedetomidine, which may offer advantages over antipsychotics in certain populations[13]. Additionally, emerging evidence supports early mobility programs, sleep promotion protocols, and multicomponent non-pharmacological interventions in preventing and managing delirium[14].
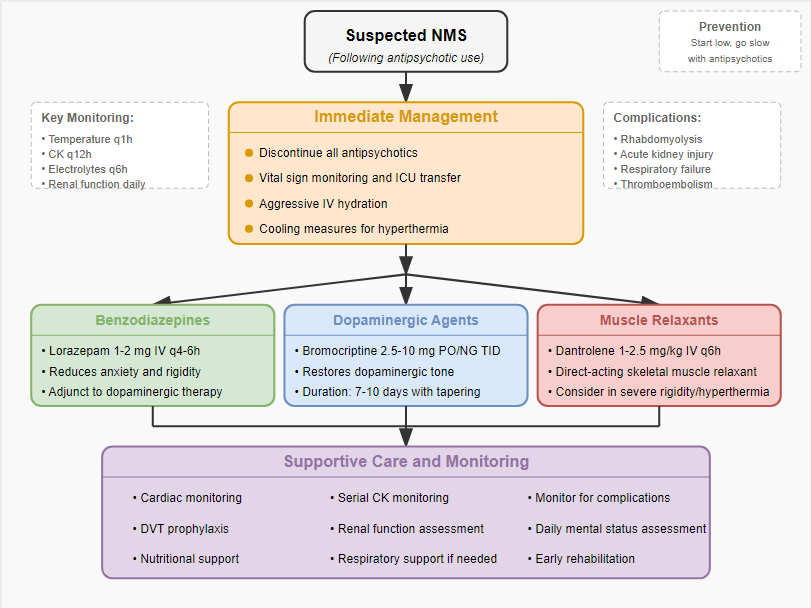
Figure 3: Management Approach to Neuroleptic Malignant Syndrome
CONCLUSION
This case underscores the importance of judicious use of antipsychotics in the management of ICU delirium. Clinicians should maintain a high index of suspicion for NMS when patients receiving antipsychotics develop unexplained fever, rigidity, or mental status changes. A multimodal approach to delirium prevention and management, emphasizing non-pharmacological strategies and careful selection of pharmacological agents when necessary, may help mitigate the risk of this potentially life-threatening complication. The pharmaceutical relevance of this case extends beyond the immediate clinical implications, highlighting the complex interplay between dopaminergic pathway disruption and idiosyncratic drug reactions. Further research into the genetic and molecular basis of NMS susceptibility may eventually allow for personalized risk assessment and more targeted approaches to delirium management in critically ill patients.
ACKNOWLEDGMENTS
I thank the patient and his family for providing consent for the publication of this case report. I also acknowledge the multidisciplinary ICU team whose collaborative efforts contributed to the successful management of this challenging case.
REFERENCES

Ranjith H. K.*, Neuroleptic Malignant Syndrome Following Haloperidol Administration in ICU Delirium: A Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3518-3523. https://doi.org/10.5281/zenodo.15476640
 10.5281/zenodo.15476640
10.5281/zenodo.15476640