
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of pharmacology, Karnataka college of pharmacy, Bangalore
NAFLD stands as a worldwide health issue which defines itself when liver cells contain greater than 5% of their weight in extra fat independent from alcoholic liver disease. The disease manifests as liver disorders starting from photosteatosis and gradually advancing to widespread nonalcoholic fatty hepatitis (NASH) until it develops into cirrhosis followed by hepatitis C-related fibrosis and hepatocellular carcinoma. The presence of NAFLD commonly arises from metabolic syndrome together with obesity and type-2 diabetes as well as dyslipidemia and insulin resistance conditions. More than 25% of the population on Earth develops this illness which leads to higher rates of obesity together with metabolic diseases. Insulin resistance along with free fatty acids function as key mechanisms of non-alcoholic fatty liver disease pathogenesis by causing inflammation and liver cell damage. The main strategy in NAFLD management starts with lifestyle changes because these methods boost metabolic activity and reduce liver fat composition. The main benefit of bariatric surgical procedures surpasses all other treatment options for highly obese patients. Additional studies are required before scientists can assess the potential of drug treatment for NAFLD. The present review investigates NAFLD's wide-ranging pathophysiology together with its associated risk elements as well as applicable treatment approaches. Treatment orders which are effective serve to prevent rising health expenses that accompany illness prevalence and health costs associated with the disease.
Background: If there is hepatitis virus infection or more than 5 percent of the liver stores body weight by lipids than patient becomes non-alcoholic fatty liver disease [1]. Non-alcoholic fatty liver disease (NAFLD) is a chronic liver disease in which excessive alcohol consumption or otherwise, fat storage in the liver increases. The liver type expression of the metabolic syndrome was the thought to be closely associated with dyslipidemia, insulin resistance, obesity and diabetes type [2]. The early expression of non-alcoholic fatty hepatitis (NASH) is defined as a disease that further goes onto advanced disease such as cirrhosis, fibrosis and hepatocellular carcinoma, in the simple liver form of steatosis (non-alcoholic fatty liver disease or NAFL).[3]It is acknowledged that NAFLD is the major cause of chronic liver diseases worldwide, and its rate of incidence has increased due to metabolic diseases and obesity. The incidence of NAFLD is some 30 times population factor geographically, and though varying, is about 25% worldwide. [4] The incidence of NAFLD is increasing but most patients remain undiagnosed and until late disease they are usually asymptomatic. After the diagnosis, the most usual way to evaluate the NASH severity and fibrosis is through a liver biopsy, but other imaging techniques used to make the diagnosis include MRI, ultrasound, and fibroscan. There were no drugs approved by the FDA currently, with the majority of treatment diet, movement and weight loss.[5]Currents of the trial involve biomarkers, potential treatment goals, and enterohepatic interactions. For this reason, there are now increased global impacts on non-alcoholic fatty liver disease (NAFLD)[6]
Prevalence and Epidemiology of Non-Alcoholic Fatty Liver Disease (NAFLD):
Similarly, non-alcoholic greasy liver infection (NAFLD) may be a true disease affiliated with weight, diabetes and the metabolic disorder. According to today’s various facts known, we estimate that NAFLD attacks 25% of all grown-ups around the world. For South America (31%) they were found to be the foremost common on all continents; and for the Center East (32%), the least flare-up (14%) was found in Africa. This is usually if not in line with past thinks on to appear comparative predominance of NAFLD within the US and Europe. Nevertheless, what was an appealing finding was that Asians had a rate of NAFLD that was relatively tall (27%), and they were more apparent (64%). It might be due to the truth that the moo BMI breakpoint was obesity. Moreover, it tends to occur more in children and teenagers especially in countries where corpulence is commonplace. By doing so, it was supposed to increase the length of illness and the necessity for various open wellbeing exercises. [7]
Importance of NAFLD as a Public Health Concern
