S.S.P. Shikshan Sanstha’s Siddhi College of Pharmacy, Chikhali, Pune, Maharashtra, India 411062
Community-acquired bacterial pneumonia (CABP) remains a major cause of morbidity and mortality worldwide, particularly among elderly patients and individuals with underlying comorbid conditions. Despite the availability of multiple antibacterial agents, effective management of CABP is increasingly challenged by rising antimicrobial resistance and safety concerns associated with commonly used therapies. Macrolides have traditionally played a central role in the treatment of CABP due to their oral availability and activity against atypical pathogens; however, their clinical utility has been compromised by increasing resistance among Streptococcus pneumoniae, risk of QT interval prolongation, and clinically significant drug–drug interactions. Nafithromycin is a novel lactone ketolide developed to address the limitations of conventional macrolides. Structural modifications enhance its binding affinity to bacterial ribosomes, resulting in potent activity against macrolide-resistant respiratory pathogens. Nafithromycin demonstrates broad-spectrum antibacterial activity against typical and atypical CABP pathogens, favourable pharmacokinetic properties with excellent lung tissue penetration, and a reduced propensity for QT prolongation and cytochrome P450–mediated drug interactions. Clinical studies evaluating nafithromycin in patients with CABP have reported high clinical cure rates comparable to standard therapies, supporting its efficacy as an oral monotherapy. The favourable safety profile and simplified dosing regimen further enhance its suitability for outpatient management. In conclusion, nafithromycin represents a promising advancement in the treatment of community-acquired bacterial pneumonia and may offer an effective and safer alternative to existing macrolide therapies, particularly in regions with high macrolide resistance.
Community-acquired bacterial pneumonia (CABP) remains a major public health challenge worldwide, contributing significantly to morbidity and mortality across all age groups, particularly among elderly individuals, immunocompromised patients, and those with chronic conditions such as diabetes, chronic obstructive pulmonary disease, renal disease, and cardiovascular disorders [1,2]. Globally, CABP leads to millions of hospitalizations annually and places a substantial burden on healthcare systems due to prolonged hospital stays and intensive care requirements [1, 2].
In developing countries, this burden is exacerbated by delayed diagnosis, limited healthcare access, and suboptimal empirical antibiotic therapy. Even in well-resourced healthcare settings, rising antimicrobial resistance and safety concerns related to existing antibiotics compromise treatment outcomes [3, 4]. These challenges highlight the need for novel, effective, and safe oral antibacterial agents that can simplify therapy and improve patient outcomes.
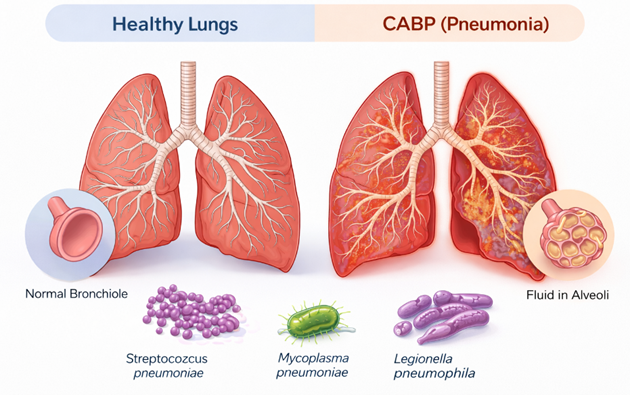
Figure 1: Comparison of Healthy Lungs and Community-Acquired Bacterial Pneumonia (CABP) with Common Causative Pathogens.
CABP is caused by a variety of bacterial pathogens, necessitating empirical treatment with broad-spectrum coverage. Streptococcus pneumoniae remains the predominant pathogen, accounting for a significant proportion of severe infections. Other commonly implicated bacteria include Haemophilus influenzae and Moraxella catarrhalis. Additionally, atypical pathogens such as Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila play a notable role, particularly in younger or ambulatory patients [2, 5]. The diversity of causative organisms complicates empirical therapy and underscores the importance of antibiotics active against both typical and atypical respiratory pathogens.
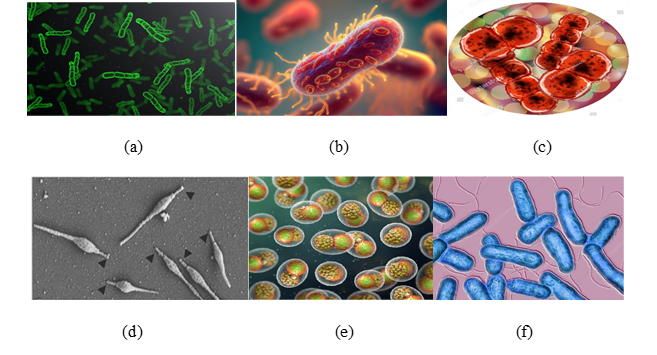
Figure 2: (a) Streptococcus pneumoniae (b) Haemophilus influenza (c) Moraxella catarrhalis (d) Mycoplasma pneumoniae (e) Chlamydophila pneumoniae (f) Legionella pneumophila
Currently, macrolides, fluoroquinolones, and β-lactam antibiotics form the backbone of CABP treatment. Although generally effective, these agents face limitations due to antimicrobial resistance, adverse effects, and safety concerns. Fluoroquinolones, for example, are linked to serious adverse events including tendinopathy, central nervous system effects, and dysglycemia [4]. Macrolides, while convenient for oral therapy and effective against atypical pathogens, have seen reduced susceptibility in key respiratory pathogens due to widespread use. β- Lactam antibiotics often require combination therapy to cover atypical organisms, which can increase pill burden and risk of non-compliance [3, 4].
