Gallstones are the same as gallbladder stones. They are crystals that are made up of cholesterol, bile salts, and bilirubin and form inside the gallbladder. Metabolic, environmental, genetic, and lifestyle factors, among other things, are responsible for bile super saturation and crystal nucleation leading to the formation of these stones. Gallstones, which may be different in size and content and thus be cholesterol, pigment, or mixed stones, are capable of manifesting a broad range of clinical symptoms, such as those being asymptomatic gallbladder sludge, severe biliary colic, cholecystitis, or pancreatitis in some cases. Therefore, a diagnostic approach by Ultrasonography is the most frequent and a therapeutic approach by laparoscopic cholecystectomy is the treatment of choice in symptomatic patients. Among new diagnostic and therapeutic strategies, the endoscopic gallbladder-preserving procedure is the one that most equally envisages the future of a better management of gallbladder stones without sacrificing function. Understanding the etiology, clinical presentation, risk factors, and current therapeutic approaches is the key to achieving better patient outcomes and to guiding future investigations.
Keywords
Cholelithiasis, biliary colic, gallbladder stone, pigment stone, cholesterol stone
Introduction
×
Gallbladder stones, or gallstones, refer to the solid formations that grow in the biliary system, most commonly in the gallbladder. They can affect 20% of the adult population in developed countries and are the main trigger of gastrointestinal problems all over the world. When cholesterol, bilirubin, or calcium salts that are part of the bile cause one substance to be overly saturated, gallstones are formed. This is the reason that the stones are crystals in nature. The risk factors for gallstones are “four Fs”: female sex, age over forty, overweight, and pregnancy or hormone therapy that affects fertility. The rapid weight-losing program, as well as blood diseases and a few ethnic groups, are also on the risk list. Most of the time, gallstone sufferers are symptom-free. However, gallstones can also cause biliary colic, acute cholecystitis, cholangitis, and gallstone pancreatitis. Ultrasonography is highly sensitive and specific, so it is the best method for diagnosis. The main treatment for symptomatic cases is laparoscopic cholecystectomy. The discovery of the mechanism of the formation of gallstones has rekindled the interest in non-invasive methods and those allowing the preservation of the gallbladder. Such a tendency corresponds to the different manners of dealing with the disease. Gallbladder stones, also called gallstones or cholelithiasis, are the crystalline growths in the gallbladder. The latter, a small, somewhat pear-shaped organ, lies under the liver and is the place for bile storage. The production of these stones due to the disruption of the substances in bile, cholesterol or bilirubin for example. Hence the happening of precipitation and crystallization. The size of gallstones can range from very small to large, and the stones may be single or multiple. Most people with gallstones are asymptomatic and have no idea of the stones. Still, some patients may suffer from biliary colic, acute cholecystitis, and in extreme cases, blockages that can lead to jaundice or pancreatitis significant symptoms and complications. Worldwide, cholelithiasis is a disease with a high frequency of occurrence, and it is at the top of the list of digestive diseases that require surgery. The risk factors for it are female sex, aging, obesity, rapid weight loss, family history, and certain medical conditions or medications that may cause it. Understanding of gallbladder stones' characteristics, origin, and clinical impact is the basis of efficient prevention, prompt diagnosis, and correct management. This facilitates the decline of health problems and complications related to this condition.
Fig No:- 1 Gall Bladder Stones
Etiology
Causes of Gallbladder Stones: Gallbladder stones, also known as cholelithiasis, are caused by a confluence of metabolic, genetic, and environmental factors that interfere with the normal operation of the gallbladder and bile. The primary processes and risk factors underlying gallstone formation are described in the sections that follow:
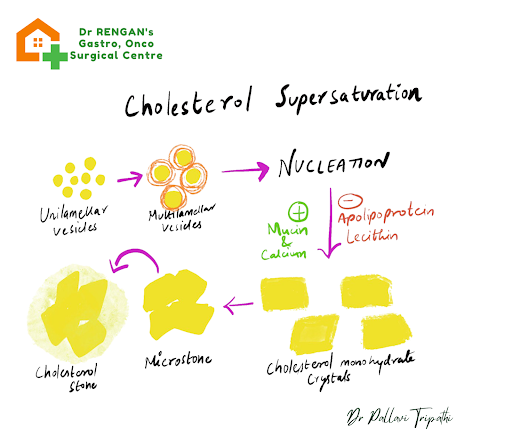
Supersaturation of cholesterol: Phospholipids, bile salts, and cholesterol should all be present in human bile in a balanced ratio. It happens when the liver produces so much cholesterol that it can no longer be dissolved by phospholipids and bile salts. Consequently, nuclei of cholesterol monohydrate are formed, which starts the formation of stones. Supersaturation of this kind is brought about by:
High cholesterol secretion as a result of either high fat consumption or the body producing too much cholesterol.