They have become important worldwide health problems due to tall predominance, solid relationship with metabolic clutters, and tall financial costs of greasy liver infection (NAFLD) without liquor utilization. Today, a constant liver infection is the first among the top most common causes in the world which took place in 25% of the population. Open wellbeing intercessions frequently endeavor to fulfill this also because of the need of compelling medications and rising wellbeing costs. [8]
Pathophysiology of non-alcoholic fatty liver disease:
There are various key mechanisms in the NAFLD pathophysiology
Insulin resistance and metabolic syndrome:A couple of a few illnesses influenced by two closely related metabolic indications − affront home and the metabolic disorder: Sort 2 diabetes, coronary illness and non alcoholic greasy liver disease. It is possible that one condition could be the affront resistance, or in other words the cells do not react correctly to insulin that affects glucose retention. It may be a ailment that enhances the danger of coronary failure and is focal to weight, hypertension, dyslipidemia and hyperglycemia. Once FFAs penetrate hepatocytes and initiate hepatocyte harm such as aggravation, apoptosis, endoplasmic reticulum (ER) stretch and swelling, they cause NAFLD or indeed NASH. [10] Affront is exceedingly restrained from fat tissue lipolysis. Onroud, this restraint is misplaced and the stream exerted in fat tissue for the production of FFAs is greatly expanded in IR conditions, such as NAFLD. One of the key transcriptional controllers of the DNL qualities is sterol administrative part official protein-1C (SREBP-1C) which is moved by IR because of the hyperinsulinemia. Also, strides are made in hindrance of FFA beta oxidation to liver lipid capacity. [11]
Lipid metabolism and accumulation in the liver: The pathologic feature of NAFLD is excess hepatic lipid accumulation. There are many types of lipid disorders. The major targets of this study are hepatic ceramide excess, hepatic injury, arachidonic acid metabolism and inflammation,and FA-induced hepatotoxicity.[12]
Hepatotoxicity and FA Accumulation: The term lipid poisonous quality portrays the structure of lipotoxic lipids, organella bustedness, and chronic irritation because of changes in cell lipid substance. In that ponder, we considered the association between the specific effects of FA poisonous quality on mitochondria and peroxisomes, and NAFLD and lipotoxicity. These less polarised layers, which accelerate FA amassing, increase from mitochondrial harm, incitement of mitochondria to oxidation and vitality digestion system. Liver aggravation and Nash treatment forms deliver irritation, cytokines, chemokines and their receptors, and regular and general resistant cells. A hindrance of tissue instruments results when aggravation of the liver occurs. Overhauling extracellular structure (ECM), these forms recover harmed hepatocytes, profit hepatocyte cell expansion and take an interest in reenactment of the staorene compartment. [13, 14]
Arachidonic acid and inflammation
Major inductors of cell harm and also death in non-alcoholic steatohepatitis (NASH) are expanded liver mirrors from FFA. A subsequent consider showed that lipid substance widened in NAFLD patients, yet the liver FFA substance was not changed. Despite this, there is no relationship between the circulating FFA reflect and the cell substance. This may be as a result of PUFAs being included in the pathogenesis of nonalcoholic greasy liver disease (NAFLD), the presence of which may have anti-inflammatory impacts, if PUFA structure is appropriate. Arachidonic corrosive is an unsaturated omega-6 fatty acid (N6 PUFA), long chain polyunsaturated essential fatty acid, which is a pioneer of extremely effective proinflammatory eicosanoids. Expended irritation can thus be related to the move from simple liver recolouring to NASH. [15,16] Since arachidonic corrosive metabolites are found exceptionally early in NAFLD and LDS are over produced as an overall fiery eicosanoid, LDS reflects a general fiery eicosanoid. Additionally, considers of steatosis in patients with NAFLD have repeatedly been demonstrated to be a relationship of enlarged liver N6:N3 proportion and scales and seriousness of plasma and NAFLD. It utilizes a partitioned consider to degree the main lipid species of the liver, offering quick and sharp information regarding the pathogenesis of nonalcoholic greasy liver malady. There is an expansion of the n6:n3 fas proportion when arachidonic corrosive and tall degrees are evacuated from n3 FAs. [17]