Macrolide resistance occurs primarily through target site modification (ribosomal methylation or mutation), active drug efflux, and enzymatic inactivation, which prevent the antibiotic from binding to the 50S ribosomal subunit and inhibiting protein synthesis. The most common mechanism is methylation of the 23S rRNA, reducing the drug's affinity. Genes for macrolide resistance act via three main mechanisms - target site modification, activation of efflux pumps and enzymatic modification of the drug [7].
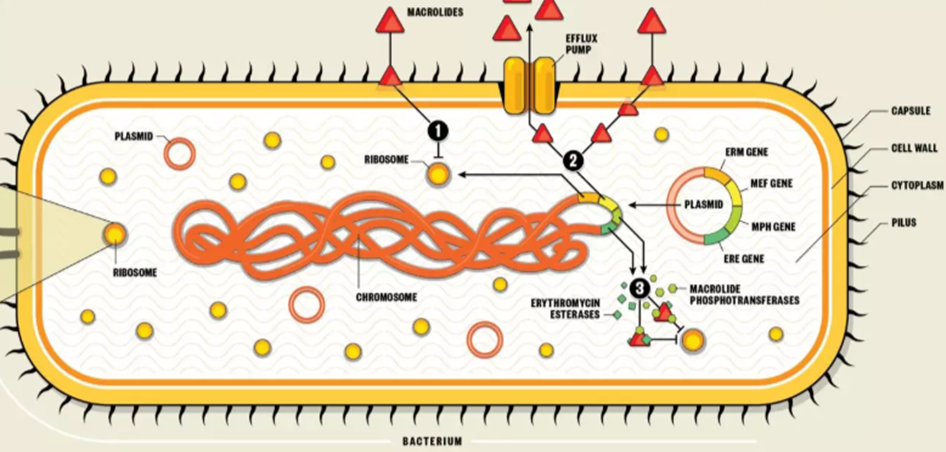
Figure 3: Mechanism of Macrolide Resistance [7].
The QT interval on an electrocardiogram (ECG) represents the total duration of ventricular depolarization and repolarization. Prolongation of the QT interval is clinically significant because it predisposes patients to life-threatening ventricular arrhythmias, particularly torsades de pointes (TdP). Drug-induced QT prolongation is a well-recognized adverse effect associated with several antimicrobial classes, including macrolides and fluoroquinolones, which are commonly used in the treatment of community-acquired bacterial pneumonia (CABP) [8,9].
Patients with CABP often have multiple risk factors for QT prolongation, such as advanced age, electrolyte imbalance, cardiovascular disease, and concomitant medications. Therefore, the cardiac safety profile of antibiotics is a critical consideration when selecting empirical and targeted therapy [9].
QT prolongation primarily occurs due to inhibition of cardiac potassium ion channels, especially the human ether-à-go-go-related gene (hERG, Kv11.1) channel. This channel mediates the rapid delayed rectifier potassium current, which is essential for phase 3 repolarization of the cardiac action potential [10].
When drugs inhibit the hERG channel:
Na+ influx → Ca2+ influx → K+ efflux → Normal QT
Drug-Induced QT Prolongation
Macrolide / Fluoroquinolone
↓
hERG (IKr) Channel Blockade
↓
↓ Potassium Efflux
↓
Prolonged Action Potential
↓
QT Interval Prolongation
↓
Risk of Torsades de Pointes
Figure 4: Mechanism of Drug-Induced QT Prolongation.
Macrolides such as erythromycin, clarithromycin, and azithromycin are known to prolong the QT interval through direct hERG channel inhibition. Additionally, many macrolides inhibit cytochrome P450 (CYP3A4), leading to increased plasma concentrations of co-administered QT-prolonging drugs [8, 11].
Clinical consequences include:
These limitations reduce the suitability of conventional macrolides for widespread outpatient management of CABP, particularly in high-risk populations [9].
CABP patients frequently receive combination therapy and supportive medications, increasing the risk of pharmacokinetic and pharmacodynamic interactions. Antibiotics with QT-prolonging potential require ECG monitoring, which is often impractical in outpatient settings. Consequently, there is a strong clinical demand for newer oral agents that retain macrolide-like efficacy without compromising cardiac safety [12].
Patients with community-acquired bacterial pneumonia (CABP) frequently belong to elderly or comorbid populations and are often prescribed multiple medications for chronic conditions such as cardiovascular disease, diabetes, and respiratory disorders. Polypharmacy substantially increases the risk of drug–drug interactions (DDIs), which may lead to reduced therapeutic efficacy, increased toxicity, or serious adverse events. Antibiotics used for CABP, particularly macrolides and fluoroquinolones, are among the most commonly implicated drug classes in clinically significant DDIs [15].
One of the most important mechanisms underlying DDIs is inhibition of hepatic cytochrome P450 (CYP) enzymes, especially CYP3A4. Several macrolides, including erythromycin and clarithromycin, are strong CYP3A4 inhibitors. When co-administered with drugs metabolized by this pathway, plasma concentrations of the co-administered drug may increase, resulting in toxicity [16].
Commonly affected drugs include:
Azithromycin has a lower CYP3A4 inhibitory effect but is still associated with clinically relevant interactions in susceptible patients [16, 17].
Macrolides can also inhibit membrane transport proteins such as P-glycoprotein (P-gp). Inhibition of P-gp alters the absorption and elimination of drugs like digoxin, leading to elevated systemic exposure and toxicity. Transporter-based interactions further complicate antibiotic selection in CABP patients receiving long-term medications [17].
Macrolide Antibiotic
↓
CYP3A4 / P-gp Inhibition
↓
↓ Drug Metabolism or Efflux
↓
↑ Plasma Drug Concentration
↓
Increased Toxicity / Adverse Effects
Figure 5: Mechanism of action of drug-drug interaction.
