1,2Columbia Institute of Pharmacy, Tekari, Near Vidhansabha Road, Raipur-493111, Chhattisgarh, India
3Sant Gahira Guru Vishwavidyalaya Sarguja Ambikapur, (C.G.), India 497001
4Sita Ram Kashyap College of Pharmacy, Rahod, Janjgir Champa, Chhattisgarh, 495556, Chhattisgarh, India
Background: While structured caloric restriction can improve metabolic health, excessive or prolonged dietary restriction (“over-dieting”) is increasingly prevalent due to aesthetic, social, and clinical pressures. Emerging evidence indicates that chronic energy deprivation may paradoxically exacerbate metabolic dysfunction and promote multisystem pathology Objective: This review critically evaluates the pathophysiological mechanisms, endocrine adaptations, pharmacological implications, and systemic consequences of excessive dietary restriction, integrating narrative synthesis with systematic trend-based evaluation (2020–2025).Methods: A structured literature search was conducted in PubMed, Scopus, and Web of Science (January 2020–January 2025). Keywords included “caloric restriction,” “over-dieting,” “metabolic adaptation,” “hypothalamic dysfunction,” “HPA axis,” “insulin resistance,” “gut microbiome,” and “nutritional deficiency.” Inclusion criteria comprised peer-reviewed human and translational studies. Data were synthesized thematically.Results: Excessive caloric restriction induces adaptive thermogenesis, neuroendocrine dysregulation (HPT, HPA, HPG axes), mitochondrial stress, micronutrient deficiencies, and gut microbiome alterations. These alterations contribute to metabolic inflexibility, sarcopenia, reproductive dysfunction, cardiovascular remodeling, neuropsychiatric disturbances, and immune suppression. Pharmacological agents such as GLP-1 receptor agonists and appetite suppressants may exacerbate nutrient deficits when combined with extreme restriction.Conclusion: Over-dieting represents a clinically under-recognized contributor to metabolic and systemic disease. Personalized, physiologically aligned dietary strategies and careful pharmacological monitoring are essential to prevent long-term harm
Caloric restriction has historically been associated with longevity benefits and metabolic improvements. However, the global rise in restrictive dieting behaviors-driven by obesity epidemics, social media aesthetics and pharmacologically assisted weight loss-has led to an increase in excessive or prolonged dietary restriction beyond physiological thresholds.(1) Recent epidemiological trends indicate that up to 40-60% of adults engage in repeated dieting cycles, often involving severe caloric deficits (<800-1,000 kcal/day) without clinical supervision.(2,3) While short-term weight loss may occur, accumulating evidence suggests paradoxical metabolic consequences including adaptive thermogenesis, endocrine suppression and metabolic inflexibility.(4) This review synthesizes emerging data (2020-2025) to elucidate the mechanistic basis and systemic implications of over-dieting.(5)
2. Methodology
2.1 Search Strategy
A systematic trend-based literature search was performed across PubMed/MEDLINE, Scopus, and Web of Science to identify relevant studies published between January 2020 and January 2025. Boolean search strategies combined key terms including:(6)
2.2 Inclusion Criteria:
2.3 Exclusion Criteria
3. Pathophysiological Mechanisms of Over-Dieting
3.1 Adaptive Thermogenesis and Metabolic Suppression
Severe caloric restriction induces a disproportionate decline in resting energy expenditure (REE) that exceeds the reduction expected from weight loss alone, a phenomenon termed adaptive thermogenesis.(7) This metabolic adaptation is characterized by decreased circulating triiodothyronine (T3) concentrations, attenuation of sympathetic nervous system activity and alterations in mitochondrial efficiency that collectively reduce energy expenditure.(8) When sustained over time this suppressed metabolic state enhances energetic efficiency and predisposes individuals to accelerated fat accumulation and weight regain upon refeeding.(9)
3.2 Hypothalamic-Pituitary-Thyroid (HPT) Axis Dysregulation
Prolonged caloric restriction decreases leptin signaling, which in turn suppresses TRH and TSH secretion along the hypothalamic-pituitary-thyroid axis.(10) This suppression can lead to low T3 syndrome and symptoms such as cold intolerance, bradycardia, and fatigue; if sustained, it may resemble subclinical hypothyroidism due to persistent HPT axis suppression.(11)
3.3 Hypothalamic-Pituitary-Adrenal (HPA) Axis Activation
Energy deprivation stimulates sustained activation of the hypothalamic-pituitary-adrenal axis, leading to increased cortisol secretion. Elevated cortisol promotes central adiposity, enhances skeletal muscle proteolysis, induces insulin resistance and accelerates bone resorption. Consequently, persistent hypercortisolemia during chronic caloric restriction may contribute to the emergence of metabolic syndrome-like characteristics and broader systemic metabolic dysregulation.(12)
