
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of pharmacy, Rai university, Ahmedabad.
Nutraceuticals (bioactive food-derived compounds, supplements and functional foods) are widely used as adjuncts for preventing and managing type 2 diabetes (T2D) and for treating prediabetes. Growing clinical and preclinical evidence suggests several nutraceuticals — notably berberine, curcumin (turmeric), vitamin D, probiotics/prebiotics and certain polyphenols — may improve glycemic markers, insulin sensitivity and cardiometabolic risk factors. Evidence quality and consistency vary: some agents show promising randomized-trial data, others mixed or null results, and safety/drug-interaction considerations are important. This article summarizes the current evidence, mechanisms, safety, and practical recommendations. The prevalence of obesity is associated with many health-related problems. Currently, more than 300 million people are considered to be obese. According to the World Health Organization (WHO), by 2030, 87 and 439 million people will be affected in India and the world, respectively. Today, herbal medicines are gaining interest in the treatment of obesity and diabetes, because of their minimal side effects. Gymnemic acid - an active component isolated from Gymnema sylvestre - has anti-obesity and antidiabetic properties, decreases body weight and also inhibits glucose absorption. Several components extracted from Gymnema prevent the accumulation of triglycerides in muscle and liver, and also decrease fatty acid accumulation in the circulation. In this paper, an attempt has been made to review the effects of various extracts from Gymnema sylvestre in the regulation of carbohydrate and lipid metabolism in both animal and clinical studies. Lifestyle is the primary prevention of diabetes, especially type-2 diabetes (T2D). Nutritional intake of olive oil (OO), the key Mediterranean diet component has been associated with the prevention and management of many chronic diseases including T2D. Several OO bioactive compounds such as monounsaturated fatty acids, and key biophenols including hydroxytyrosol and oleuropein, have been associated with preventing inflammation and cytokine-induced oxidative damage, glucose lowering, reducing carbohydrate absorption, and increasing insulin sensitivity and related gene expression.
Diabetes mellitus, particularly type 2 diabetes, is a chronic metabolic disorder characterized by elevated blood glucose levels due to insulin resistance or deficiency. With its rising global prevalence, there is an urgent need for effective strategies that go beyond conventional pharmacological treatments. One promising approach is the use of nutraceuticals—bioactive compounds derived from food sources that offer health benefits, including disease prevention and therapeutic support.
Diabetes Mellitus (DM) is a major and increasing global health challenge. Type 2 diabetes (T2D) in particular involves insulin resistance, β-cell dysfunction, chronic hyperglycaemia and a host of vascular and metabolic complications. Traditional pharmacologic treatments are effective, but they have limitations including side-effects, cost, and incomplete mitigation of complications. This has led to growing interest in nutraceuticals – food-derived bioactive compounds (functional foods, phytochemicals, vitamins/minerals, herbal extracts) – as complementary or adjunctive strategies for prevention or management of diabetes. For example, one review notes: “plant polyphenols … have been proposed as effective supplements for diabetes management and prevention of its long-term complications.
1.1 Sources of Nutraceuticals
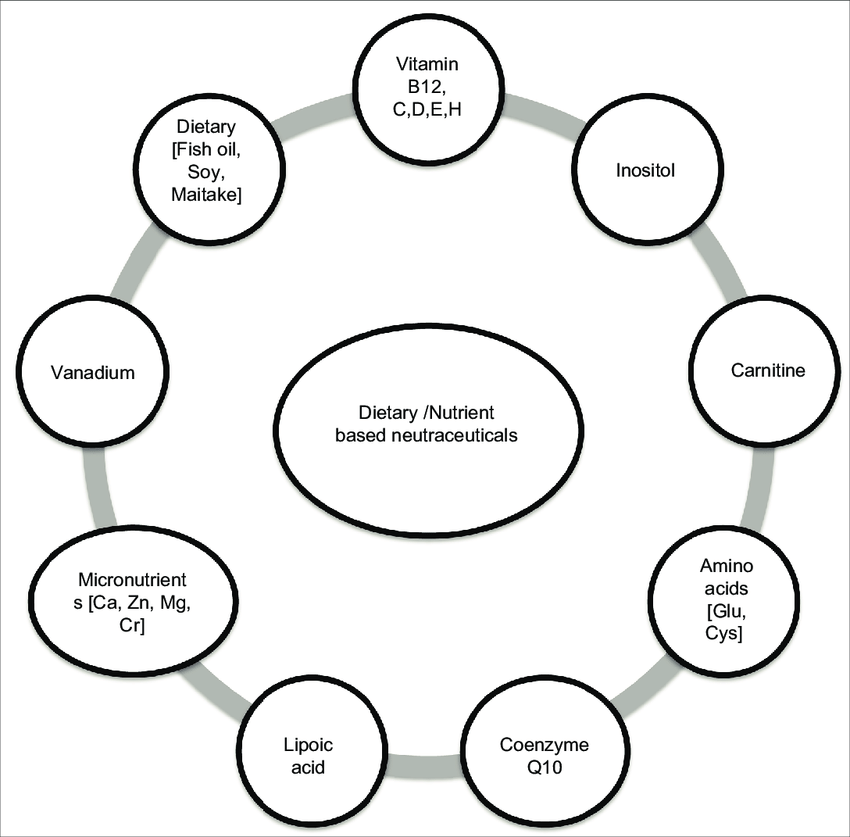
Nutraceuticals are naturally occurring substances found in foods, herbs, and dietary supplements that possess medicinal properties. They include:
•Vitamins and minerals (e.g., vitamin D, magnesium)
•Phytochemicals (e.g., flavonoids, polyphenols)
•Herbal extracts (e.g., cinnamon, fenugreek, bitter melon)
•Functional foods (e.g., probiotics, omega-3-rich foods)
These compounds can modulate biological processes and help maintain metabolic balance, making them valuable tools in diabetes care.