Pharmacodynamic interactions occur when two drugs exert additive or synergistic effects on the same physiological system. In CABP therapy, the most clinically relevant pharmacodynamic interaction involves QT interval prolongation.
When macrolides are co-administered with other QT-prolonging drugs (e.g., antiarrhythmics, antipsychotics, fluoroquinolones), the risk of torsades de pointes is significantly increased. This interaction is independent of drug concentration and can occur even at therapeutic doses [18].
The presence of DDIs can lead to:
In outpatient CABP management, avoiding antibiotics with high DDI potential is essential to ensure safety and treatment success [15, 19].
Nafithromycin is a novel lactone ketolide antibiotic designed to overcome macrolide resistance while improving safety. It exerts its antibacterial effect by inhibiting bacterial protein synthesis through binding to the 50S ribosomal subunit. Unlike traditional macrolides, nafithromycin demonstrates dual-site ribosomal binding, which enhances its affinity and reduces susceptibility to resistance mechanisms [13].
Specifically, nafithromycin interacts with:
This dual interaction leads to effective inhibition of translocation and premature termination of bacterial protein synthesis.
Resistance to macrolides commonly arises through:
Nafithromycin retains activity against many resistant strains because its structural modifications allow stable ribosomal binding even in the presence of methylated rRNA. This property is particularly valuable against Streptococcus pneumoniae, a predominant CABP pathogen [13, 14].
Unlike conventional macrolides, nafithromycin exhibits minimal interaction with the hERG channel and does not significantly inhibit CYP3A4. As a result:
These characteristics represent a major therapeutic advantage in the management of CABP [12, 14].
A major advantage of nafithromycin is its minimal inhibition of CYP3A4 and P-glycoprotein, significantly reducing its potential for pharmacokinetic DDIs. In vitro studies have demonstrated negligible effects on major drug-metabolizing enzymes, making nafithromycin safer for use in patients receiving multiple concomitant medications [20].
This favorable interaction profile, combined with reduced QT prolongation risk, supports its suitability as an oral monotherapy for CABP.
Nafithromycin
↓
Penetration into Bacterial Cell
↓
Binding to 50S Ribosomal Subunit
↓
Inhibition of Protein Synthesis
↓
Suppression of Bacterial Growth
↓
Clinical Cure of CABP
Figure 6: Mechanism of action Nafhithromycin.
EPIDEMIOLOGY OF COMMUNITY-ACQUIRED BACTERIAL PNEUMONIA (CABP)
Community-acquired bacterial pneumonia (CABP) remains a leading cause of infectious morbidity and mortality worldwide. Despite advances in antimicrobial therapy and vaccination, CABP continues to impose a substantial public health burden, particularly in low- and middle-income countries (LMICs) such as India. The epidemiology of CABP varies considerably across regions due to differences in population demographics, healthcare infrastructure, vaccination coverage, prevalence of comorbidities, and antimicrobial resistance patterns [21,22].
Globally, community-acquired pneumonia affects approximately 3–5% of adults annually, with bacterial pathogens accounting for a major proportion of clinically significant cases [23]. The estimated global incidence of CAP is ~4,000–4,500 cases per 100,000 population per year, with higher incidence rates observed at the extremes of age [24].
Lower respiratory tract infections, including CABP, are consistently ranked among the top three causes of infectious disease–related mortality worldwide, contributing to approximately 2–2.5 million deaths annually [24,25].
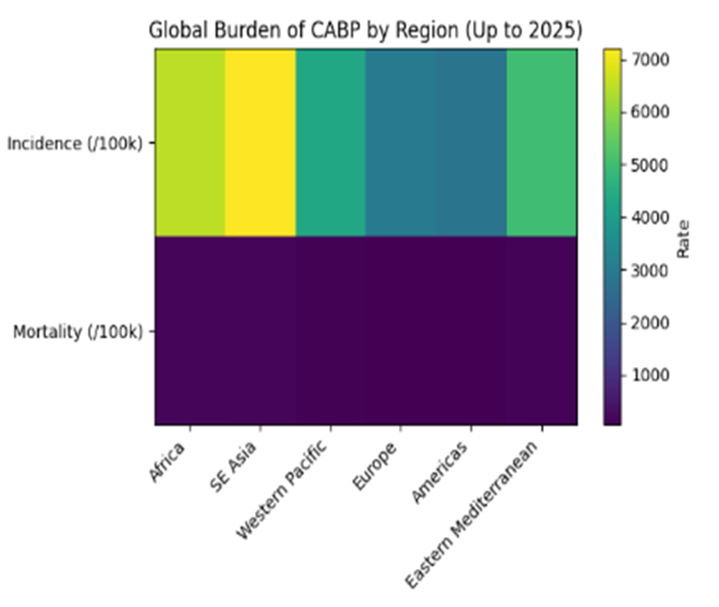
Figure 7: Marked regional differences in the incidence and mortality of CABP are observed worldwide, with the highest burden reported in South-East Asia and Africa.
CABP-associated mortality varies according to disease severity and healthcare setting:
Elderly patients (≥65 years), immune compromised individuals, and those with chronic cardiopulmonary diseases experience disproportionately higher mortality rates [22, 26].
