Shri Vishnu College of Pharmacy, Andhra Pradesh
Polymyxin B remains a last-line intravenous antibiotic for multidrug-resistant Gram-negative infections. Nephrotoxicity limits its use and complicates dosing decisions in patients with renal impairment. Debate persists about whether once-daily (OD) or twice-daily (BD) maintenance regimens optimize efficacy and minimize kidney injury in this population.Objective: To critically review pharmacokinetic (PK), pharmacodynamic (PD), preclinical, and clinical evidence comparing OD and BD polymyxin B regimens in patients with impaired renal function, and to present practical recommendations for clinicians and directions for research.Methods: We performed a targeted review of population PK studies, systematic reviews, animal experiments, clinical observational studies comparing dosing frequency, and international consensus guidelines relevant to polymyxin B dosing in renal impairment. Key sources included the International Consensus Guidelines for polymyxin use, population PK reports, and comparative clinical nephrotoxicity analyses. Results and conclusions: Population PK analyses indicate that polymyxin B clearance is influenced by host factors and, in several cohorts, by renal function — although non-renal elimination pathways are also important; this partly explains diverging dose-adjustment recommendations. Preclinical animal data are conflicting: some studies suggest less nephrotoxicity with OD dosing, while others find greater toxicity with high single peaks or with more frequent fractionation depending on total daily dose and experimental design. Clinical evidence is limited largely to observational studies; a notable multicentre retrospective analysis found higher acute kidney injury (AKI) rates with OD dosing versus BD, but randomized controlled trials (RCTs) are lacking. International consensus guidelines generally recommend a loading dose followed by BD maintenance (e.g., 1.25–1.5 mg/kg every 12 h) and emphasize therapeutic drug monitoring (TDM) where available. Given current evidence, BD maintenance with individualized adjustments (guided by TDM and close renal monitoring) is the most prudent approach in patients with renal impairment.
Polymyxin B is a cyclic lipopeptide antibiotic revived as a last-resort option for severe infections caused by carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), carbapenem-resistant Pseudomonas aeruginosa, and other carbapenem-resistant bacteria worldwide[1]. Its clinical utility is circumscribed by nephrotoxicity, which occurs commonly and ranges from mild creatinine rises to severe acute kidney injury (AKI) requiring renal replacement therapy[17]. A recent meta-analysis reported that 36–47% of patients treated with polymyxins develop AKI, with higher risk linked to total dose, treatment duration, and concurrent use of other nephrotoxic drugs[8][9]. Determining an optimal dosing regimen balancing antimicrobial efficacy (PK/PD targets) against nephrotoxic risk is particularly challenging in patients with pre-existing renal impairment or unstable renal function[1],[5]. Historically, polymyxin dosing approaches varied widely; contemporary practice has coalesced around loading doses and divided (q12h) maintenance regimens in many centres, but controversies remain about whether once-daily (OD) dosing may reduce toxicity without compromising efficacy[2,20]. This review synthesizes existing PK, PD, preclinical, clinical and guideline evidence.
METHODS
We performed a targeted literature search addressing polymyxin B pharmacokinetics, population PK models, nephrotoxicity, dosing frequency comparisons and guidelines for dosing in renal impairment. Search terms included “polymyxin B pharmacokinetics”, “polymyxin B renal impairment”, “once daily versus twice daily polymyxin B”, “polymyxin nephrotoxicity”, and “polymyxin guidelines” and clinical OD vs BD comparative studies.