Role of oxidative stress:It is caused due to the awkward nature in the formation of ROS and the antioxidant resistances that leads to tissue and DNA damage. The etiology may be brought about by an unsettling influence of the antioxidant structure or an change in the generation of preoxidant items. Indeed, it is basic for tissue repair, and additionally can conceal dynamic phases of beginning or corruption of conditions, including a record of systemic conditions, cardiovascular ailment, persistent bowel sickness, neurological and behavioral disarranges. It is immediately recognized with such suspicions that OS itself is included in the movement of NASHLD to NASH to cause them moo misery in metabolic disorder. In fact, the major expenditure in the industry of ROS was perceived as an important expenditure in the field of liver fibrosis. The OS is related with numerous associated preoxidative jolts that are related with mitochondrial brokenness, which may be the predominant denominator of the OS. According to encourage signs, NASH OS climbing is due to mitochondrial DNA and protein variations from the norm. Changes in the complex - II, and reduced capacity of the electron transport chain (like superoxides or hydrogen peroxides) disturb the usual electron cross section and an electron spillage is bound to oxygen. As noted in 18, NASH has moo GSH peroxidase, MnSOD levels and catalase levels, therefore the capacity of mitochondria to lower ROS levels is reduced. [18]
Risk factors for non-alcoholic fatty liver disease: NAFLD is turning into an progressively basic wellbeing condition over the globe. Recently, the title has been voted to be renamed by a worldwide assemble of specialists by choosing NAFLD induction (broken) greasy liver disease (MAFLD). According to the most recent investigate, nonalcoholic greasy liver infection (NAFLD) probably a multiorgan infection including a combination of variable metabolic, environmental, hereditary and epigenetic causes. Of what degree are all spheres guilty for advancement of NAFLD is vague, perhaps various places of NAFLD may show some other examples of criticalness. [19]
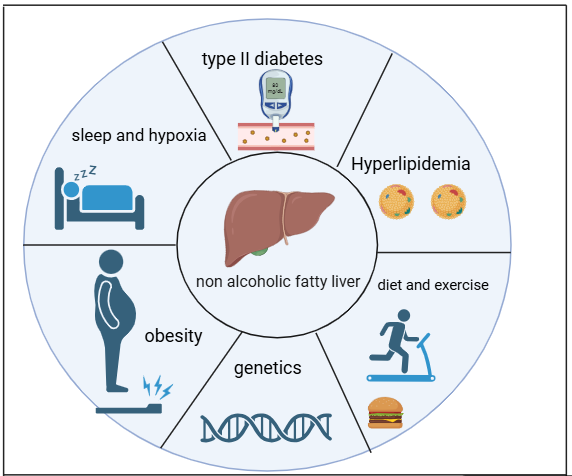
Obesity and metabolic syndrome:It really reminds us that the (otherwise PAGs focus on) weight plague is in fact the diligence of non-alcoholic greasy liver infection (NAFLD). One of the foremost vital hazard variables for NAFLD is weight, and the higher the body mass file (BMI), the better the possibility for worsening this condition. In a recent meta-analysis A appeared that NAFLD is much more common in pathologically stout group with the frequency of 78.09 % (95 % CI 64.37–87.55) with several methods. However, in overweight or corpulent people, the predominance was only 52.65% (95% CI, 48.20% 57.05%) and in nonadopted people, 12.01% (95% CI, 10.47% 13.75). Finally, central weight is associated with both NASH and dynamic fibrosis in NAFLD patients, as indicated by a review cohort ponder. Moreover, incline appeared to be strongly related with extreme liver fibrosis (OR 5.8; p = 0.004) and middle weight (> 102 cm and > 88 cm) in NAFLD patients, and middle weight (OR 4.2; p = 0.0001) and overweight or obese status (OR 3.6; p = 0.0001) in NAFLD patients in general, with more than 11,400 subjects included in metalweed such as that middle weight showed associations with metabolic syndrome related variables and plasma glucose levels (0.14). Since most ponders center around how weight is related with NAFLD hazard, particularly with regards to BMI. [20]
Diet and exercise: NAFLD calls for physical movement and weight misfortune and physical movement play an vital role in treatment of the condition. [21] However, appears inquire about that adherence to a calorie restricted count calorie, keeping up regular work out exercises and slow weight reduction of 5% to 10% can help in improving liver chemical levels and decrease liver fat. In reality, this equivalent 5 percent misadventure was related with better arranges of metabolic health and liver fat. Therefore, normal exercise can aggravate the metabolic issues in patients with NAFLD. [22, 23] Monophosphate activated protein kinase of adenosine (AMPK) is one of the most subjects within the decrease of liver fat. Oxygen consuming work out helps the muscles use the supplements to allow more movement on the muscle, as one would say. [24] In case you're encountering NAFLD, it's in