3.4 Reproductive Axis Suppression (HPG)
Reduced circulating leptin and insulin levels during prolonged energy deficiency disrupt hypothalamic gonadotropin-releasing hormone (GnRH) pulsatility, leading to suppression of the hypothalamic-pituitary-gonadal (HPG) axis. Clinically, this manifests as amenorrhea in females, decreased testosterone levels in males, impaired fertility and progressive reductions in bone mineral density. This constellation of findings closely parallels the pathophysiology of functional hypothalamic hypogonadism associated with chronic energy imbalance.(13)
3.5 Mitochondrial Dysfunction and Oxidative Stress
Excess restriction may reduce mitochondrial biogenesis and increase ROS production due to nutrient insufficiency, impairing metabolic flexibility.(14)
Very-low-calorie diets reduce microbial diversity and short-chain fatty acid production, affecting: Immune regulation, Insulin sensitivity, Gut barrier integrity.(15)
3.7 Micronutrient Deficiencies
Prolonged excessive dietary restriction is frequently associated with deficiencies in essential micronutrients, including iron, vitamin B12, vitamin D, zinc, and essential fatty acids. These deficiencies contribute to clinically significant consequences such as iron-deficiency anaemia, peripheral neuropathy, impaired immune competence, reduced bone mineralization and accelerated sarcopenia, thereby compounding the systemic impact of chronic energy deprivation.(16)
4. Systemic Consequences
4.1 Metabolic Disease Risk
Paradoxically, severe dietary restriction may exacerbate metabolic dysfunction by increasing insulin resistance, promoting preferential visceral fat regain and reducing lean body mass, thereby adversely altering body composition despite reduced caloric intake.(17)
4.2 Cardiovascular Effects
Severe and prolonged energy restriction can produce significant cardiovascular complications, including reduced cardiac muscle mass due to myocardial atrophy, electrolyte imbalances that impair normal cardiac conduction and-particularly in extreme cases-QT interval prolongation, increasing the risk of arrhythmias and sudden cardiac events.(18)
4.3 Neuropsychiatric Implications
Chronic energy restriction is associated with significant neuropsychological disturbances, including heightened anxiety and depressive symptoms, cognitive impairment and the development of obsessive, food-focused behaviors that reinforce maladaptive eating patterns.(19)
5. Pharmacological Perspectives
5.1 GLP-1 Receptor Agonists
Although effective for obesity management, combining such therapy with extreme dietary restriction may increase the risk of excessive lean mass loss, micronutrient deficiencies and Hypoglycemia in susceptible individuals.(20)
5.2 Appetite Suppressants and Sympathomimetics
Appetite suppressants and sympathomimetic agents may aggravate physiological stress responses by elevating cortisol levels and worsening electrolyte imbalances, thereby increasing the risk of metabolic and cardiovascular complications.(21)
5.3 Metformin and SGLT2 Inhibitors
In undernourished individuals, the use of metformin and SGLT2 inhibitors may further exacerbate existing energy deficits and, although uncommon, increase the risk of ketoacidosis, particularly in metabolically vulnerable patients.(22)
6. Figures (Conceptual Diagrams)
(Figure 1 illustrates the integrated neuroendocrine cascade triggered by chronic caloric deficit. Prolonged energy restriction reduces adipose tissue mass and circulating leptin levels, leading to hypothalamic dysregulation. This central adaptation disrupts three major endocrine axes: suppression of the hypothalamic-pituitary-thyroid (HPT) axis, activation of the hypothalamic–pituitary–adrenal (HPA) axis and suppression of the hypothalamic-pituitary-gonadal (HPG) axis. Collectively these hormonal alterations drive widespread systemic consequences, including metabolic suppression, insulin resistance, sarcopenia and bone loss. Figure 2 presents a systemic impact model of prolonged dietary restriction, highlighting the bidirectional interactions between central neuroendocrine adaptations and peripheral organ systems. Dietary restriction initiates hypothalamic-mediated alterations, including activation of the HPA axis and suppression of the HPT and HPG axes, resulting in elevated cortisol, reduced thyroid hormone (T3), decreased sex hormones and increased inflammatory signaling. These central changes propagate to multiple organs, contributing to muscle loss and impaired anabolic signaling, bone loss and reduced density, hepatic metabolic alterations, gut atrophy and dysbiosis, and cardiac atrophy with diminished contractile function. The figure emphasizes the integrated, multisystem nature of chronic energy deficiency.)
