1 Department of Pharmacy Practice, JSS College of Pharmacy, JSS Academy of Higher Education and Research, Ooty, Tamil Nadu, India
2 Department of Medical Oncology, Gleneagles Global Hospital, Chennai, Tamil Nadu, India.
Paclitaxel is an anticancer taxane-based agent used in the adjuvant therapy of the breast cancer of the HER2-positive type. Paclitaxel is easily digestible by the majority of patients. Nonetheless, some cases of severe pulmonary complications inclusive of interstitial pneumonitis and ARDS have been reported particularly in patients who have preexisting respiratory conditions. We introduce a case of a 62-year -old female of postmenopausal age having carcinoma of the left breast, pT2 pN0 cMx. Her breast cancer was estrogen receptor positive, progesterone receptor positive and HER2 positive. Significant in her past medical history includes the underlying interstitial lung disease and severe ARDS, the treatment of which necessitated prone ventilation and tracheostomy which the patient was currently recovering. Her ground-glass opacities and interstitial thickening of the septa showed in both lungs as a result of her baseline imaging. The patient was operated in the form of breast-conservation surgery and placed on paclitaxel, carboplatin, and trastuzumab chemotherapy. Although the patient was initially stabilized clinically after the first round of chemotherapy, there was a high risk of the patient developing respiratory complications due to underlying lung disease. It may be difficult to distinguish between pneumonitis caused by paclitaxel and infection, or exacerbation of ILD. The case highlights the necessity of personal evaluation of advantages and risks of taxane-containing chemotherapy and close observation of the patients having the respiratory disease
Paclitaxel, a chemotherapeutic agent which is derived from the bark of the North American yew tree, Taxus brevifolia, has been used in ovarian and breast cancer treatment [1]. Moreover, the mechanisms of PTX action associated with the inhibition of tumor growth can act on different levels. In these studies, PTX initiated a cascade of signaling pathways resulting in programmed cell death [2,3]. The cellular mechanism of paclitaxel involves inducing mitotic block by stabilizing microtubules, thereby reducing the dynamic nature of these cytoskeletal structures [4].Common adverse effects are neutropenia, alopecia, peripheral neuropathy, nausea with vomiting, arthralgia, myalgia, and hypersensitivity reactions [5,6]. Paclitaxel-induced pneumonitis (PIP) is a very rare, poorly characterized, and potentially life-threatening complication of paclitaxel therapy with an estimated incidence of 0.73 - 12% [7,8]. Possible risk factors of PIP include pre-existing interstitial lung disease (ILD), 12-cycle vs. 4-cycle dosing regimen, and tumor type (presuming lung cancer patients may have lower pulmonary reserves) [7,9].The existing evidence shows that cases of pulmonary exacerbation with paclitaxel in their patients with already existing interstitial lung disease (ILD) and recent acute respiratory distress syndrome (ARDS) receiving adjuvant treatment of HER2-positive breast cancer are small. We offer an example of a patient with a history of ILD and current ARDS who demonstrated acute respiratory exacerbation in the nearest future after the beginning of chemotherapy with paclitaxel. The case demonstrates the danger of lung toxicity due to taxane in patients whose lung functions are already compromised and the need to determine risk-benefit individually. The patient provided informed consent regarding the publication of this case report by means of a written informed consent.
CASE PRESENTATION:
The patient was a 62-year-old postmenopausal female with a background of interstitial lung disease (ILD) and has recently developed severe acute respiratory diseases syndrome (ARTS), with a history of left malignancy in the breast, which she would like to be addressed further. On 16 December 2025, she had been placed on the fourth round of prone position ventilation and tracheostomy because of ARDS-related respiratory failure that was also progressing slowly. She had comorbid conditions of diabetes mellitus. An external MRI of the both bilateral breasts that followed showed a size of 3.8 × 2.8 cm lesion in upper outer quadrant of the left breast with spiculation and mild shrinkage of nipple-areolar complex. On the fine-needle aspiration cytology, invasive ductal epithelial cells were detected. PET-CT done on the entire body on 20 December 2025 was able to show a heterogeneously enhancing lesion as lobulated in the upper outer quadrant of the left breast and a metabolically active left axillary lymph node, which was very suggestive of nodal metastasis. Further, the pulmonary fibrotic interstitial septal thickening was of low-grade metabolically active type with a confluent ill-defined ground-glass opacities that is characteristic of the inflammatory ILD, and was predominant in the lower lobes (Table 1).