PHARMACOKINETICS AND THE INFLUENCE OF RENAL FUNCTION
Overview of PMB PK/PD principles
Polymyxin B demonstrates concentration-dependent killing and an AUC/MIC relationship is frequently cited as the principal PK/PD index correlating with efficacy[1],[5]. A recent population PK modeling study, using aggregated polymyxin B free-plasma concentrations from published clinical datasets (J Clin Pharmacol 2023), supports this concept by showing that attainment of target exposures associated with optimal AUC/MIC ratios often requires higher total daily doses compared with those commonly used in practice. Monte Carlo simulations performed in critically ill patient scenarios demonstrated that standard dosing regimens often fail to achieve adequate Probability of Target Attainment when organism MICs are ≥1 mg/L, while simultaneously increasing the likelihood of nephrotoxic exposures. This emphasizes the narrow therapeutic window of polymyxin B and suggests the use of individualized dosing strategies-especially TDM-guided dose escalation-when treating high-MIC pathogens.[12] Achieving adequate systemic exposure against high-MIC pathogens often requires substantial daily doses, but this runs counter to toxicity concerns. Loading doses reduce time to therapeutic exposure, while maintenance dosing determines steady-state exposure and toxicity risk[3]. In one of the original mechanistic studies, Abdelraouf et al. (2012) showed, in a controlled rat model, that dividing the same total daily dose into BID or TID regimens resulted in significantly greater tubular injury-elevated KIM-1/NGAL and extensive histopathologic damage-compared to once-daily dosing due to prolonged tissue exposure and inadequate recovery time[20]. These findings were complemented by a human kidney-on-a-chip model developed by Weber et al. (2018); it was established that polymyxin B internalization follows the megalin-cubilin pathway, which accumulates in mitochondria and lysosomes, causing oxidative stress leading to apoptotic injury[18],[19]. Briefly, high concentration causes minimal toxicity, while prolonged moderate concentration produces substantial proximal tubular damage, confirming that cumulative intracellular exposure and elevated Cmin drive nephrotoxicity but not Cmax.[7],[17],[18],[19],[20]
Taken as a whole, these studies provide a coherent mechanistic insight to explain why once-daily dosing is less nephrotoxic than divided dosing despite identical AUC and why patients with reduced renal reserve (CKD/ESRD) are particularly vulnerable to sustained elevated troughs.[17,18,20]
Clearance and renal function
Historically, polymyxin B was considered primarily cleared by non-renal mechanisms unlike colistin prodrug CMS, suggesting limited need for renal dose adjustment. Although polymyxin B undergoes minimal renal excretion (<5% of dose), Manchandani et al. demonstrated that the kidneys—particularly the renal cortex and proximal tubules—accumulate the highest tissue concentrations of the drug. This indicates that nephrotoxicity is not related to clearance but to preferential intracellular uptake and retention within tubular cells.[19] Their biodistribution findings align with mechanistic data showing receptor-mediated endocytosis and intracellular accumulation as the drivers of injury, reinforcing that sustained systemic exposure (high Cmin), rather than urinary elimination, dictates renal toxicity risk.[18],[20] The growing body of evidence suggests that polymyxin B–induced nephrotoxicity is an exposure-driven process, and trough concentration (Cmin) is a more reliable predictor of kidney injury compared with peak levels.[17] Han et al. demonstrated that patients who developed AKI had more than double the median Cmin of non-AKI patients and identified a threshold of 3.13 mg/L above which the risk of AKI rose sharply.[17] Mechanistic studies utilizing a human kidney-on-a-chip model illustrated that polymyxin B is actively internalized by proximal tubular cells through the megalin–cubilin pathway and accumulates within mitochondria and lysosomes, where it evokes oxidative stress and cell injury.[18] Importantly, sustained moderate exposure caused far greater toxicity than brief high peaks, confirming a Cmin-driven pattern.[18],[20] Animal studies further showed that divided dosing regimens (BID/TID) produce higher troughs and greater nephrotoxicity than once-daily dosing despite similar total daily doses.[20],[21] Along with PK/TD modeling, these findings provide a basis for the preferential use of dosing strategies which minimize Cmin-particularly in patients with impaired renal reserve-to reduce nephrotoxic exposure while preserving antimicrobial efficacy However, multiple recent population PK analyses have identified covariates including creatinine clearance or other indices of renal function that modestly, but significantly, influence clearance in certain cohorts including critically ill and transplant recipients.[3],[4],[5] Polymyxin B clearance (CL ≈ 2.37 L/h) was well described by a one-compartment model, and total body weight was not a statistically significant predictor of clearance, suggesting weight-based dosing requires further evaluation, according to Kubin et al. (2018).Such findings explain divergent recommendations some groups advocate weight-based dosing with no routine renal adjustment, whereas others propose renal-function informed dose reduction in severe impairment or dynamic AKI. Recent population PK/TD modeling in critically ill adults further quantified the relationship between systemic exposure and nephrotoxicity risk, providing thresholds to guide individualized dosing and TDM strategies.[1],[11],[17]