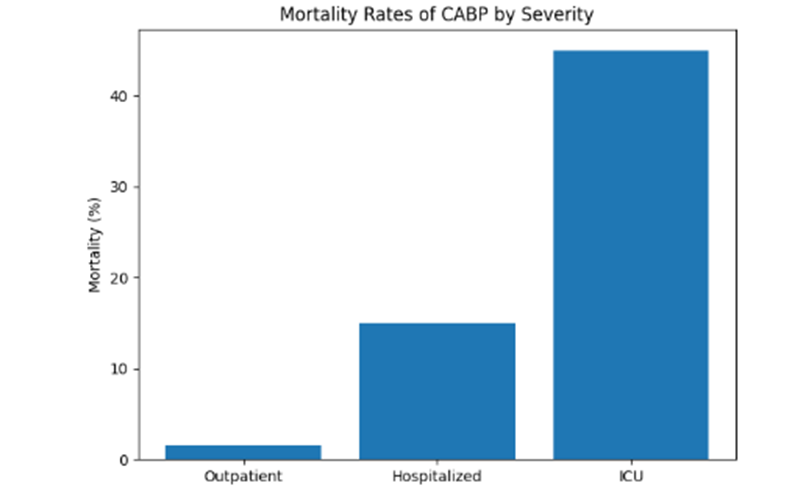
Figure 8: Mortality increases substantially with disease severity, particularly among ICU-admitted patients.
Epidemiological studies demonstrate a U-shaped age distribution, with the highest incidence and mortality observed in:
In older adults, incidence rates may exceed 25–40 cases per 1,000 persons per year, reflecting immunosenescence and increased comorbidity burden [23, 24].
Streptococcus pneumoniae remains the predominant bacterial cause of CABP globally, followed by Haemophilus influenzae, Staphylococcus aureus, and atypical pathogens such as Mycoplasma pneumoniae [27]. Increasing antimicrobial resistance, particularly macrolide and β-lactam resistance, has significantly influenced contemporary CABP epidemiology and treatment strategies [26, 27].
India bears a disproportionately high burden of pneumonia, contributing nearly 20–25% of global pneumonia cases. Epidemiological estimates suggest an annual pneumonia incidence of 5–11 cases per 1,000 population, corresponding to approximately 4–5 million adult CABP cases per year. Under-diagnosis, limited access to microbiological testing, and under-reporting—particularly in rural regions—suggest that the true burden may be substantially higher [28, 29].
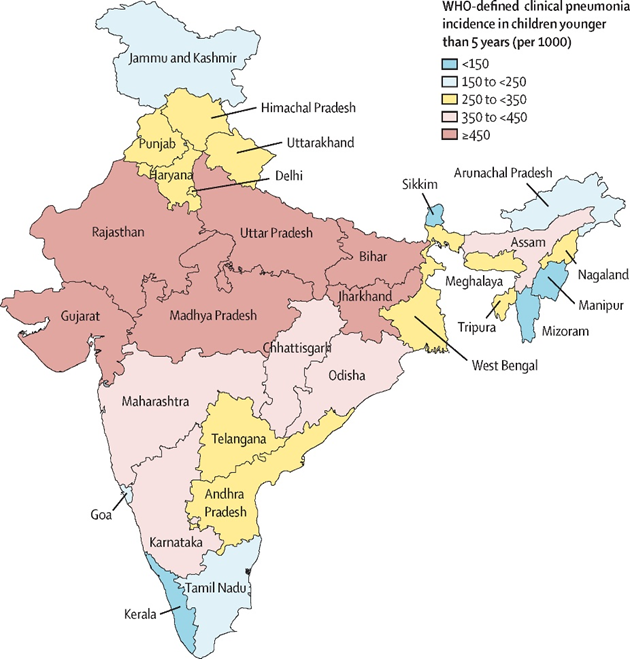
Figure 9: WHO-Defined Clinical pneumonia incidence in children younger than 5 years (per 1000).
Mortality rates associated with CABP in India remain significantly higher than those reported in high-income countries:
Delayed healthcare presentation, inappropriate empirical therapy, limited ICU capacity, and high prevalence of multidrug-resistant organisms contribute to adverse outcomes [21, 29].
In contrast to Western populations, Indian studies report a higher prevalence of Gram-negative pathogens, particularly in hospitalized and severe cases. This pathogen distribution has direct implications for empirical antibiotic selection and antimicrobial stewardship in India [28, 29]. The relative contribution of major bacterial pathogens causing CABP in India is illustrated in Fig1.9.
Table 1: Major bacterial pathogens causing CABP in India
|
Pathogen |
Epidemiological relevance |
|
Streptococcus pneumoniae |
Most common overall pathogen |
|
Klebsiella pneumoniae |
Common in severe & elderly patients |
|
Staphylococcus aureus |
Post-viral and severe pneumonia |
|
Mycoplasma pneumoniae |
Younger adults |
|
Pseudomonas aeruginosa |
ICU and high-risk patients |
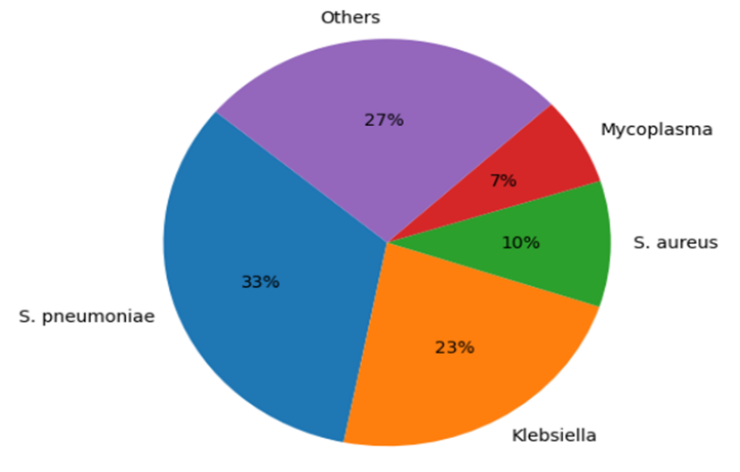
Figure 10: Etiological Distribution of CABP in India.
Distribution of major bacterial pathogens causing community-acquired bacterial pneumonia in India. Streptococcus pneumoniae remains the predominant pathogen, while Gram-negative organisms, particularly Klebsiella pneumoniae, contribute significantly to hospitalized and severe cases. CABP incidence in India demonstrates seasonal peaks during winter and post-monsoon months, likely related to increased viral respiratory infections, air pollution, and overcrowding.