Table 1: Pulmonary and Cardiac Evaluation
|
Investigation |
Findings |
|
CT Chest (Outside) |
Multiple peribronchial consolidations with adjacent ground-glass opacities; diffuse bilateral peribronchial thickening; mild bilateral pleural effusion |
|
PET-CT (Lung Findings) |
Fibrotic interstitial septal thickening with confluent ground-glass opacities in both lungs, predominantly involving the lower lobes |
|
Echocardiography (13.01.2026) |
Left ventricular ejection fraction (LVEF) 64%; mild left ventricular diastolic dysfunction; mild pericardial effusion; no regional wall motion abnormality |
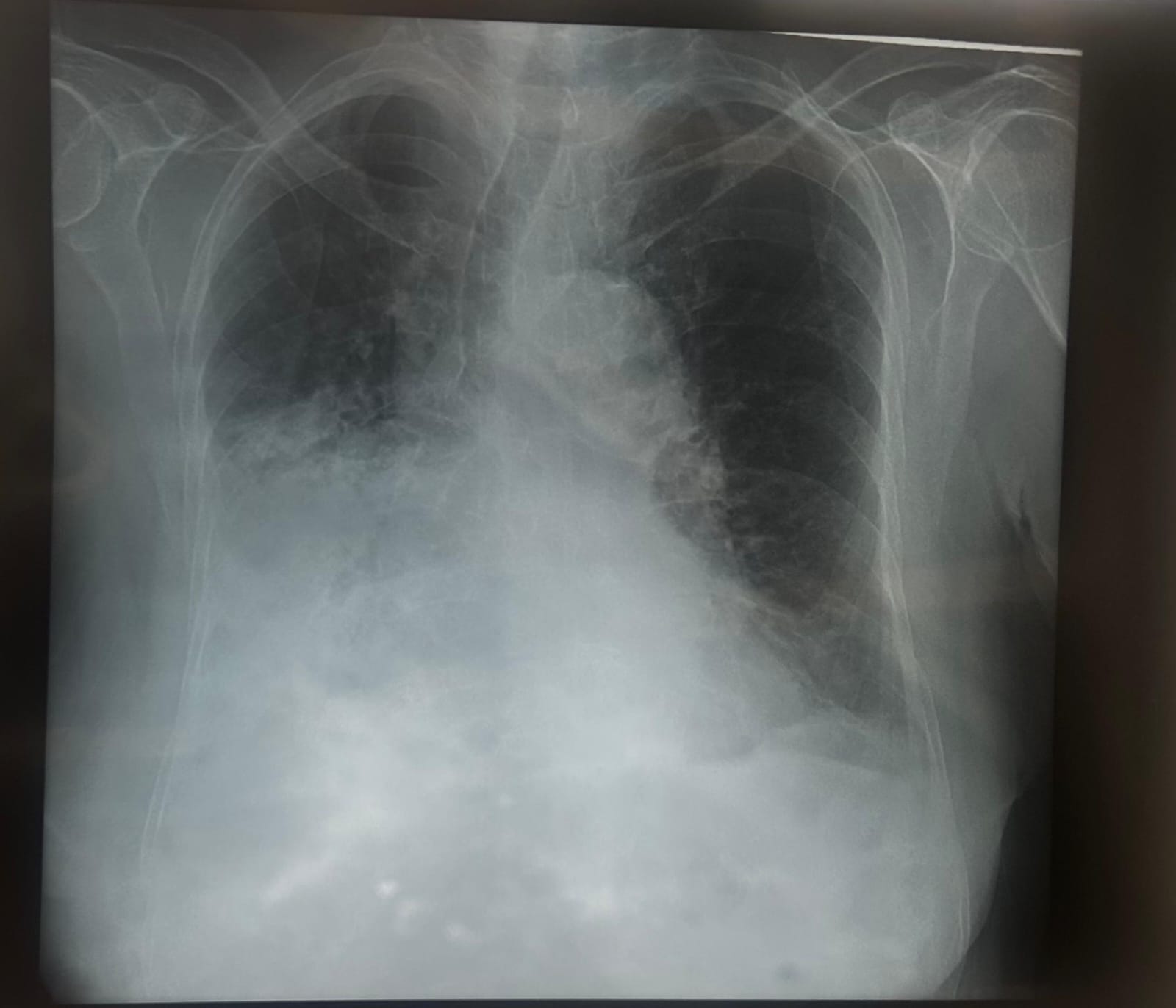
Figure 1: Chest X-ray
The nodule of non-metabolically active adrenal soft tissue in the left side was quite diagnostic of adenoma. Grade II (Modified Bloom-Richardson 7/9) ER positive, PR positive, HER2 neu 2+ (FISH positive) and Ki-67 index 20% were confirmed by core needle biopsy (26 December 2025). On 14 January 2026, the patient was referred to the multidisciplinary consultation and pulmonology examination and the left breast conservation surgery with frozen section, axillary lymph node dissection (Level I and II), and Type I oncoplastic reconstruction procedure. End of operation histopathy revealed Grade II, 3.5 x 2.5 x 2 cm ( pT2) invasive ductal carcinoma (table 2).
Table 2: Final Histopathological Findings
|
Parameter |
Findings |
|
Final Diagnosis |
Carcinoma left breast |
|
Pathological Stage |
pT2 pN0 cMx |
|
Tumor Size |
3.5 × 2.5 × 2 cm |
|
Histology |
Invasive ductal carcinoma, Grade II (Modified Bloom–Richardson score 7/9) |
|