Low secretion of bile acid, commonly caused by the reduced activity of the enzyme cholesterol 7α-hydroxylase, which leads to a smaller bile acid pool.
A shortage of phospholipids that reduces the ability of lecithin to maintain cholesterol in the bile at the proper level.Such alterations in bile composition can account for up to 80% of gallstones in Western populations.
fig no:- 2 Cholesterol Supersaturation
Gallbladder Hypomotility: Inflammation of the gallbladder hampers its emptying and the bile is usually left behind. The condition that the bile is accumulated, which leads to crystal formation and aggregation. Some of the factors are:
Fasting or rapid weight loss that diminishes the release of cholecystokinin and decelerates gallbladder contraction.
Estrogen therapy and pregnancy in which the elevated levels of estrogen reduce the secretion of bile acids and slow the flow of bile.
Neuromuscular defects in the gallbladder muscle which in most cases are due to chronic inflammations or diabetic nerve damage.Because supersaturated bile can stay for a longer time, gallstones can grow.
fig no:-3 Gallbladder Hypomotility
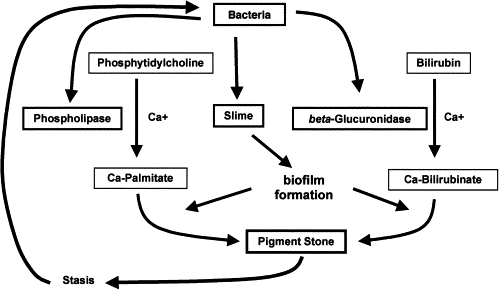
Pigment Stone Formation: Pigment stones develop when there is an excess of bilirubin compounds in the bile, mostly calcium bilirubinate. The main causes are:
Hematologic diseases such as sickle cell anemia and hereditary spherocytosis which lead to the increase of unconjugated bilirubin.
Bile duct infections that can cause bacteria to become more active creating an environment that changes bilirubin and allows the formation of pigments.
Cirrhosis and chronic liver diseases where the organ that is supposed to remove bilirubin from the body fails leading to the accumulation of it in the bile.The proportion of pigment stones to other types of gallstones in some Asian and hemolytic populations is higher.
Fig No:-4 Pigmented Stone Cycle
Genetic and Ethnic Predisposition: According to family and twin studies genetic factors can be linked to the probability of gallstone diseases. Some of the related genes include:
ABCG5/G8 transporters genes which code for the proteins that regulate cholesterol secretion into the bile.
CYP7A1 enzyme that is essential in bile acid formation.
The SLCO1B1 transporter that has an effect on the absorption of bile salts.Ethnically, Native Americans and Hispanics are genetically more susceptible to having gallstones as their prevalence is quite high.
Additional Risk Factors:
Female sex: The hormone estrogen raises the cholesterol levels of the bile thereby doubling the risk of gallstones in women.
The age of over 40 years: The longer a person is exposed to different risk factors the greater the chances of the gallstone formation.
Metabolic syndrome and obesity: The production of cholesterol in the liver is facilitated by insulin resistance which is a feature of obesity and metabolic syndrome.
Rapid weight loss: Quick removal of the cholesterol from the peripheral tissue and its transfer into the bile can be one of the factors that lead to the formation of stones.
Pathophysiology
Pathophysiology of Gallbladder Stones:- Gallbladder stones or cholelithiasis are a result of changes in bile composition and gallbladder function due to several factors. These are the main processes that trigger gallbladder stone formation and growth.
Bile Supersaturation: Bile is a tempered combination of cholesterol, bile salts, and phospholipids. The trio keeps cholesterol dissolvable. A condition of supersaturation arises when the liver secretes cholesterol which is more than the double of bile salts and phospholipids so that the solubility limit is exceeded. On this occasion, cholesterol monohydrate crystals are generated. The elements that add to this are high cholesterol levels in blood, lowered production of bile acids, and deficiency of phospholipids in hepatic cells.