OVERVIEW OF THE NOVEL LACTONE KETOLIDE NAFHITHROMYCIN:
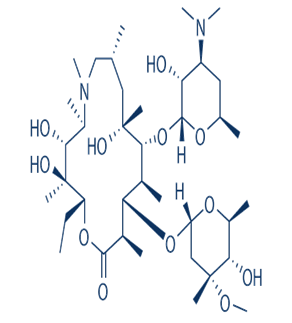
Nafithromycin (also known as WCK 4873) is a next-generation ketolide antibiotic developed as an advanced derivative of the macrolide class. Chemically, it belongs to the lactone ketolide subclass, which represents structurally modified macrolides designed to overcome resistance mechanisms associated with conventional agents such as azithromycin and clarithromycin. Ketolides differ from classical macrolides primarily by removal of the cladinose sugar at the C3 position, replacement with a keto functional group, and the introduction of an extended aryl–alkyl side chain. These modifications confer enhanced ribosomal binding, improved antibacterial potency, and reduced susceptibility to macrolide resistance mechanisms [30, 31].
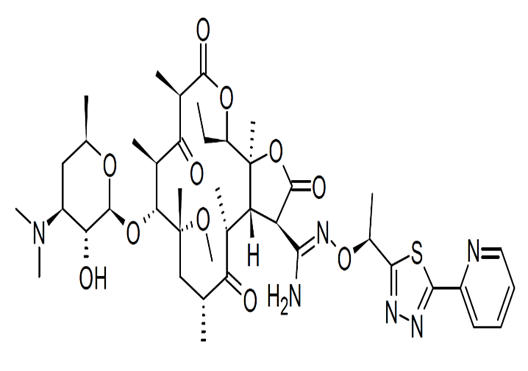
Figure 11: Chemical Structure of Nafhithromycin
Formula: C42H62N6O11S
Molecular Weight: 859.05 g/mol
Structure: It is a 16-membered lactone-ketolide featuring a 2-pyridine-1,3,4-thiadiazole side chain connected via a four-atom spacer.
Nafithromycin retains a 14-membered macrolactone ring, a core structural feature essential for binding to the bacterial ribosome. This lactone ring acts as the scaffold upon which additional functional groups are positioned to optimize antimicrobial activity. Compared with earlier macrolides, the ring system in nafithromycin is chemically stabilized to enhance acid resistance and metabolic durability [32].
A defining feature of nafithromycin is the replacement of the cladinose sugar at the C3 position with a keto group. In classical macrolides, the cladinose sugar plays a key role in triggering inducible MLS resistance via erm-mediated methylation of the 23S rRNA. Removal of this sugar significantly reduces resistance induction and enhances activity against macrolide-resistant Streptococcus pneumoniae. This modification is fundamental to the ketolide class and directly contributes to the superior resistance profile of nafithromycin [31].
Nafithromycin contains a rigid aromatic side chain attached to the macrolactone ring, which is absent in azithromycin and clarithromycin. This side chain extends into domain II of the 23S rRNA, enabling a second anchoring point within the ribosomal exit tunnel. As a result, nafithromycin exhibits dual ribosomal binding, significantly increasing binding affinity and reducing the likelihood of resistance due to target site modification [30].
|
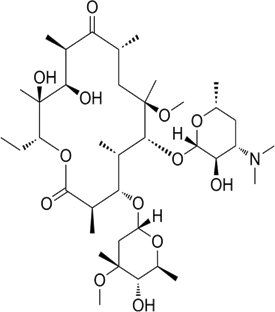
|
|
|
Azithromycin |
Clarithromycin |
Nafhithromycin |
Azithromycin is a 15-membered azalide macrolide, characterized by the insertion of a nitrogen atom into the lactone ring and retention of the cladinose sugar. While azithromycin demonstrates broad-spectrum activity, its reliance on a single ribosomal binding site (domain V) makes it vulnerable to methylation-mediated resistance. In contrast, nafithromycin:
These differences translate into higher potency against resistant pneumococcal strains and improved pharmacodynamic performance [33, 34].
Clarithromycin is a 14-membered macrolide derived from erythromycin with enhanced acid stability due to methoxy substitution. However, it still retains the cladinose sugar and binds predominantly to domain V of 23S rRNA, making it susceptible to MLS<sub>B</sub> resistance. Nafithromycin overcomes these limitations through:
As a result, nafithromycin demonstrates greater in vitro and in vivo activity against macrolide-resistant respiratory pathogens [32, 35].
Table 2: Structural Comparison of Nafithromycin with Azithromycin and Clarithromycin.
|
Feature |
Nafithromycin |
Azithromycin |
Clarithromycin |
|
Antibiotic class |
Ketolide |
Macrolide (Azalide) |
Macrolide |
|
Lactone ring |
Modified macrolactone |
15-membered |
14-membered |
|
Cladinose sugar |
Absent (keto group) |
Present |
Present |
|
Extended side chain |
Present |
Absent |
Absent |
|
Ribosomal binding sites |
Domain II & V |
Mainly Domain V |
Domain V |
|
Activity vs macrolide-resistant strains |
High |
Low–Moderate |
Low |
|
Lung tissue penetration |
Excellent |
Moderate |
Moderate |
The collective structural modifications in nafithromycin lead to:
These properties make nafithromycin particularly suitable for community-acquired bacterial pneumonia (CABP), where high pulmonary concentrations and resistance coverage are critical. Nafithromycin represents a rationally designed ketolide, in which specific chemical modifications—namely cladinose removal, keto substitution, and an extended aryl–alkyl side chain—directly translate into improved antibacterial efficacy and resistance suppression.