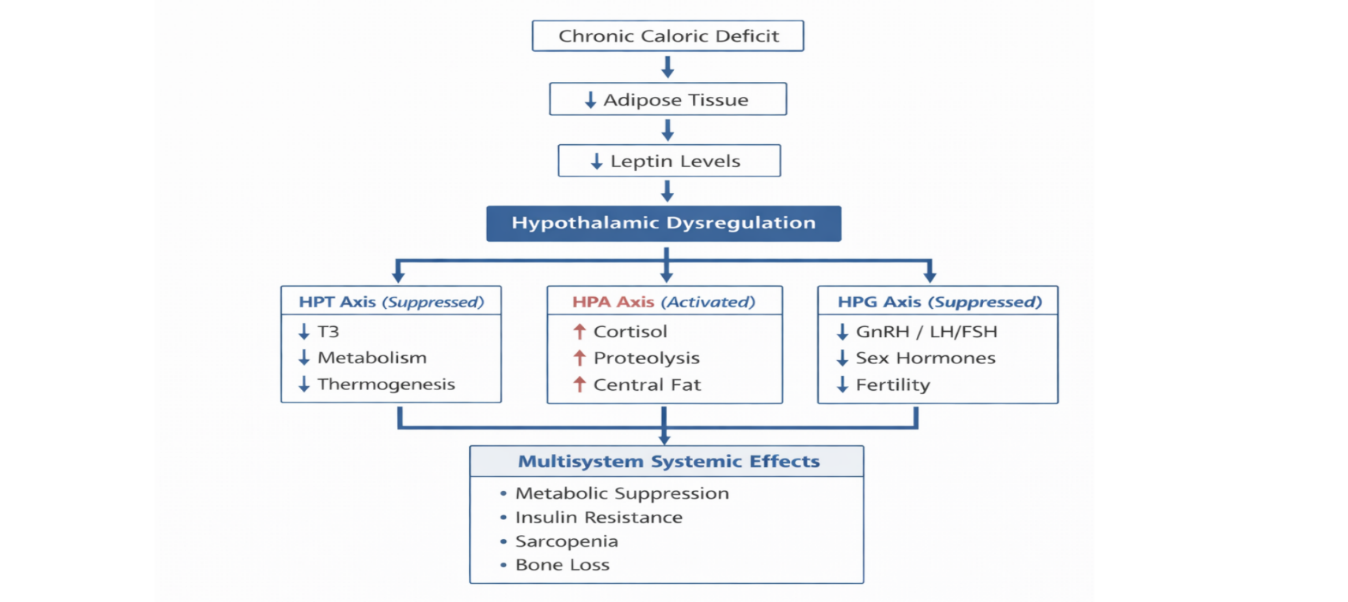
Figure 1: Neuroendocrine Cascade in Excessive Caloric Restriction
[Schematic representation of the neuroendocrine adaptations to chronic caloric deficit. Prolonged energy restriction reduces adipose tissue mass and circulating leptin levels, leading to hypothalamic dysregulation. This central disruption alters three major endocrine axes: suppression of the hypothalamic-pituitary-thyroid (HPT) axis resulting in decreased triiodothyronine (T3), reduced metabolic rate and diminished thermogenesis; activation of the hypothalamic-pituitary-adrenal (HPA) axis characterized by elevated cortisol, enhanced proteolysis, and central fat redistribution; and suppression of the hypothalamic-pituitary-gonadal (HPG) axis leading to reduced gonadotropin secretion, decreased sex hormones, and impaired fertility. Collectively, these neuroendocrine alterations contribute to multisystem systemic effects, including metabolic suppression, insulin resistance, sarcopenia, and bone loss.]
Description: Flow diagram showing caloric deficit → leptin reduction → HPT, HPA, HPG axis dysregulation → systemic effects.
Caption: Integrated neuroendocrine response to chronic energy deficiency.