Nucleation and Mucin Hypersecretion: After the formation of cholesterol crystals, a progression to stone formation requires the congregation of these. Mucin glycoproteins, released by gallbladder epithelial cells, give a base for the crystals to start nucleation. An imbalance that favors pronucleating mucins over antinucleating proteins speeds up crystal aggregation. Excess mucin and impaired gallbladder emptying facilitate the transformation of small crystals into bigger ones.
Gallbladder Hypomotility: The process of gallbladder evacuation in a crystal formation stage is very important as it helps to get rid of the crystals that have started developing. A hypomotility, which may be caused by fasting, rapid loss of weight, pregnancy, hormonal therapy or neuromuscular disorders, results in bile stasis. Here, crystals are retained in the gallbladder for a longer time and thus, the tendency to cluster is increased. Decreased release of cholecystokinin and smooth muscle malfunction further exacerbate the stasis.
Types of Stones and Specific Pathways: Cholesterol stones account for more than 80% of gallstones in the west. Their formation involves bile supersaturation and nucleation directly. Black pigment stones have a major part of calcium bilirubinate in them and develop in sterile bile as a result of unconjugated bilirubin elevation, e.g. in hemolysis, cirrhosis, etc. Besides, the gallbladder lining’s antioxidative destruction and overproduction of mucin also encourage the formation of these black stones. Brown pigment stones arise in the bile ducts if there is an infection. Enzymatic action of bacterial β-glucuronidase on bilirubin followed by calcium bilirubinate polymerization and stone formation in the ducts is the sequence leading to the origin of bacteria in the bile ducts.
Inflammatory and Oxidative Contributions: The gallbladder lining that has been chronically infl amed, either because of continuous crystal irritation or low-grade infection, creates oxidative stress. This upsets epithelial cells and raises mucin secretion, thus establishing conditions that can rapidly advance stone growth as well as alter the gallbladder wall.
Genetic and Metabolic Influences: Moderations of genes concerning bile transport and bile acid synthesis affect cholesterol release and bile acid levels, thus having a sway on stones' risk. Metabolic syndrome and insulin resistance not only increase the production of cholesterol by the liver but also make the gallbladder weak, hence, people become more liable to cholesterol stones.
Clinical Implications of Pathophysiology: When stones increase in size, they are able to obstruct the cystic or common bile duct. It can then cause biliary colic, acute cholecystitis, cholangitis, or gallstone pancreatitis. Knowing these mechanisms helps to consider preventive measures and novel therapies such as bile acid dissolving drugs and ways to facilitate gallbladder motility.
Signs and Symptoms
Gallbladder stones, or cholelithiasis, frequently remain silent with no signs or symptoms. On occasion, they are discovered unintentionally while checking for some other disorders with imaging. When the signs present, these are generally due to the obstruction of bile fl ow by the stones. Such a situation causes inflammations, infections, or the occurrence of biliary colic.
Biliary Colic (Gallstone Attack): Biliary colic is the major symptom of biliary colic. A sudden, intense and continuous pain in the right upper quadrant or epigastric area is its characteristic. The pain can become crampy, sharp or stabbing. Some people who suffer from it compare it to a tightening. In some cases, the pain radiates to the right shoulder, the area between the shoulder blades, or, d ere is a very low possibility also of the chest or left upper quadrant. The duration of attacks is from a few minutes to a few hours; their frequency is usually after fatty meals. What takes place is that bile pressure is increased due to gallbladder contraction. At times, the pain may interfere with sleep. Apart from the pain, nausea and vomiting are usually present.
Chronic Symptoms: There is also a group of patients who suffer from indigestion, bloating, and vomiting all the time. These complaints tend to be aggravated after the consumption of fatty and greasy foods but are usually less severe than acute colic. This can be an indication of partial obstruction or gallbladder malfunction.
Acute Cholecystitis: If a gallstone ends up persistently obstructing the cystic duct, then inflammation along with infection of the gallbladder wall will be the result. Constant pain in the right upper quadrant with tenderness, fever, nausea, vomiting, and a palpable gallbladder mass are the recognizable symptoms. Murphy’s sign, which expresses the stopping of inspiration during gallbladder palpation, is usually a confirmed positive. Immediate medical attention is required for acute cholecystitis.