Its dual ribosomal binding mechanism distinguishes it structurally and functionally from azithromycin and clarithromycin, positioning nafithromycin as a promising next-generation therapy for respiratory infections [34, 35].
Unlike classical macrolides that bind primarily to domain V of the 50S ribosomal subunit, nafithromycin interacts simultaneously with domain V and domain II of 23S rRNA. This dual interaction stabilizes the drug–ribosome complex and prevents displacement caused by methylation or point mutations.
This mechanism:
Dual binding is considered the principal structural reason for nafithromycin’s enhanced antibacterial spectrum and lower resistance potential [31].

Figure 12: Dual ribosomal binding mechanism of nafithromycin at domains II and V of 23S rRNA.
Nafithromycin (marketed as Miqnaf) is a well-tolerated novel macrolide antibiotic generally causing mild side effects like dysgeusia (taste change), nausea, diarrhea, headache, and dizziness. It shows minimal gastrointestinal issues and is considered a safer alternative to older antibiotics for treating Community-Acquired Bacterial Pneumonia (CABP).
Common Side Effects:
Based on clinical trial data, the most frequently reported treatment-emergent side effects include:
ANALYTICAL METHODS DEVELOPED FOR NAFITHROMYCIN (WCK 4873)
Analytical methods are crucial in drug development for quantification, pharmacokinetic studies, impurity profiling, quality control, and microbiological activity assessment. Nafithromycin, a novel lactone ketolide antibiotic under development for community-acquired bacterial pneumonia (CABP), has prompted the development of several analytical techniques to support its bioanalysis, quality control, and microbiological evaluation.
One of the most widely used methods for nafithromycin quantification in biological matrices is liquid chromatography-tandem mass spectrometry (LC-MS/MS). This method enables sensitive, precise, and selective measurement of nafithromycin and its major metabolite in human plasma, urine, and other samples, which is essential for pharmacokinetic and bioavailability studies.
A validated LC-MS/MS assay was developed for simultaneous quantification of nafithromycin and its N-desmethyl metabolite in human plasma. Protein precipitation was used for sample preparation, and clarithromycin served as an internal standard. The calibration curve was linear (r ≥ 0.99) over a wide range (10–5000 ng/mL), with acceptable precision and accuracy according to regulatory bioanalytical guidelines [37].
A similar LC-MS/MS method was applied in pharmacokinetic studies of oral nafithromycin, using protein precipitation with acetonitrile followed by LC-MS/MS analysis. Nafithromycin concentrations in plasma and in bronchoalveolar lavage fluids were quantified with linear standard curves and low limits of quantification, supporting in vivo PK/PD research [38].
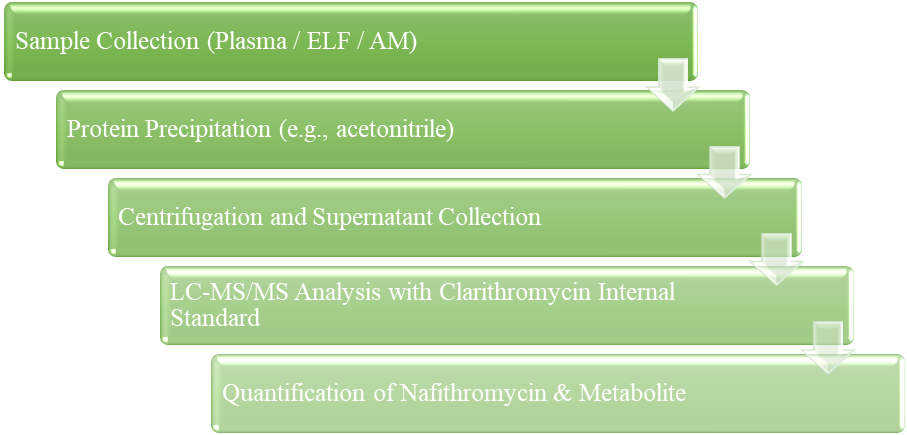
Figure 13: Bio analytical Workflow
Table 3: Key LC-MS/MS Bio analytical Parameters
|
Parameter |
Result |
|
Sample prep method |
Protein precipitation |
|
Matrix |
Human plasma, BAL fluid |
|
Internal standard |
Clarithromycin |
|
Linear range |
10–5000 mg/mL |
|
LLOQ |
10 mg/mL |
|
Precision & accuracy |
Within regulatory limits |
Classic chromatographic analysis of nafithromycin using RP-HPLC has been used for quantitative estimation and detection of related impurities. One analytical investigation employed an RP-HPLC system with a C18 column, buffer–acetonitrile mobile phase, and UV detection to quantify nafithromycin in pharmaceutical samples [39].
A refined method using RP-UPLC (BEH C18 column with a gradient mobile phase and PDA detection) offers faster run times and improved resolution than traditional HPLC. This is useful for routine quality control during drug substance and formulation analysis and provides robust analytical data for regulatory compliance [39].
Ultra-High-Performance Liquid Chromatography coupled with mass spectrometry (UHPLC-MS) has also been developed for quantifying nafithromycin with high specificity. This technique integrates chromatographic separation with mass detection, enhancing sensitivity and structural information, and is particularly useful for metabolite profiling and trace level quantitation [39].