any case prescribed to cut back on basic sugars all the more than it if there was ever a period to do it, since these individuals are frequently in charge of hyperplasmic lipids, expanded glucose in the blood, and expanded effronter levels. But it’s crucial that their slim down is moo and NO saturated fats are display because numerous of these animals have to negotiate with high cholesterol. Furthermore, meals of natural products and vegetables should be eaten. Other than that, do not disregard to stay away from liquor and also tobacco to minimize the dangers of heart from NAFLD [25]. Preparation and weight misfortune can, to a great extent, increase obent embed levels and diminish leptin and make the zona affront susceptible to corpulence. As such, there is a good correlation between affront resistance and adiponectin mirrors in patients with NAFLD, leading to these way of life changes truly being more significant. [26]
Hypoxia and sleep apnea: OSA is regularly identified with corpulence, affecting somewhere in the range of 2% and 4% of individuals in any case. This is where the rehashed breathing during rest is due to blockage of aviation routes. It has even been thought about have for this situation that there are individuals who have troublesome OSA with next predominance and seriousness of nonalcoholic steatohepatitis (NASH). [27] It demonstrates that scenes with low moo oxygen levels have the capacity to prompt preformation as a result of the upgrade of NASH at rest. For instance, they contemplate including creatures that documented indications of irritation driving to the part of fibrosis. This illustrates how these hypoxic scenes can worsen the change of basic fat list into severe liver disease, but do not specifically hurt the liver. Rest of the liver (OSA) is regularly associated to rest. [28,29]
NAFLD or non-alcoholic greasy liver infection: A metabolic infection that can influence the liver and add to raised cholesterol levels and increasing the probability in diabetes and developing. If sort 2 diabetes and NAFLD happen simultaneously, they could deteriorate the metabolic profile, making you extra possible for cardiovascular issues. However, the clinical-clinical implication and the actual of NAFLD in people with type 2 or prediabetic diabetes remains obscure, despite the fact that the relationship between NAFLD and type 2 disaccharide still remains elusive. There are thinks about that NAFLD patients have an expanded reflect of angiopoietin like protein 8 (ANGPTL-8). Mice with an change in ANGPTL-8 have lower plasma triglycerides, which might be explained by higher clearance of triglycerides because of increased lipoprotein lipase activity. Reflections on face of the relationship between plasma-ANGT-8 and liver fat mass in patients with NAFLD. Surprisingly, ANGPTL-8 is positively associated with liver lipid levels, regardless of an individual’s lean or having liver disease. Solid indicator of NAFLD seriousness is high serum levels of ANGTL-8. It may also be that the accumulated lipids in liver led to this. [30, 31, 32]
Clinical features and diagnosis: Most people with NAFLD do not have symptoms that warrant mention, however there are symptoms that are unclear, or even pain on the right side of the abdomen. In another sense generally, liver enzyme levels go up a little wrong, which includes an enlargement of gamma glutamyl transpeptidase and Alanine aminotransferase (old). Fatty liver can sometimes be imaged and the abnormal liver enzyme level will show up on imaging, and often a physician will make its diagnosis incorrectly. NAFLD may be found incidentally during abdominal surgery when the liver is enlarged or tall. NAFLD has only been diagnosed in a small number of people, and most of those with NAFLD will not have been diagnosed.
Imaging techniques: Stomach and ultrasound are the most fundamental of the broad methods used for subjective assessment of liver recoloring. Liver recoloring is a method made moderately accessible, precisely estimated with important info. Liver steatosis, vascular group, profound debilitating, liver brightness, and tall liver differentiate are a minimum of two occasions of the other two determinations of stomach ultrasound. US conclusion has a few disadvantages, including subjectivity, administration demands, moo affectability to situate in the middle of the wooden linchpin coloring, and lack of evaluation of steatosis. Yet, MRI is more costly and less common than it is more objective and sensitive to estimations of steatosis. [33]