Complications with Jaundice and Infection: If stones dislodge into the common bile duct, they may cause blockage which leads to jaundice, a condition where the skin and eyes become yellow because of the accumulation of bile. Trouble breathing, rapid heartbeat, tiredness, weight loss, fever, and stomach pain are among the symptoms. The Charcot triad is a combination of signs with fever, jaundice, and right upper quadrant pain, which is the usual presentation of ascending cholangitis - a bacterial infection of the bile ducts. The illness may progress to the Reynold pentad, another stage where low blood pressure and altered mental status join the Charcot triad symptoms. This illness requires treatment immediately upon arrival.
Other Symptoms:
Nausea and vomiting, especially after eating fatty foods
Bloating and excessive gas
Fever and chills, which can indicate infection
Ongoing abdominal tenderness
Fast heartbeat during infection or inflammation
Asymptomatic gallstones: Asymptomatic gallstones are those that make no symptoms and are discovered by chance and they amount to 80%. On the other hand, they can become problematic, and are therefore not to be neglected.
Diagnosis
Diagnosis and Pharmacotherapy of Gallbladder Stones:The cornerstone of the treatment of gallbladder stones is proper diagnosis and suitable medical therapy for a few selected patients. Here is a brief overview of diagnostic and therapeutic approaches in gallstone disease.
Diagnostic Evaluation:
Clinical Assessment and Laboratory Tests: The first evaluation is a long history and physical examination to identify biliary colic, tenderness in the right upper quadrant, and Murphy’s sign. Laboratory tests are used to detect complications and not to confirm the presence of stones. Inflammatory response with an increase in white blood cells "Leukocytosis" occurs in cholecystitis. "High" bilirubin, alkaline phosphatase, and transaminase levels point to choledocholithiasis or cholangitis. Elevated amylase and lipase are markers of gallstone, induced pancreatitis.
Abdominal Ultrasound: The first step is an ultrasound scan, a test which has a sensitivity of more than 95% and a specificity of more than 98% for the identification of gallstones. The test visualizes bright spots with no sound behind them, gallbladder wall thickening, and fluid around the gallbladder.
Endoscopic Ultrasound (EUS): By far, EUS has higher sensitivity in locating microlithiasis and identifying stones in the common bile duct. The procedure is performed when a transabdominal ultrasound is inconclusive.
Magnetic Resonance Cholangiopancreatography (MRCP): MRCP techniques enable the biliary and pancreatic duct system to be seen without the use of a scope. This is an excellent method for diagnosing choledocholithiasis and does not involve radiation exposure.
Endoscopic Retrograde Cholangiopancreatography (ERCP): Primarily, ERCP is a therapeutic method for the extraction of stones. Its diagnostic usefulness is minimal because of its invasiveness and the danger of pancreatitis and perforation.
Hepatobiliary Iminodiacetic Acid (HIDA) Scan: The nuclear test evaluates the openness of the cystic duct as well as the gallbladder's ejection fraction. It is very accurate in detecting acute cholecystitis when the ultrasound findings are doubtful.
Computed Tomography (CT): CT is a less sensitive method for detecting stones but it can be used for checking the development of the disease, other conditions, and radiopaque stones.
Pharmacologic Management: One of the medical treatments is dissolution of the gallstones with bile acids. This treatment is appropriate for those patients who have small (<15 mm), radiolucent cholesterol stones; functional gallbladders (ejection fraction ≥50%); and those who are inoperable. The main compounds that are used are:
Ursodeoxycholic Acid (UDCA)
Operation: By lessening the liver's cholesterol secretion and adding to the bile acid pool, the drug reduces cholesterol saturation in bile.Amount: 8, 12 mg/kg/day in several doses.
Result: Full dissolution rates vary from 20% to 70% within 6 to 24 months, with the rate of success being more when the stones are less than 5 mm.
Time: The response is evaluated at 6 months; the treatment is discontinued if there is no significant reduction. In the event of partial dissolution, the treatment may be extended for 24 months at the most.
Side Effects: The drug is usually quite well tolerated; however, diarrhea is the most frequent side effect.