Preclinical evidence: frequency, uptake and nephrotoxicity mechanisms
Animal data on dose fractionation and renal toxicity are heterogeneous. Certain rodent studies showed relatively less histologic or biomarker evidence of renal injury with single high daily doses compared with the same total daily dose divided into multiple administrations a finding attributed to saturable uptake mechanisms in proximal tubular cells that limit intracellular accumulation after a large single dose. In line with this, Sun et al. (2021) showed that while controls remained stable, rats given the divided 9 mg/kg q12h regimen showed slightly higher and more prolonged serum creatinine elevations over 96 hours compared with the 18 mg/kg q24h group, suggesting greater renal stress with fractionated dosing.[6] Conversely, other animal experiments demonstrated greater injury with large peaks or with specific fractionation schedules; results depended strongly on species, dosing route, total daily dose, and endpoints used. Translational extrapolation to human intravenous dosing is therefore uncertain. The conflicting preclinical signal underlines the importance of clinical human data and TDM.[20],[21]
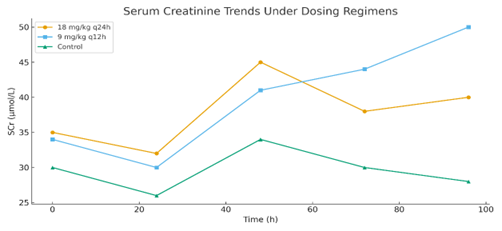
Figure 1. Serum creatinine trends under different dosing regimens of polymyxin B in rats. Values reproduced conceptually based on Sun W. et al., 2021.[6]
Clinical evidence comparing OD and BD regimens
Observational cohort data
The human clinical literature that directly compares OD versus BD polymyxin B maintenance regimens is limited and mostly observational. A commonly cited multicentre retrospective study reported significantly higher AKI incidence among patients receiving once-daily dosing compared with twice-daily dosing, with a similar time to AKI onset and mostly reversible renal dysfunction after therapy change or cessation.[15],[2] Other retrospective analyses and meta-analytic summaries corroborate increased nephrotoxicity risk associated with higher daily doses and concomitant nephrotoxins, but the direct effect of dosing frequency remains incompletely resolved by confounding factors inherent to observational studies such as patient severity, co-medications, cumulative exposure, and indication bias.[5],[17] More recently, Hanafin et al. (2025) modelled exposure-toxicity relationships in critically ill adults in a population PK/toxicodynamic analysis and predicted an increased probability of AKI with OD compared to BD at the same total daily dose. This effect was driven by modelled distributions showing slightly higher AUC?? and modest trough elevations in a subset of OD patients, thereby increasing predicted toxicity. However, these findings reflect simulated exposures rather than measured concentrations and contrast with mechanistic and organ-on-chip data that show that sustained intracellular accumulation and elevated Cmin-not peak concentrations-are the dominant drivers of polymyxin B nephrotoxicity. As such, this study reinforces the uncertainty in clinical frequency-related toxicity differences and highlights the pressing need for prospective trials employing real-time TDM and standardized AKI definitions.[11] Notably, in a small retrospective series of five renally impaired patients treated exclusively with BD dosing (Yu et al.), the only individual who developed neurotoxicity was receiving the twice-daily regimen. This result is consistent with the clinical PK observations of Yu et al. (2023), who found that excessive trough concentrations (Cmin >3 mg/L), a range linked to an increased risk of AKI, were often seen in renally impaired patients receiving routine twice-daily polymyxin B[13]. More robust clinical exposure–response evidence has recently emerged from a prospective study published in Critical Care evaluating AUC thresholds as predictors of both efficacy and nephrotoxicity in patients with carbapenem-resistant Gram-negative infections. This investigation represents one of the most clinically meaningful datasets to date, demonstrating that polymyxin B efficacy and renal toxicity are governed not simply by total daily dose or dosing frequency, but by the precise magnitude of systemic exposure. The authors specified a very clear inflection point in the exposure–toxicity curve; when AUC24 exceeded approximately 60–70 mg·h/L, probability of AKI increased steeply and consistently, while exposures within the 50–60 mg·h/L range maximized microbiological response with substantially lower renal risk. Of particular note, trough concentrations—again, not peak levels—were identified as the strongest determinant of toxicity, confirming mechanistic observations from organ-on-chip models and prior clinical PK analyses that sustained intracellular accumulation, not transient peaks, drives proximal tubular injury. Importantly, the authors reported that neither once-daily nor twice-daily dosing inherently guarantees safe exposure. Rather, failing to control AUC and Cmin is the primary determinant of nephrotoxicity. The present study provides critical evidence, now clinically validated, that polymyxin B therapy in renally impaired patients must be TDM-guided, AUC-targeted dosing, and that dosing frequency decisions should be secondary to attaining and maintaining exposures within this therapeutic window.[23]This observation highlights that patients with renal dysfunction may be particularly vulnerable to neurotoxic effects when exposed to repeated peak concentrations, further complicating interpretation of BD versus OD toxicity patterns.[22]