Liver biopsy: Today the disease of nonalcoholic fatty liver illness (NAFLD) is assessed by liver biopsy. Most of which has been skipped because it is prohibited by the rule of diagnostics and filtration of the degree of damage other harmful liver and the filtration of Fibatoge, Fibertoge, Fibertoge, Fibertoge, Fibertoge, Fibertoge, Fibertoge, Fibertoge, and Fibertoge. Fibatozen. You are, however, a large standard for diagnosis, but liver biopsy is an intrusive method with actual risk and is limited because a pathologist's subjective assumptions have only as much weight as the suppositions translate. Furthermore, the fragment of parasite of the virion that is checked is really a moderately little part of the parasite in general harm. Also, a few non-invasive demonstrative disobedient and assessments for the appraisal of liver fibrosis, as well as discovery of rhino and liver recoloring. This area explains the points of interest and problems of each of these gadgets. [34] If NAFLD is identified, clinical prognosis strategies can be used to identify patients with fibrosis. These rules serve as a speedy, uncomplicated method in which risk-rated patients who may require a transfer from one expert to another would be in compliance. The data for liver fibrosis values comes from the METAVIR assessment system. F0 (no fibrosis), F1 (mild fibrosis), F2, (moderate fibrosis), F3 (advanced fibrosis) or F4 (frank cirrhosis according to a liver biopsy). [35]
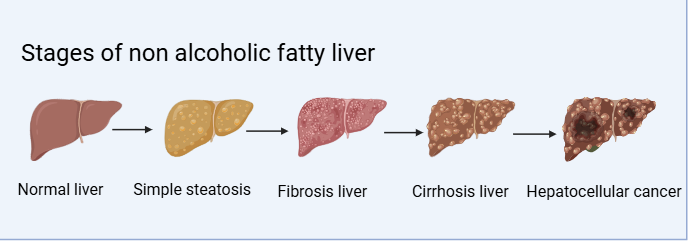
Simple Steatosis: These patients have steatosis alone or steatosis minimalizing non-severe concurrent lesions, and not qualifying as non-alcoholic steatohepatitis (NASH) NASH. It is also observed that these patients with steatosis probably have other cardiovascular or non-hepatic disease outcomes, and they have a increased risk of death in epidemiological studies. [36] In a small number of patients, steatosis and light are found simultaneously, including with spacious (enlarged) or larger hepatocytes of normal size or several inflammatory cells. This lesion is assumed in general to be NAFL, but it is not certain that this prediction is as cheap as pure steatosis. Some of these cases, in retrospect, have been slower than the NASH cases, while in fact developing more slowly and more slowly, but that these lesions can stabilize or reproduce. Discovery of lipid droplets in hepatocytes in 5% or less of hepatocytes is an optional limitation of the pathological classification of steatosis. The most common type of steatosis is usually the main one, but medium green steatosis (dominant large droplets or mixture of small and large droplets) can occur also. The core is displaced in hepatocytes that almost completely are encapsulated in large cutaneous steatosis by lipid vacuoles. In the worst boocytes, such cells may be similar. Appearance of one or more small vacuoles in the cytoplasm causes central steatosis. [38] Stomachemia is assessed on a simple four point scale 0 to 3. Calculate the proportion of hepatocytes with fatty acid fluid taking into consideration only macro and or mediocre steatosis. Normal (degrees 0) liver has less than 33% of fatty liver hepatocytes filled with fat. When steatosis reaches class 2 and 3 hepatocytes contain at least 34 or 66% of fat. [39]
Non-alcoholic steatopatitis:The natural history of NAFLD and NASH is still unknown; however, patients with NASH and steatohepatitis histologic patterns and progressive fibrosis have an extremely increased risk for endostage or death. Steatosis and steatosis have an etiology which is not known. An epidemiological data suggests there are two different entities which another can process through other and laterasis to the steatohepatitis. Indeed, the form of liver damage is steatohepatitis, as have been said earlier, and that means liver tissue must be examined. Although composition-based approaches based on clinical and biological information do exist, none is offered to subjects to demonstrate steatohepatitis or discriminate between pure steatosis and the disease. Thus, if the presence is detected by Nash, it is advisable that a liver biopsy is conducted. However, it is now widely accepted that to the diagnosis of steatosis, lobular inflammation and declaration of liver cell ballooning also is needed. If NASH is diagnosed, other histological features may be present, but they are not used. [40, 41, 42, 43]