Estrogen Receptor (ER) |
Positive (60%) |
|
Progesterone Receptor (PR) |
Positive (70%) |
|
HER2/neu |
2+ (FISH positive, 20%) |
|
Ki-67 Proliferation Index |
20% |
|
Perineural Invasion |
Present |
|
Lymphovascular Invasion |
Not identified |
|
Axillary Lymph Nodes |
0/12 positive |
|
Surgical Margins |
Free of tumor |
Infection of the perineal area was identified and absence of lymphovascular emboli. The surgical margins were free of all tumors. Metastasis of the axillary lymph nodes (0/12; pN0). The patient was put on the TCH regimen (paclitaxel, carboplatin, trastuzumab) of six courses with trastuzumab maintenance therapy. On the 16 th February 2026, the patient was admitted and received Cycle 1 chemotherapy. She was studied and diagnosed to be conscious, orientated, afebrile, ECOG performance status 1 and hemodynamically stable. The baseline investigations were normal (Table 3)
Table 3: Adjuvant Chemotherapy – Cycle 1
|
Drug |
Dose |
Route |
|
Paclitaxel |
140 mg |
IV infusion |
|
Carboplatin |
200 mg |
IV infusion |
|
Trastuzumab |
550 mg |
IV infusion |
In accordance with an informed consent, the patient was provided with: With the assistance of supportive medications and pulmonology follow-up recommendations, the patient had been put on the infusion successfully and discharged in a hemodynamically stable state. Taking into account the already existing history of ILD and the subsequent severe ARDS in the patient, it was advised that all the respiratory system should be monitored using these stages that follow as the probability of pulmonary complications development is high.