Table 1.Exposure–Toxicity Stratification of Polymyxin B: PK Parameters, Trough Concentrations, and Model-Predicted AKI Risk[11]
|
Exposure / PK Parameter |
Low Exposure Group |
Medium Exposure Group |
High Exposure Group |
Key Interpretation |
|
Approx. AUC24 range (mg·h/L) |
~25–40 mg·h/L |
~40–55 mg·h/L |
>55 mg·h/L |
Higher AUC associated with graded increase in AKI probability. |
|
Median predicted probability of AKI |
≈22–28% |
≈35–45% |
≈55–65% |
AKI risk increases stepwise across exposure categories. |
|
Model-predicted AKI risk: OD vs BD |
~5–10% higher (OD) |
~5–12% higher (OD) |
~8–15% higher (OD) |
Higher troughs (Cmin) with OD drive predicted toxicity differences. |
|
Trough concentration (Cmin) |
Lowest |
Moderate |
Highest |
Cmin identified as strongest TD predictor of nephrotoxicity. |
|
Mechanistic implication |
Minimal intracellular accumulation |
Moderate accumulation |
High accumulation |
Supports cumulative exposure → tubular injury model. |
|
Proportion of simulated patients |
~30–35% |
~40–45% |
~20–25% |
Reflects spread of exposure in critically ill population. |
|
Clinical interpretation |
Lower toxicity but underexposure risk |
Balanced efficacy/toxicity |
High toxicity risk; prioritize TDM |
High exposure group drives most modeled AKI events. |
Population studies and TDM experiences
Population PK and TDM-guided dosing studies have shown that standard dosing often achieves similar plasma exposures across a range of renal functions, though subsets severe AKI, CRRT may differ.[3],[4],[5] Where TDM was applied, individualized dose adjustments frequently improved target attainment without obvious increases in toxicity.[17] These data support model-informed individualized dosing over one-size-fits-all rules, and suggest that dose frequency per se may be less important than total exposure AUC and how that exposure is achieved and monitored.[5]
Gaps: absence of randomized trials
To date there are no large randomized controlled trials directly comparing OD versus BD polymyxin B in adults with renal impairment.[1] Existing observational data suggest possible harm with OD dosing, but residual confounding is likely.[2],[5] Consequently, definitive recommendations require prospective randomized or TDM-guided adaptive trials — especially in renal impairment and CRRT strata.[1]
Guidelines and expert opinions
The 2019 International Consensus Guidelines synthesize available data and recommend using a loading dose followed by divided maintenance dosing (commonly q12h) and emphasize that polymyxin B is generally preferred for systemic infections over colistin, and that TDM and model-informed precision dosing are desirable where available. The guidelines advise cautious individualized management in patients with renal dysfunction and acknowledge uncertainties in the influence of renal function on PMB clearance. Many centres and subsequent reviews have adopted BD maintenance dosing as the standard approach while calling for further research into renal adjustments and frequency comparisons.[1],[5]
Practical recommendations (evidence-based, pragmatic)
Research priorities
Limitations of this review
This is a targeted, not systematic, review intended to synthesize clinically relevant evidence for decision makers it did not follow a full systematic review.[5] The available clinical comparisons are observational and susceptible to confounding the translational value of animal data is limited by interspecies differences.[20],[16],[]21] Despite these limitations, convergent evidence from PPK studies, consensus guidelines, and clinical cohorts supports BD maintenance dosing with individualized adjustments in renal impairment.[1],[3],[4],[5],[17]
CONCLUSION
Given the current state of the evidence base-population PK studies that demonstrate variable but sometimes significant renal influence on polymyxin B clearance, conflicting preclinical findings on dose-fractionation, and limited observational human data-the optimal dosing frequency in renally impaired patients is uncertain.[3],[4],[5] Whereas some animal models suggest that once-daily exposure may engender lower nephrotoxicity due to reduced cumulative trough levels, such a safety advantage has not been consistently demonstrated in human observational studies, and higher Cmin values with divided dosing remain a concern in patients with impaired renal function.[17],[2],[5]
Currently, there is a lack of high-quality evidence to recommend once-daily maintenance dosing over twice-daily regimens in renal impairment. The most prudent strategy remains one including a loading dose followed by individualized dosing-commonly twice daily-guided by therapeutic drug monitoring and close renal surveillance. There is an urgent need for robust randomized or model-informed prospective studies to clarify whether OD or BD dosing offers superior efficacy and safety across different degrees of renal dysfunction and CRRT settings.[1]
REFERENCES

Dr. Vadapalli Rama Rao, Adithya Shetty H, Mohammed Sonia, Dr. Manoj D.V, Prateeksha Vinnu, Adnan Sharief SK, Nalajala Akash, Polymyxin B Dosing in Renal Impairment Once-Daily Versus Twice-Daily Regimens: A Critical Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 2591-2599. https://doi.org/10.5281/zenodo.17951570
 10.5281/zenodo.17951570
10.5281/zenodo.17951570