Fibrosis: For the patients with non-alcoholic fatty liver disease (NAFLD), the important thing is whether there is high level of fibrosis. This prognostic characteristic depends on the patient outcomes and disease course. Several of these biochemical and clinical attributes have been used to develop several serological assessments of fibrosis. NAFLD Fibros Score (NFS), Bird, and FIB-4 are simple online service programs such as those to reduce the calculations for these tests. Commercial tests like Fibroktest, Fibroketer-NAFLD and Enanced Liver Fibrosis Score (ELF Test) provide a more comprehensive review. The split limits for these tests are used to maximize sensitivity and specificity, as well as to accurately identify and exclude advanced fibrosis. Thus, the applied strategy is based on screening for secondary mobility to care (in exclusion of huge fibrosis) with simple serological markers. Temporary elastography (TE) makes more detailed measurements. In this measurement, the liver tire measurements are measured as a testament to the amount of fibrosis. New developed imaging method is supersonic shear imaging (SSI) and acustic wave force impulse (ARFI) give equivalent results. Early transfer of severe fibrosis patients and targeted treatments provide healthcare workers an opportunity to improve patient outcomes. Indeed, NAFLD calls for extremely important taylor made care to account for each patient’s needs to accurately calculate risk. [44]
Hepatocellular carcinoma: The most common type of primary liver cancer is hepatocellular carcinoma (HCC), which inhibits morbid and mortality rates worldwide. Patients with chronic liver disease are more frequent, in particular among patients with liver disease due to hepatitis B and C virus, alcohol-induced liver disease and non-alcoholic fatty liver disease (NAFLD). The main reason for the increment in HCC is increased metabolic associated steatohepatitis (MASH), which includes type 2 diabetes and obesity. Through a multi stage process, chronic liver inflammation, fibrosis, and then cirrhosis, this process eventually results in HCC. Genetic and epigenetic change such as oxidative stress, involvement in Wnt/²-catenin signaling and TP53 mutations candictate hepatoma formation. Ultimately it brings to light a role in the progression of HCC through immune evasion, intestinal microbiomas and mitochondrial disorder. Because HCC is symptomatic only in late stages, there remains an early stage challenge in detection of this disease. Except for some blood markers such as DCP and alphafeto protein (AFP), imaging techniques such as MRI, CT scans, ultrasound, etc. are common in diagnostics. But since new biomarkers like circulating tumor DNA (CTDNA) and glypican-3 (GPC3) [45–48] can be looked up to improve accuracy, we showed that new biomarkers can assist in improving the accuracy.[45,46,47,48]
Treatment and Management of NAFLD: NAFLD management is based on changes in the nutrition and lifestyle, mainly in the changes of levels of physical activity. Indeed, continuous weight loss significantly reduces liver fat, improves metabolism health and slows the progression of the disease. [49.50.51.52]
Dietary Changes: Wearing clothes decreases caloric intake to 1,200–1,500 kcal/day while also allowing the reduction of 500–1,000 kcal/day to help people lose weight. The weight reduction of 3–10% brings health benefits to non-obese and obese people and hepatic steatosis and fibrosis improve when weight loss reaches ≥7–10%. Two diet strategies for liver fat prevention include low-carbohydrates combined with low-sugar diets to prevent liver fat accumulation and consuming Omega-3 polyunsaturated fatty acids found in flaxseeds and fish to improve insulin sensitivity while lowering liver fat based on meta-analyses. Regular coffee drinking also aids in reducing NAFLD and liver fibrosis severity.
Physical Activity: Regular physical activity strengthens all advantages that derive from nutritional interventions. Patients need to engage in strong intensity activities that total either 150 minutes per week or 75 minutes per week. The reduction of liver fat occurs through both aerobic and tolerance exercise with strength functioning as an essential component. NAFLD treatment reaches its most efficient point when patients combine dietary limitation with clean nutrition along with dedicated exercise routines. The interventions help improve insulin sensitivity and fight inflammation while halting disease evolution and deliver treatment which combines both effectiveness and non-medicinal elements.