DISCUSSION
The paclitaxel is a popular taxane chemotherapeutic agent which is employed in the proactive treatment of HER2-positive breast cancer. Though taxane usage has largely been safe, it has been attributed to pulmonary toxicities, including hypersensitivity pneumonitis, interstitial pneumonitis, organizing pneumonia, and, less frequently, to acute respiratory distress syndrome (ARDS). Patients with pre-existing interstitial lung disease (ILD) have the apparent risk of experiencing pulmonary toxicity. Radiographic evidence of fibrotic interstitial septal thickening and ground-glass opacities in both lungs was present in our patient before commencing chemotherapy. It is worth mentioning that she recently had recovered ARDS, which necessitated prone positioning and tracheostomy, indicating that she had grossly reduced pulmonary reserve. Despite having a stable underlying condition (ECOG 1) and normal heart operation (LVEF 64%), the initiation of adjuvant chemotherapy comprising of paclitaxel posed high chances of pulmonary toxicity. The pathophysiology of the paclitaxel pneumonitis has not been clear. Two mechanisms of paclitaxel pneumonitis are proposed including an allergic form (type I hypersensitivity reaction) and a cell-mediated cytotoxic form (type IV hypersensitivity reaction). Unmediated by type II hypersensitivity reactions, Type I hypersensitivity involves immunoglobulin E (IgE) and is linked to the discharge of histamine and other vasoactive substances with the help of basophils and mast cells. The response is linked with acute dyspnea, bronchospasm, hypotension and erythematous rash, which typically takes place soon after exposure to drugs. The incidence of this type is up to 30% in the case of paclitaxel-associated adverse reactions and it reduces to 1% to 3% when premedicated with steroids. Conversely, type IV hypersensitivity reactions, also referred to as delayed-type hypersensitivity reactions is mediated by T lymphocytes. Cytokines release leads to the activation of T cells and macrophages with the ultimate result of inflammatory tissue damages. This lagging response has a delay of between several hours to two weeks after exposure to the drug and is associated with progressive dyspnea and radiographical changes of bilateral ground-glass opacities or consolidation. Such signs were observed in our patient following the initiation of paclitaxel therapy, thereby indicating a pathogenesis which is caused by delayed hypersensitivity reactions [10,11]. The association between the infusion of paclitaxel and the onset of pulmonary failure in the background of previous imaging findings on the presence of inflammatory ILD is very suggestive in our case of pulmonary exacerbation as a result of chemotherapy. Drug induced pneumonitis and infection or further development of underlying ILD are often hard to tell. It involves the suspected drug and the administration of systemic corticosteroids in moderated to severe cases in management. The diagnosis is essential at the earliest stage, particularly in patients with low lung reserve since it may lead to irreversible lung damage or repeated ARDS when no treatment is done. It requires a high degree of coordination between oncology and pulmonology team in the decisions involving the continuation, changing or discontinuation of adjuvant therapy in high risk patients. The given case elucidates the necessity of paying extra attention to the risks and benefits before starting the taxane-based chemotherapy in a patient with the existing significant lung disease. Although chemotherapy with adjuvants is an established form of treatment in the presence of HER2-positive breast cancer, one of them should be significant due to the risk of pulmonary toxicity, especially in a patient who has a history of a serious respiratory illness.
CONCLUSION
Paclitaxel-related pneumonitis is an uncommon but severe complication particularly among patients who have some underlying interstitial lung disease and low pulmonary reserve. The pulmonary deterioration, which occurs after taxane treatment, may be confusing with infection or further development of the underlying pulmonary disease, which may result in delays in diagnosis. Accordingly, an early diagnosis of drug-induced pneumonitis should be made in the presence of the development of new or the exacerbation of dyspnea, hypoxia, and radiographic evolution of ground-glass opacities after chemotherapy. This case underscores the need to have an extensive pulmonary analysis and risk benefit analysis before administering adjuvant therapy based on taxanes in high-risk patients. It is highly important to stop the causative agent promptly, start corticosteroid therapy early, and monitor outcome closely to avoid the irreversible damage to the lungs, and to maximize the results.
REFERENCES


Dipanjan Maity, Ponni Sivaprakasam , Paclitaxel-Associated Pulmonary Exacerbation in a Patient with Pre-Existing Interstitial Lung Disease and Recent ARDS During Adjuvant Therapy for HER2-Positive Breast Cancer: A Case Report, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 258-263 https://doi.org/10.5281/zenodo.19384505
 10.5281/zenodo.19384505
10.5281/zenodo.19384505