Chenodeoxycholic Acid (CDCA) and Combination Therapy:
CDCA has the same properties in dissolving stones but a higher number of side effects. A mixture of UDCA and CDCA (5, 6 mg/kg/day each) may accelerate the dissolution process, however, it may also aggravate the gastrointestinal tract with symptoms such as diarrhea. The duration of the intended treatment is about the same as for UDCA alone with the added requirement of monitoring symptom improvement.
Clinical Outcomes and Considerations:Stone Size: Stones that are smaller than 5 mm have a greater chance of being dissolved successfully.
Symptom Relief: Patients receiving UDCA treatment experience less biliary colic and dyspeptic symptoms even if they are not necessarily complete stone dissolution ones.
Recurrence: Gallstones are likely to reappear after cessation of bile acid therapy; therefore, regular follow, up is necessary.
Emerging Therapies: Research is underway on other agents and combinations (e.g., UDCA plus PUFA) for better effectiveness.
Treatment of Gallbladder
Treatment of Gallbladder Stones and Their Types: A well, planned treatment of gallstone diseases is the key to success in recovering the patient. Factors such as the composition of the stones, the patient's symptoms, and some other personal factors need to be carefully considered while deciding the treatment. Nevertheless, gallstones can be differentiated into three main groups: cholesterol stones, black pigment stones, and brown pigment stones. Each variety has its own specifics regarding causes and treatment.
Types of Gallstones:-
Cholesterol Stones: One of the main constituents of these mollusks is crystalline cholesterol monohydrate, which makes up more than half of their total composition. They are the most common varieties in Western populations and are usually associated with production of an over, saturated bile and decreased activity of the gall, bladder
Black Pigment Stones : These stones are mainly comprised of calcium bilirubinate polymers and calcium carbonate. The stones develop in the sterile bile and their occurrence is associated with an increase in unconjugated bilirubin which may result from hemolytic disorders, cirrhosis or ileal surgery.
Brown Pigment Stones:The composition of these stones includes calcium bilirubinate and components derived from the bacterial cell walls. They originate in the infected bile ducts as bacteria deconjugate the bilirubin. Biliary tract infections and stasis are the most frequent causes of this process.
Treatment Modalities:
Watchful Waiting: Asymptomatic gallstones, often called "silent stones," do not need treatment because the annual risk of complications is low, less than 2%. Monitoring and lifestyle changes, like maintaining weight and following a low-fat diet, are recommended.
Medical Dissolution Therapy: This option is for patients with small, radiolucent cholesterol stones that are less than 15 mm in size, have a clear cystic duct, and are at high surgical risk. Ursodeoxycholic Acid (UDCA) lowers cholesterol saturation by reducing cholesterol secretion from the liver and improving bile flow. The standard dosage is 8 to 12 mg/kg per day, taken twice daily. Complete dissolution rates range from 30% to 60% over 6 to 24 months, with better success for stones smaller than 5 mm. Side effects are minimal, mostly including diarrhea. Chenodeoxycholic Acid (CDCA) can achieve similar results but is associated with a higher risk of liver damage and diarrhea, which limits its use. Combining UDCA and CDCA might improve results but can also increase gastrointestinal side effects.
Extracorporeal Shock Wave Lithotripsy (ESWL): This is a noninvasive method that uses focused shock waves to break apart cholesterol stones, followed by treatment with UDCA to dissolve any remaining fragments. It works well for a few small stones, under 3 cm, in patients who cannot undergo surgery. Success rates for ESWL are around 70%, though rates can vary based on stone composition and accessibility.
Endoscopic Interventions: Endoscopic Retrograde Cholangiopancreatography (ERCP) with sphincterotomy allows for the removal of stones from the common bile duct. This procedure is used for conditions like choledocholithiasis and cholangitis. Endoscopic Gallbladder Drainage and Stenting may be considered for managing acute cholecystitis in patients at high surgical risk, providing temporary relief.
Surgical Management: Laparoscopic Cholecystectomy is the standard treatment for symptomatic gallstones. It results in low complications and quick recovery. This procedure involves the removal of the gallbladder through small cuts in the abdomen and is indicated for biliary colic, cholecystitis, pancreatitis, and preventive removal in high-risk groups such as those with sickle cell disease. Open Cholecystectomy is reserved for more complicated cases with severe inflammation, adhesions, or specific patient issues that prevent laparoscopic surgery.