Surgical interventions: Bariatric Surgery
Bariatric surgery can be utilized to treat obese individuals with non-alcoholic greasy liver disease (NAFLD). This may lead to long-term weight misfortune and rectification of metabolic issues such as affront resistance and cardiovascular malady. Two of the foremost well-known strategies, laparoscopic sleeve gastrectomy (LSG) and RYGB bypass (RYGB), decrease stomach measure, change absorption, and increment liver digestion system. Considers have appeared that bariatric surgery kills 56% of steatosis, makes strides swell generation by 49%, diminishes irritation by 45%, and relapse of fibrosis causes 25-40%. Compared to non-Asians, Asians by and large have the next determination of fibrosis and a better rate of steatosis. Long-term benefits include a diminished probability of movement of liver cirrhosis, a lower rate of cancer due to weight, and a decrease within the most imperative undesirable cardiovascular and liver occasions within the decade (8.5% vs. 8.5% vs. 8.5%. 15.7%) and 2.3% compared to 9.6%. Nevertheless, 12% of patients can compound or create NAFLD after surgery, with way of life and compliance with expanded reconnaissance being of foremost significance. All things considered, bariatric surgery remains one of the finest medicines for NAFLD, particularly in exceedingly corpulent patients. It is invaluable to combine with fitting postoperative care to altogether reestablish liver and metabolic control. [53]
Pharmacological therapies: The affront sensitizers are a class of drugs which opens the body's reaction to affront hormone, in particular the mindful one that fills your blood sugar. As medications for greasy liver sickness (NAFLD) and nonalcoholic steatohepatitis (NASH), affront sensitizers have been researched. Affront resistance harrows both NAFLD and NASH, a state in which the affronted cells remained safe. Lifted blood sugar concentrations cause the liver to damage and advance the development of greasy liver infection. Metformin is an affront sensitizer that has been under investigation as a medicate for NAFLD and NASH treatment indications. Because of its status as an affront sensitizer, metformin has been suggested as a possible treatment of NAFLD and NASH. By creating diminished affectability of the cells of the body to affront and creating diminished glucose generation of the liver it works. On the other hand, metformin may reduce in affront affectability and flare of the liver without being proven to be effective in the treatment of NASH. TZDs fall into the rapidly growing class of affront sensitizers that have to date been investigated as possible medicines for NAFLD and NASH. TZDs such as pioglitazone and rosiglitazone fortify a protein called peroxisome proliferator actuated receptor gamma (PPAR-gamma) which helps decrease liver aggravation and enhance insusceptibility to affront. This would seem to lessen liver irritation and rise the sensitivity to injury in people with NAFLD and NASH. They, that is surely, may have extremely severe side effects including edema, weight increase and greater chance of heart failure. We conclude that TZDs and metformin have been promising for affront sensitizers to improve affront affiability and decrease liver irritation in people with NAFLD and NASH. They are not exceptionally tough and may be destructive. Advance research would be needed in order to plan compelling and secure medications for the illnesses.[54]
Obeticholic Acid (OCA): If OCA treatment for steatohepatitis (which does not contain liquid obeticolic corrosive) is an artificial indication, then chenodeoxycholic corrosive (ordinarily grey corrosive) might be an indication of the human oversee just as the inhibition of the monooxygenase pathway, which is presumably a subjective indication. To their digestive orientation of cholesterol and glow, they seemed to have anticholestatic and hepatoprotective properties. OCA is a candidate for recovery for non-alcoholic steatohepatitis (NASH) with its anti-inflammatory and anti-fibrotic activity. Many clinical ponds were at the heart of the security and adequacy of the OCA. Treating patients in a stage 2A weight error-controlled study with OCA reduced liver stimulation and fibrosis in people with diabetes or nonalcoholic fatty liver disease advanced. Naturally, OCA displayed a certain degree of resilience in the treatment of Nash, which Stadium-2B-rock also demonstrated. In just over 283 test members, OCA was administered at a dose of 25 mg daily for 72 weeks. When 45% of patients treated with OCA on the number of patients focused without incremental fibrosis vs. 21% of patients treated with placebo, 45% was met as the main goal of consideration. Nonspecific treatments of OCA induced lower levels of fibrosis, steatosis, lobular stimulation and hepatocyte swelling in patients. The heap also lost weight and looked old on the OCA treated heap.