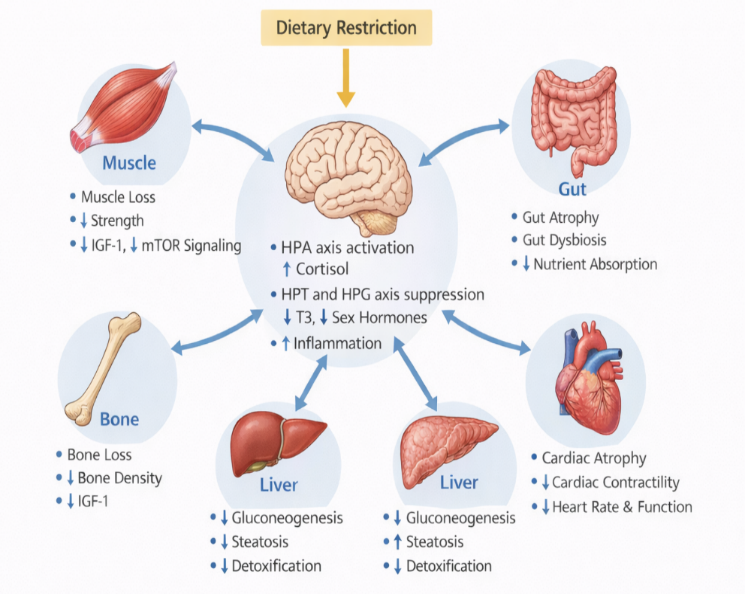
Figure 2: Systemic Impact Model of Prolonged Dietary Restriction
[Schematic illustration of the multisystem effects of chronic dietary restriction. Central neuroendocrine adaptations-characterized by activation of the HPA axis (↑ cortisol) and suppression of the HPT and HPG axes (↓ T3, ↓ sex hormones, ↑ inflammation)-mediate downstream effects across peripheral organs. These include muscle loss and reduced anabolic signaling, bone loss and decreased bone density, impaired hepatic metabolism, gut atrophy and dysbiosis and cardiac atrophy with reduced contractility. Arrows indicate bidirectional interactions between central and peripheral systems.]
Description: Multiorgan interaction map (brain, muscle, bone, gut, liver, heart).
Caption: Multisystem consequences of prolonged dietary restriction.
7. Tables
Table 1: Mechanistic Overview of Over-Dieting
|
Mechanism |
Molecular Mediators |
Clinical Outcome |
ReF. |
|
Adaptive thermogenesis |
↓T3, ↓SNS |
Weight regain |
(23) |
|
HPA activation |
↑Cortisol |
Muscle loss |
(24) |
|
HPG suppression |
↓GnRH |
Amenorrhea |
(25) |
|
Microbiome shift |
↓SCFA |
Insulin resistance |
(26) |
Table 2. Pharmacological Interactions
|
Drug Class |
Benefit |
Risk in Over-Dieting |
Ref. |
|
GLP-1 agonists |
Appetite reduction |
Lean mass loss |
(27) |
|
SGLT2 inhibitors |
Glycemic control |
Ketoacidosis risk |
|
|
Metformin |
Insulin sensitization |
GI malabsorption |
8. Abbreviations
BMI - Body Mass Index
GLP-1 - Glucagon-Like Peptide-1
GnRH - Gonadotropin-Releasing Hormone
HPA Axis -Hypothalamic–Pituitary–Adrenal Axis
HPG Axis - Hypothalamic–Pituitary–Gonadal Axis
HPT Axis -Hypothalamic–Pituitary–Thyroid Axis
QT Interval - Interval Between Q Wave and T Wave on Electrocardiogram
REE-Resting Energy Expenditure
ROS - Reactive Oxygen Species
SCFA - Short-Chain Fatty Acids
SGLT2 - Sodium-Glucose Cotransporter-2
SNS - Sympathetic Nervous System
T3 - Triiodothyronine
TRH - Thyrotropin-Releasing Hormone
TSH - Thyroid-Stimulating Hormone
9. Future Perspectives and Research Gaps
CONCLUSION
Excessive dietary restriction induces complex neuroendocrine adaptations that may paradoxically predispose individuals to metabolic dysfunction and systemic disease. While caloric restriction remains a powerful therapeutic tool, its overuse without physiological alignment carries substantial risks. Clinical practice must transition from aggressive weight-loss paradigms toward metabolically protective, individualized approaches.
Declaration:
Ethics approval and consent to participate:
This article is a narrative review and does not involve any experimental studies conducted on human participants or animals. Therefore, ethical approval and informed consent were not required.”
Clinical Trial No:
This manuscript is a review article and is not associated with any clinical trial; therefore, clinical trial registration is not applicable.
Consent for publication:
This manuscript does not include any individual participant data; therefore, consent for publication is not applicable
Availability of data and material:
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the preparation of this review
Funding:
The authors received no funding for this manuscript.
Declaration of competing interest: The authors declare no conflict of interest.
Acknowledgements:
The authors express their sincere gratitude to the Principal of Columbia Institute of Pharmacy, Raipur, Chhattisgarh, India, for providing the necessary infrastructural and library facilities to support the completion of this review
REFERENCES

Shiv Kumar Bhardwaj, Trilochan Satapathy, Khemkaran Ahirwar, Manmohan singh Jangdey, Over-Dieting and Excessive Dietary Restriction Pathophysiological Mechanisms, Pharmacological Perspectives, and Their Role in Metabolic and Systemic Diseases - A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3024-3032. https://doi.org/10.5281/zenodo.18697734
 10.5281/zenodo.18697734
10.5281/zenodo.18697734