1.2 Pathophysiological Rationale for Nutraceutical Use in Diabetes
To understand how nutraceuticals might help, it helps to summarise key mechanisms in T2D and how bioactives can intervene:
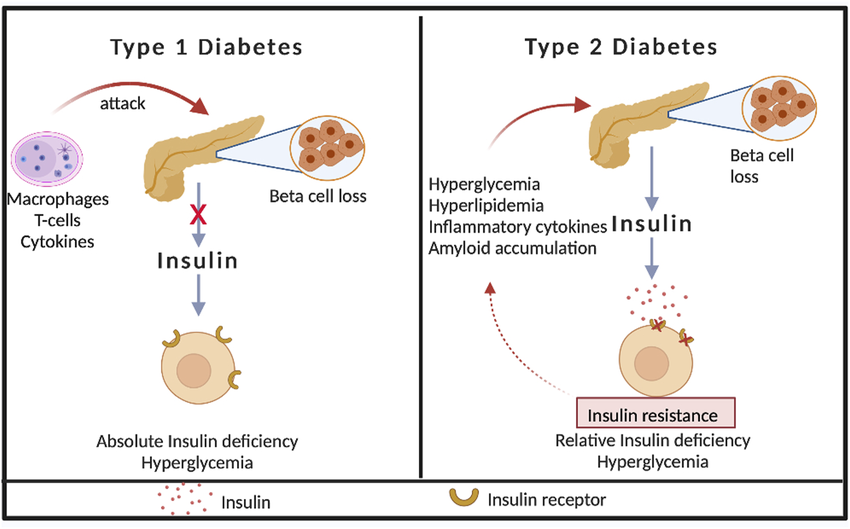
•Insulin resistance/β-cell dysfunction: In T2D the body’s tissues respond less to insulin, and pancreatic β-cells gradually fail to produce enough insulin.
•Oxidative stress & inflammation: Persistent hyperglycaemia and lipotoxicity trigger oxidative stress, activation of NF–κB, cytokines, and contribute to tissue damage/sequelae. SpringerLink+1
•Glucose absorption & transport dysregulation: Impairments in GLUT transporters, increased hepatic gluconeogenesis, and decreased glucose uptake all contribute.
•Advanced glycation end-products (AGEs), endothelial dysfunction, dyslipidaemia: These lead to micro- and macro-vascular complications.
•Gut microbiota and epigenetic influences: Emerging evidence links the gut flora, diet and nutraceutical compounds to glucose metabolism and insulin sensitivity.
Nutraceuticals can intervene at various points: improve insulin signalling, enhance antioxidant capacity, reduce inflammation, modulate glucose absorption, influence gene expression or enzyme activity (e.g., AMPK activation, PPAR modulation) and improve β-cell survival.
1.3 Evidence for Nutraceuticals in Diabetes Prevention & Management
Here we examine key categories of nutraceuticals and summarise the evidence, benefits and limitations.
Phytochemicals & Plant-derived Bioactives
•Polyphenols (flavonoids, stilbenes, phenolic acids) from foods such as green tea, berries, pomegranates, cinnamon, etc. One review states: “Plant polyphenols … based on in vitro studies, animal models and some clinical trials, have been proposed as effective supplements for diabetes management and prevention of its long-term complications.”
•Specific herbs/spices: For example, cinnamon (Cinnamomum zeylanicum), fenugreek (Trigonella foenum graecum), bitter melon (Momordica charantia) have been studied in diabetic contexts. For instance one review mentions bitter gourd, cinnamon, tulsi (Ocimum sanctum) and fenugreek.
•Mechanisms: inhibition of carbohydrate-digesting enzymes (α-glucosidase/α-amylase), increased GLUT4 translocation, AMPK activation, reduced oxidative stress, decreased inflammatory cytokines.
Evidence summary: Some small human trials and many preclinical studies show beneficial effects—reductions in fasting plasma glucose (FPG), HbA1c, improved lipid profiles. For example, one review summarising 18 studies of ~21 nutraceuticals found that many lowered FPG and HbA1c significantly (p < 0.05) in T2D.