Ongoing Clinical Trials: And as of now, two preclinical or stage 3 think about for OCA are in development. In the inverse think about, the security and adequacy of OCA in sufferers of NASH balanced cirrhosis is considered, while in the continuation contemplate the NASH impact on fibrosis is seen. Data for the potential treatment of NASH OCA has been disseminated among the test more so and has ensued. [55]
Emerging therapies:
Peroxisome Proliferator-Activated Receptor Agonists for Non-Alcoholic Steatohepatitis Treatment
A nuclear receptor of the growth factor activated receptor (PPAR) in peroxisoma regulates a number of metabolic functions, including lipid metabolism, high eyelets of glucose, and inflammation. Three PPAR subtypes were determined: PPAR-alpha, PPAR-beta/delta and PPAR-gamma. Each of these subtypes has different roles and tissue symptoms. Lack of PPAR-alpha is associated with failure of solute transport and cryooxidation, expressed mostly in liver and brown adipose tissue. By increasing PPAR activity, lipid metabolism has been improved, inflammation has been reduced, and the mirror of inflammatory plasma cytokines reduced. Immune system and adipose system expression of PPAR-beta is responsible for the controlling of the immune system and improving insulin sensitivity (PPAR-beta/delta controls the metabolism of fat and carbohydrates). The new selective PPARî± modulator, Pemafibrat (K-877), has appeared advantageous in animal models of diseases associated with dyslipidemia, non-alcoholic fatty liver, induced hypercholesterolemia, induced prehepatitis, and induction of prehepatitis in animal models of NASH. Pemafibrat regulates glucose oxidation and induces fatty acid oxidation through effects on important target genes. Pemafibrat has also been shown in clinical studies to reduce plasma triglycerides, VLDL cholesterol, residual cholesterol and APOC III levels. Moreover, that Pemafibrat uses magnetic resonance elasticity to diminish liver tires without diminishing liver fat content has been proved. It is promising for nash treatment, but there should be side effects and severe renal venous thromboembolism to be carefully considered. It is not known whether pemafibrat can reverse histological damage and halt progression of NASH in further studies. After all, PPAR agonists in particular represent Pemafibrati, a promising therapeutic strategy for the management of Nash. Further studies in safety and efficacy profile are needed, however. [56]
Farnesoid X Receptor Agonists for NASH Treatment: One of the atomic receptors that plays an indispensable function in upkeeping metabolic same-metabolic illness is farnesoid X receptor (FXR). In the kidneys, liver, digestion tracts, and adrenal organs, bile acids begin to express FXR. Our data show that FXR agonists obstruct masses in body organs and the liver NF-B activated fiery reaction. Furthermore, it inhibits hilter kilter dimethylarginine (ADMA) acceptance that raises endogenous microorganism oxide quantities and manages coronary event. There have also been later ponders that FXR agonists have a place in the treatment of NASH. A couple of the messages have shown the two-fold LXR-alpha and FXR agonist that treats NAFLD liver fibrosis and hepatitis. A restoration methodology for NASH from FXR agonists is possibly capable. Through its focusing on on FXR, these agonists can advance forward in the face of affectability, restrict aggravation, and give command over the lipid and the digestion of the glucose framework. There is a need to help in assist investigate the potential of FXR agonists in the therapy of its NASH. [54]
Glucagon-Like Peptide-1 Receptor Agonists for NASH Treatment: The hormone that is, this is an Increist hormone, Glucagon Like Peptide 1 (GLP-1) helps direct blood glucose levels. GLP-1 receptor agonists diminish starvation, forestall liver fat arrangement, and improve run a risk. It too incurs vitality use and causes weight reduction. Others clinical consider have been that twofold GLP-1 and the glucose dependent insulinotrop peptide (GIP) receptor agonist tyldidatide are successful in treating non-alcohol susceptible steatohepatitis (NASH). It proceeds toward affront affectability and raises the amount of oboneeectin, a protein related to loss suppression, based on the affront relationship. Another GLP 1 receptor agonist that may be used in the treatment of Nash is semaglutid. It purges stomach, put a dent in the liver fat, and enhance affront sensitivity. Examples of possible medications for NASH come in the form of GLP-1 receptor agonists. A multidimensional approach to treatment of infection is described. It is comprised of weight reduction and insulin resistant hepatocyte fat collection. Side effects are queasiness, spewing and loose bowels, and for the most part well endured. GLP-1 receptor agonists must be completely investigated as a potential treatment of NASH. [57]
CONCLUSION:
In rundown, non-alcoholic greasy liver malady (NAFLD) has gotten to be a vital open wellbeing issue due to the expanding worldwide predominance of weight and metabolic disorder. Early intercession and treatment are critical since another liver infection chance is accessible, but the early arrange infection is regularly asymptomatic. In spite of the fact that way of life changes such as nourishment, work out, and weight misfortune stay the most bolster of treating non-alcoholic greasy liver disease, modern treatment methodologies such as medicine and bariatric surgery seem possibly treat the complexity of the illness. The weight he applies around the world requires open wellbeing intercessions to raise mindfulness and drive way of life changes. An intrigue approach including nutritionists, doctors and researchers ought to be included in viably handling this developing plague in case our information advances through NAFLD.
REFERENCES

Chandana K. B.*, U. Rajashekhar, Non-Alcoholic Fatty Liver Disease: A Review of Pathophysiology, Risk Factors and Therapeutic Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 448-462. https://doi.org/10.5281/zenodo.15132907
 10.5281/zenodo.15132907
10.5281/zenodo.15132907