Table 4: Chromatographic Methods Summary
|
Method |
Detection |
Column |
Mobile Phase |
Application |
|
RP-HPLC |
UV |
C18 |
Buffer/Acetonitrile |
Quantification, QC |
|
RP-UPLC |
PDA |
BEH C18 |
Gradient ACN/Formic Acid |
Rapid assay |
|
UHPLC-MS |
MS |
C18 |
ACN/Formic Acid |
High specificity quantitation |
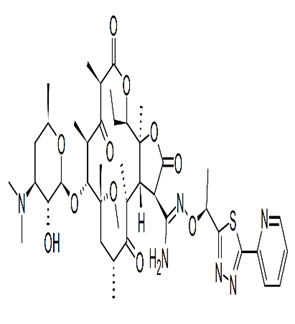
Another key analytical advancement is the identification and quantification of related impurities of nafithromycin using reversed-phase liquid chromatography compatible with mass spectrometry. Forced degradation studies revealed process impurities and degradation products. Chromatographic separation using XTerra C18 and gradient elution, followed by MS identification, allowed structural characterization of impurities, supporting stability studies and quality control [40].
Figure 14: Impurity Analysis Framework
Although not an analytical chemistry technique per se, determining antimicrobial susceptibility and quality control (QC) ranges is essential for clinical research and surveillance. Using standard broth micro dilution and disk diffusion tests, quality control ranges for nafithromycin were established for key control strains (e.g., S. aureus, S. pneumoniae, H. influenzae). These methods define expected inhibition zones and MIC QC ranges, which are used in monitoring susceptibility and validating phenotypic assays [41].
Table 4: Nafithromycin MIC QC Ranges (CLSI)
|
Organism (ATCC) |
Disk Diffusion (mm) |
MIC Range (µg/mL) |
|
S. aureus 25923 |
25–31 |
— |
|
S. aureus 29213 |
— |
0.06–0.25 |
|
E. faecalis 29212 |
— |
0.016–0.12 |
|
S. pneumoniae 49619 |
25–31 |
0.008–0.03 |
|
H. influenzae 49247 |
16–20 |
2–8 |
Method Validation and Regulatory Perspectives:
Each analytical method described above has been evaluated and validated according to standard guidelines (e.g., US FDA bioanalytical method validation protocols) to ensure accuracy, precision, linearity, specificity, sensitivity, and reproducibility. These validations are critical for clinical trials and eventual regulatory submission of nafithromycin [37].
Table 5: Developed Analytical Method and their applications.
|
Analytical Category |
Methods |
Applications |
|
Bioanalytical Quantitation |
LC-MS/MS |
PK, bioavailability |
|
Chromatographic Assay |
RP-HPLC, RP-UPLC, UHPLC-MS |
QC, assay |
|
Impurity Profiling |
RP-LC + MS |
Stability, degradation |
|
Microbiological QC |
Broth microdilution & disk diffusion |
Susceptibility testing |
|
Future Tools |
Rapid AST, biosensors |
Fast MIC / clinical use |
FUTURE RESEARCH GAPS IN ANALYTICAL METHOD DEVELOPMENT FOR NAFITHROMYCIN
Analytical methods for nafithromycin exist for LC–MS/MS quantification, HPLC assays, impurity profiling, and microbiological susceptibility testing. However, several opportunities remain to advance the field further- particularly in the realms of green analytical chemistry, rapid clinical testing, high-throughput capability, and method standardization [44–48].
Although UV-visible spectroscopy is simple and cost effective for some drug assays, no green UV analytical methods have been comprehensively published for nafithromycin yet.
Research Gaps:
a) Lack of UV Methods for Nafithromycin
b) Need for Green Solvent Systems
Table 6: Potential Research Priorities for UV-based Assays
|
Research Priority |
Rationale |
|
UV Method Development for Nafithromycin |
Provides simple QC assay |
|
Use of Green Solvents (Ethanol, Water) |
Minimizes environmental impact |
|
Validation per ICH Q2(R1) |
Ensures accuracy & regulatory compliance |
|
Stability-Indicating UV Methods |
Differentiates nafithromycin vs degradation products |
Current HPLC and UPLC methods for nafithromycin use traditional organic phases (acetonitrile, methanol), which are toxic and generate hazardous waste. Future research should integrate green chromatography principles [46].
Research Gap-
a) Greener Mobile Phase Development
b) Green Stationary Phases
c) HPLC in Real Samples
Table 7: HPLC/UPLC Green Chemistry Opportunities
|
Area |
Current Status |
Future Gap |
|
Mobile Phase |
ACN / MeOH |
Ethanol / Water / ILs |
|
Stationary Phase |
Conventional C18 |
Monolithic / Core–shell |
|
Sample Prep |
Protein precipitation |
Green extraction methods |
|
Run Time |
Medium |
Ultra-fast UPLC |
Rapid methods that provide quantitation within minutes are lacking.
Gap:
No published implementation of high-throughput LC–MS/MS with automated sample prep for nafithromycin PK monitoring.
Future Direction:
Explore robotic sample handling and 96-well plate extraction systems.
Phenotypic AST currently relies on standard broth microdilution, which takes 18–24 hours.
Gap:
Rapid AST methods (e.g., optical metabolite detection, microdroplet sensors) have not been validated for nafithromycin.
Future Direction:
Integrate techniques like:
Gap:
No global inter-laboratory validation protocols specific to nafithromycin analytical methods.
Future Direction:
Harmonize nafithromycin assay protocols under organizations like CLSI, EMA, FDA.
While some impurity profiling exists, full stability-indication protocols under various stress (heat, light, pH) are limited.
Future Direction: Develop robust stability studies with green analytical endpoints.
Most PK methods are in plasma only.
Future Direction:
Expand validated methods to:
This will support better correlation with CABP efficacy.