Percutaneous Cholecystostomy: This method uses imaging to guide the drainage of the gallbladder in critically ill or unstable patients with acute cholecystitis. It helps manage sepsis and inflammation before a more definitive surgery.
Treatment Selection Considerations:
The composition and size of the stones determine whether medical dissolution or lithotripsy is appropriate. The severity of symptoms and potential complications, such as cholecystitis or pancreatitis, require immediate surgical or endoscopic intervention. Patient comorbidities and surgical risks influence the choice among conservative, endoscopic, or percutaneous methods. Gallbladder function can be evaluated with a HIDA scan; a low ejection fraction, below 35%, favors cholecystectomy over dissolution therapy.
Prevention
Prevention of Gallbladder Stones: Gallstones start to form through various factors that include genetics, metabolism, diet, and lifestyle. Preventive measures mainly concentrate on eliminating these risk factors that are connected with bile supersaturation, poor gallbladder motility, and other symptoms. Efficient prevention comprises of lifestyle changes, dietary modification, and properly managing the present metabolic disorders.
Lifestyle and Dietary Modifications:
Maintain a Healthy Weight:- Among other things, obesity raises the risk of gallstones, as it doubles the level of cholesterol in bile. Fast weight loss and bariatric surgery are also known to have a side effect of gallstone formation. So, it is crucial to keep a healthy and stable weight by weighing down slowly, if necessary, and not losing the weight very quickly. Slow weight loss of around 0.5 kg per week is most effective in decreasing cholesterol oversaturation in bile and gallbladder hypokinesia.
Balanced Diet:- Diet high in fiber, fruits, vegetables, and healthy fats, such as omega, 3 fatty acids, may prevent the formation of gallstones. You should avoid saturated fats, refined carbohydrates, and food that have a high amount of cholesterol, because these contribute to gallstone formation. Proper hydration is also beneficial for good bile flow and getting rid of the stasis.
Reduce Risk of Diabetes and Metabolic Syndrome:- By maintaining normal blood sugar levels, blood pressure, and lipid profiles for those who suffer from metabolic syndrome, bile cholesterol saturation, and liver secretion can be lowered. This method can help to lessen the risk of gallstone formation.
Pharmacological Prevention:-
Use of Ursodeoxycholic Acid (UDCA): To be more specific, for the groups that are considered as risky, like patients with hemolytic diseases or those who lose weight rapidly, low, dose UDCA would be the therapy that prevents gallstones by reducing cholesterol levels in bile. However, it is not encouraged for general use because of its cost and limited supporting evidence.
Statins and Lipid, Lowering Agents:- Some studies suppose that statins may have a ghallstone lowering effect by reducing cholesterol synthesis and secretion, though this has not been widely accepted. They are primarily used to address hypercholesterolemia and not to prevent gallstones.
Regular Monitoring and Management of Underlying Conditions: -
The Bilirubin and cholesterol concentrations in the bile that contribute to pigment can be lessened by treating hemolytic anemia as well as liver diseases like cirrhosis.
Surgery for High, Risk Patients:- Prophylactic cholecystectomy is not usually performed on people who do not have symptoms. Nevertheless, it may be possible to take into consideration patients suffering from inherited disorders that cause the production of gallstones and its complications.
Additional Preventive Measures:-
Promote Physical Activity routine physical activity is very necessary for keeping an ideal weight and improving the metabolism of the fats which is the production related to the occurrence of gallstones. Avoid Prolonged Fasting:-Long fasting or total parenteral nutrition (TPN) can decrease gallbladder motility leading to stasis and an increased risk of stone formation. Eating small and frequent meals is very important in stimulating gallbladder contractions and hence improving bile flow.
CONCLUSION:
Preventing gallstone disease mainly focuses on lifestyle changes such as a protection of a healthy weight, proper nutrition, manageable metabolic control, and treatment of underlying conditions. The effectiveness of these approaches is more evident in high, risk individuals, who are advised to follow a gradual weight management program and dietary consultation. Pharmaco, logical prevention in combination with UDCA could be utilized for specific groups at high risk but generally is not allowed for all. Early detection and risk factor management are the cornerstones in reducing the formation of gallstones and their complications.
REFERENCES
Jones MW. Gallstones (Cholelithiasis). StatPearls [Internet]. 2024 Jun 1. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459370/
Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;368(9531):230–239.
Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;368(9531):230–239.Definition & Facts for Gallstones. NIDDK. 2025 Aug 26. Available from: https://www.niddk.nih.gov/health-information/digestive-diseases/gallstones/definition-facts
Gallstones – Diagnosis & treatment. Mayo Clinic. 2025 Apr 15.Sebghatollahi V. A Clinician’s Guide to Gallstones and Common Bile Duct (CBD). PMC. 2025 Jun 15.Buyuker F et al.
The effect of ursodeoxycholic acid in dissolving gallstones after laparoscopic sleeve gastrectomy. BMC Surg. 2025;25:101.Fromm H. Gallstone dissolution therapy. Gastroenterology. 1986;91(6):1560–1567.Lee SY et al. Gallstone dissolution effects of combination therapy with UDCA and PUFA. Gut Liver. 2024.
Definition & Facts for Gallstones. NIDDK. 2025 Aug 26.Buyuker F et al. The effect of ursodeoxycholic acid in dissolving gallstones after laparoscopic sleeve gastrectomy. BMC Surg. 2025;25:101.Fromm H. Gallstone dissolution therapy.
Gastroenterology. 1986;91(6):1560–1567.Gutbub et al. Extracorporeal shock wave lithotripsy in gallstone disease. J Hepatobiliary Pancreat Sci. 2023;30(4):289–297.Baron TH et al. Endoscopic and percutaneous management of gallbladder disease. Gastrointest Endosc Clin N Am. 2024;34(2):273–288.
Reference
Jones MW. Gallstones (Cholelithiasis). StatPearls [Internet]. 2024 Jun 1. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459370/
Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;368(9531):230–239.
Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;368(9531):230–239.Definition & Facts for Gallstones. NIDDK. 2025 Aug 26. Available from: https://www.niddk.nih.gov/health-information/digestive-diseases/gallstones/definition-facts
Gallstones – Diagnosis & treatment. Mayo Clinic. 2025 Apr 15.Sebghatollahi V. A Clinician’s Guide to Gallstones and Common Bile Duct (CBD). PMC. 2025 Jun 15.Buyuker F et al.
The effect of ursodeoxycholic acid in dissolving gallstones after laparoscopic sleeve gastrectomy. BMC Surg. 2025;25:101.Fromm H. Gallstone dissolution therapy. Gastroenterology. 1986;91(6):1560–1567.Lee SY et al. Gallstone dissolution effects of combination therapy with UDCA and PUFA. Gut Liver. 2024.
Definition & Facts for Gallstones. NIDDK. 2025 Aug 26.Buyuker F et al. The effect of ursodeoxycholic acid in dissolving gallstones after laparoscopic sleeve gastrectomy. BMC Surg. 2025;25:101.Fromm H. Gallstone dissolution therapy.
Gastroenterology. 1986;91(6):1560–1567.Gutbub et al. Extracorporeal shock wave lithotripsy in gallstone disease. J Hepatobiliary Pancreat Sci. 2023;30(4):289–297.Baron TH et al. Endoscopic and percutaneous management of gallbladder disease. Gastrointest Endosc Clin N Am. 2024;34(2):273–288.
Atharva Raut
Corresponding author
Department of Pharmacology, Dr. Rajendra Gode College of Pharmacy, Amravati -444602, Maharashtra (India).
Department of Pharmacology, Dr. Rajendra Gode College of Pharmacy, Amravati -444602, Maharashtra (India).
Rutuja Alone
Co-author
Department of Pharmacology, Dr. Rajendra Gode College of Pharmacy, Amravati -444602, Maharashtra (India).
Ashwani Aswar
Co-author
Department of Pharmacology, Dr. Rajendra Gode College of Pharmacy, Amravati -444602, Maharashtra (India).
Dr. Harigopal S. Sawarkar
Co-author
Department of Pharmacology, Dr. Rajendra Gode College of Pharmacy, Amravati -444602, Maharashtra (India).
Atharva Raut*, Rutuja Barange, Rutuja Alone, Ashwani Aswar, Dr. Harigopal S. Sawarkar, Pathophysiology and Management of Gallbladder Stones: Current Clinical Insights, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2364-2375 https://doi.org/10.5281/zenodo.17431120




 10.5281/zenodo.17431120
10.5281/zenodo.17431120