Limitations: Many studies are small, heterogeneous in design (dose, duration, population), sometimes lacking placebo control. Human outcome data are less robust. The review on dietary polyphenols notes that “further investigations using human clinical studies are needed to confirm the beneficial effects”.
Micronutrients (Vitamins & Minerals)
•Vitamins such as C, D, E have been studied. For example, vitamin D deficiency is associated with insulin resistance and β-cell dysfunction. One narrative review mentions vitamins C, D, E in the context of improving insulin sensitivity and lowering blood sugar/lipids.
•Minerals such as zinc, chromium, magnesium have also been implicated in glucose metabolism. For instance, chromium supplementation has been proposed but results remain equivocal.
Evidence summary: Some association studies show low vitamin D or magnesium levels correlate with higher diabetes risk. Supplementation trials yield mixed results—some improvement in glycaemic indices in deficient patients, but not consistent across the board.
Limitations: Dosing, form (bioavailability), baseline nutrient status, and confounding lifestyle factors make interpretation difficult. Supplementation is not a substitute for diet and lifestyle.
Functional Foods, Dietary Fibre, Fatty Acids
•Dietary fibre (soluble & insoluble) helps modulate post-prandial glucose, slow carbohydrate absorption, improve insulin sensitivity. One review mentions resistant dextrin reducing FPG, HbA1c and CRP in T2D. nutrafoods.eu
•Omega-3 fatty acids, monounsaturated fats, etc may improve lipid profiles, reduce inflammation, and indirectly modulate insulin sensitivity. For example, a recent article notes omega-3 fatty acids show potential in sensitising insulin and ameliorating diabetic complications. Bentham Science
Evidence summary: There is moderate evidence that diets rich in whole grains, legumes, low-GI foods and good fats improve metabolic outcomes. However, isolating the effect of a single “nutraceutical” from the broader diet is challenging.
Limitations: The effect size may be modest; compliance and long-term studies are fewer; the interplay with overall diet/lifestyle is complex.
1.4 Prevention of Diabetes:
While most studies focus on management of established diabetes, there is growing interest in prevention of progression from pre-diabetes (impaired fasting glucose/impaired glucose tolerance) to T2D.
•Some evidence suggests that nutraceuticals may delay or reduce risk of T2D development via improving insulin sensitivity, reducing oxidative stress, improving β-cell function.
•However, robust RCTs in large cohorts specifically for prevention are sparse. One review of nutraceuticals in chronic disease management noted diabetes prevention as a target, but cautioned about evidence strength. PubMed
•Given the multifactorial origin of T2D (genetics, obesity, inactivity, diet), nutraceuticals should be viewed as adjuncts, not replacements for lifestyle interventions.
1.5 Practical Considerations & Safety
•Dosage & standardisation: Bioactive compounds in herbs/foods vary widely in concentration, purity and bioavailability. Many studies use standardized extracts; commercial supplements may differ.
•Interactions: Some nutraceuticals may interact with anti-diabetic medications (e.g., risk of hypoglycaemia if added to insulin or sulfonylureas). Always require medical supervision.
•Quality & regulation: Nutraceuticals are less strictly regulated than pharmaceuticals in many regions; issues of contamination, adulteration, mislabelling exist.
•Evidence grade: Much of the evidence is pre-clinical or small-scale human studies. Long-term outcome data (micro-/macro-vascular endpoints) are limited.
•Holistic approach: Nutraceuticals are most effective in the context of comprehensive care – diet modification, exercise, weight control, medication as needed. They are not “magic bullets”.
•Individual variability: Baseline nutrient/status, genetics, gut-microbiome, disease stage all influence response. Precision-nutrition approaches may become relevant.
2. CONCLUSIONS
The concept of nutraceuticals in diabetes prevention and management is promising: bioactive food-derived compounds can target multiple pathophysiological mechanisms (oxidative stress, inflammation, glucose transport, insulin signalling).
•Several categories (plant polyphenols, herbal extracts, micronutrients, dietary fibre/fats) show positive effects on glycaemic control, insulin sensitivity, and some metabolic parameters in people with T2D.
•The evidence for prevention of diabetes is less robust, though biologically plausible.
•Key caveats: heterogeneity of studies, small sample sizes, variation in dose/form, lack of long-term outcomes and standardisation.
•For practitioners and patients: nutraceuticals may serve as adjunctive tools, especially in early disease or pre-diabetes, but should not replace standard of care (diet, lifestyle, pharmacotherapy when indicated).
•Future directions: larger, well-designed RCTs with standardised preparations; dose-finding studies; long-term follow-up on complications; exploration of combination “poly-nutraceutical” (synergistic) approaches; integration of nutraceutical use into precision nutrition/personalised medicine paradigms.
REFERENCES

Navinraj Mourya*, Dhivar Priti Kumari R., Nutraceuticals in Diabetes Prevention and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 3767-3775 https://doi.org/10.5281/zenodo.17697448
 10.5281/zenodo.17697448
10.5281/zenodo.17697448