Table 8: Comprehensive Research Gaps
|
Area |
Current Status |
Research Gap |
|
UV Methods |
Not yet reported |
Need green UV methods |
|
HPLC/ UPLC |
Uses hazardous solvents |
Greener chromatography |
|
Bioanalytical quantification |
LC–MS/MS established |
High-throughput, automation |
|
Susceptibility methods |
Broth microdilution only |
Rapid AST |
|
Global standardization |
Not established |
Harmonized protocols |
|
Stability studies |
Limited |
Full stress decomposition |
|
Tissue assays |
Plasma centric |
Lung/ELF validated |
CONCLUSION:
Community-acquired bacterial pneumonia (CABP) continues to represent a significant global health burden, particularly in elderly individuals, patients with comorbidities, and populations in low- and middle-income countries. The increasing prevalence of antimicrobial resistance, safety concerns such as QT interval prolongation, and clinically significant drug–drug interactions associated with conventional macrolides and fluoroquinolones have substantially limited current therapeutic options. These challenges underscore the urgent need for safer, effective, and resistance-resilient oral antibacterial agents for CABP management.
Nafithromycin, a novel lactone ketolide antibiotic, has emerged as a promising next-generation therapeutic option designed to address these unmet clinical needs. Its rational structural modifications—namely removal of the cladinose sugar, incorporation of a C3 keto group, and addition of an extended aryl–alkyl side chain—enable dual ribosomal binding at domains II and V of the 23S rRNA. This unique mechanism enhances antibacterial potency and preserves activity against macrolide-resistant respiratory pathogens, particularly Streptococcus pneumoniae. Importantly, nafithromycin demonstrates a favorable safety profile with minimal hERG channel inhibition, reduced QT prolongation risk, and negligible CYP3A4 and P-glycoprotein interaction potential, making it well suited for outpatient therapy and polypharmacy-prone populations.
From an analytical perspective, substantial progress has been made in developing robust bioanalytical and chromatographic methods for nafithromycin, including LC–MS/MS assays for pharmacokinetic evaluation, RP-HPLC/UPLC methods for quality control, and LC–MS–based impurity profiling to support stability and regulatory requirements. However, notable research gaps remain, particularly in the development of cost-effective green UV spectrophotometric methods, environmentally sustainable chromatographic techniques, rapid antimicrobial susceptibility testing, and high-throughput automated bioanalysis. Addressing these gaps will be critical for expanding nafithromycin accessibility, supporting antimicrobial stewardship, and aligning future analytical workflows with green chemistry principles.
Overall, nafithromycin represents a clinically and analytically important advancement in the management of CABP. Its integrated advantages- enhanced efficacy against resistant pathogens, improved cardiac and drug–drug interaction safety, and strong lung tissue penetration—position it as a valuable addition to the current therapeutic armamentarium. Continued clinical evaluation, method standardization, and innovation in green and rapid analytical approaches will further strengthen its role in contemporary and future CABP management strategies.
ABBREVIATIONS:
|
Abbreviation |
Full Form |
|
ACN |
Acetonitrile |
|
AST |
Antimicrobial Susceptibility Testing |
|
BAL |
Bronchoalveolar Lavage |
|
CABP |
Community-Acquired Bacterial Pneumonia |
|
CAP |
Community-Acquired Pneumonia |
|
CLSI |
Clinical and Laboratory Standards Institute |
|
CYP |
Cytochrome P450 |
|
CYP3A4 |
Cytochrome P450 3A4 |
|
DDI |
Drug–Drug Interaction |
|
ECG |
Electrocardiogram |
|
ELF |
Epithelial Lining Fluid |
|
erm |
Erythromycin Ribosome Methylation gene |
|
FDA |
Food and Drug Administration |
|
hERG |
Human Ether-à-go-go–Related Gene |
|
HPLC |
High-Performance Liquid Chromatography |
|
ICU |
Intensive Care Unit |
|
ICH |
International Council for Harmonisation |
|
IKr |
Rapid Delayed Rectifier Potassium Current |
|
LC–MS/MS |
Liquid Chromatography–Tandem Mass Spectrometry |
|
LMICs |
Low- and Middle-Income Countries |
|
LLOQ |
Lower Limit of Quantification |
|
MLSB |
Macrolide–Lincosamide–Streptogramin B |
|
MIC |
Minimum Inhibitory Concentration |
|
mef |
Macrolide Efflux gene |
|
mph |
Macrolide Phosphotransferase |
|
P-gp |
P-glycoprotein |
|
PDA |
Photodiode Array |
|
PK/PD |
Pharmacokinetics / Pharmacodynamics |
|
QC |
Quality Control |
|
QT |
Time interval between Q and T waves on ECG |
|
RP-HPLC |
Reversed-Phase High-Performance Liquid Chromatography |
|
RP-UPLC |
Reversed-Phase Ultra Performance Liquid Chromatography |
|
TdP |
Torsades de Pointes |
|
UHPLC-MS |
Ultra-High-Performance Liquid Chromatography–Mass Spectrometry |
|
UV |
Ultraviolet |
|
WHO |
World Health Organization |
DECLARATIONS:
Acknowledgement: Would like to thank the SSP Shikshan Sanstha’s Siddhi College of Pharmacy, Chikhali, Pune for providing infrastructure.
Funding Sources: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest: The authors do not have any conflict of interest.
Ethics Statement: This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Consent to participate: This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration: This review does not involve any clinical trials.
Permission to reproduce material from other sources: Not Applicable
Consent to publish: Not applicable. This article does not contain any individual person’s data in any form (including individual details, images, or videos).
Author Contributions:
Vaishnavi Singh*: Investigation, Writing, review & editing, Conceptualization.
Dr. Hitanshi Darji: Investigation, Supervision, Conceptualization.
Dr. Pravin Sable: Editing, Supervision.
REFERENCES



Vaishnavi Singh, Dr. Hitanshi Darji, Dr. Pravin Sable, Next-Generation Ketolides in Respiratory Infections: A Comprehensive Review of Nafithromycin in CABP, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2205-2227. https://doi.org/10.5281/zenodo.18635604
 10.5281/zenodo.18635604
10.5281/zenodo.18635604
