
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, St. Mary’s College of Pharmacy, Secunderabad, Telangana, 500025
Pharmaco-cybernetics is an emerging interdisciplinary field that integrates pharmacy, cybernetics, information technology, and healthcare systems to enhance medication safety, therapeutic effectiveness, and clinical decision-making. With the rapid digital transformation of healthcare in India, pharmaco-cybernetic systems offer significant potential in improving prescription management, drug monitoring, pharmacovigilance, and patient-centered care. This manuscript discusses the concept, scope, and applications of pharmaco-cybernetics, highlighting its role in clinical decision support, electronic health records, and real-time medication tracking. Particular emphasis is placed on the integration of pharmaco-cybernetic systems with the Ayushman Bharat Digital Mission (ABDM), using the Ayushman Bharat Health Account (ABHA) as a unique digital patient identifier to securely link prescriptions, dispensing data, and clinical outcomes. Such integration enables interoperable data exchange among healthcare providers, pharmacies, laboratories, and regulatory bodies, thereby reducing medication errors, preventing duplicate therapies, and supporting evidence-based healthcare delivery. Furthermore, the adoption of pharmaco-cybernetics strengthens pharmacovigilance through systematic collection and analysis of adverse drug reaction data, contributing to improved drug safety and regulatory oversight. Overall, pharmaco-cybernetics represents a transformative approach to modernizing pharmacy practice and advancing India’s digital health ecosystem
Pharmaco?cybernetics brings together the cybernetic ideas of feedback, control, and communication with modern pharmacy informatics to build learning systems around medication use. In these systems, digital tools such as electronic health records (EHRs), computerized provider order entry (CPOE), pharmacy information systems (PIS), clinical decision support systems (CDSS), telepharmacy platforms, and mobile health applications work in combination to support accurate documentation, automated safety checks, and continuous clinical monitoring, reducing human error and supporting truly patient?centered care 1.
As patients live longer with multiple chronic diseases, polypharmacy, multimorbidity, and frequent transitions between hospitals, clinics, and home care make it much easier for dangerous mismatches to arise between past and newly prescribed medications. When records are fragmented and medication histories are incomplete, prescribers often cannot see the full trajectory of what a patient has been taking, which increases the risk of serious adverse drug events when new drugs or doses are introduced. Health card systems and nationwide medication history?sharing programs have emerged as practical responses to this problem, giving Pharmacists and physicians a rapid access to near?complete medication histories that can alter treatment decisions in time?critical settings such as acute coronary syndromes and emergency percutaneous coronary intervention (PCI) 2.
Central to this field is the idea that every prescription, refill, and dose adjustment should be informed not only by current symptoms and diagnoses but also by the patient’s lived history with medicines—what worked, what failed, and what caused harm. Health card systems, shared medication?history services, and AI?enhanced decision tools offer practical ways to bring that history to the bedside in seconds, allowing clinicians to make decisions that are both scientifically sound and deeply individualized 3.
The following real?world cases from the table illustrate how incomplete medication histories and incompatible therapies have caused serious harm.
Table 1: Real?world cases demonstrating need for pharmaco?cybernetics
|
Sl.no |
Patient Details |
Year |
Case Summary |
Reference |
|
1 |
Middle-aged woman with chronic pain and long-term opioid use, admitted for acute pain exacerbation with multiple comorbidities |
2020 |
Admitting team lacked complete prior opioid regimen details; physician ordered concentrated oxycodone at dose not reflecting tolerance, pharmacist assumed opioid-naïve status; led to over sedation and respiratory depression. Pharmaco-cybernetic solution: health card-linked history + AI dose-equivalence checking to flag mismatch. |
Yang A. Multifactorial Medication Mishap. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2014.4 |
|
2 |
200 adult ICU patients receiving IV medications, critically ill with polypharmacy |
2007 (Brazil ICU study) |
Simultaneous IV incompatible pairs (e.g., midazolam + hydrocortisone, cefepime combinations) accounted for 40.9% of drug-related problems, risking precipitation, occlusion, and therapeutic failure. Solution: EHR-integrated IV-compatibility CDSS for automated detection and alternatives. |
Vijayakumar A, Sharon EV, Teena J, Nobil S, Nazeer I. A clinical study on drug-related problems associated with intravenous drug administration. J Basic Clin Pharm. 2014 Mar;5(2):49-53. doi: 10.4103/0976-0105.134984. 5 |
|
3 |
Adults with acute coronary syndrome/ST-elevation MI needing urgent PCI, often unconscious/confused |
2024 evaluation (South Korea nation wide program) |
Pre-program: unknown prior antiplatelet/anticoagulant status complicated PCI/antithrombotic decisions. "Patient’s In-home Medications at a Glance" provided one-click history, reducing PCI time and improving decisions. Demonstrates health card-like sharing benefits. |
Cho J, Yoo S, Lee EE, Lee HY. Impact of a Nationwide Medication History Sharing Program on the Care Process and End-User Experience in a Tertiary Teaching Hospital: Cohort Study and Cross-Sectional Study. JMIR Med Inform. 2024 Mar 20;12:e53079. doi: 10.2196/53079. 6 |
|
4 |
Adults admitted to acute medical wards (prospective study) |
2023 (Europe tertiary hospital) |
Pharmacist-led best possible medication histories revealed frequent unintentional discrepancies (omissions, wrong doses, duplications) at admission, preventing ADEs. Highlights need for longitudinal history access. |
Vargas V, Blakeslee WW, Banas CA, Teter C, Dupuis-Dobson K, et al. (2023) Use of complete medication history to identify and correct transitions-of-care medication errors at psychiatric hospital admission. PLOS ONE 18(1): e0279903. 7 |
Within this context, pharmaco?cybernetics aims to coordinate interoperable information systems, health card infrastructures, artificial intelligence–driven analytics, and pharmacist?led processes so that each prescribing decision is guided by high?quality, longitudinal medication data rather than isolated snapshots from a single encounter. By embedding continuous feedback about outcomes, errors, and near?misses into these systems, pharmaco?cybernetics aspires to create a safer, adaptive cycle of prescribing, monitoring, and adjustment that can better protect patients from avoidable harm.
2. METHODOLOGY
2A. CYBER-PHYSICAL SYSTEMS IN PHARMACOCYBERNETICS PRACTICE
2A.1. Core Hardware Infrastructure Supporting Pharmaco-Cybernetics
2A.1.1. Workstation computers
All Pharmaco-cybernetics operations rely on high-performance desktop or laptop computers as their main processing units. These devices are necessary for the operation of Electronic Health Record (EHR), Clinical Decision Support Systems (CDSS), and Pharmacy Information Systems (PIS). They can multitask; retrieve data in real time, and process medications quickly because of their sophisticated computational abilities. Reliable workstation performance reduces processing delays, guarantees continuous pharmacy workflow, and supports accurate and effective patient care8.
2A.1.2. Mobile devices [Smartphones/ tablets]
Mobile phones can be used to access mobile health (mHealth) apps that help people take their medications as prescribed, be monitored remotely, and communicate digitally. These devices allow pharmacists to conduct telepharmacy consultations, perform virtual medication reviews, and verify drug information at the point of care. Patients may also use these devices for receiving dose reminders, managing medication schedules, scanning barcodes, and accessing online health records. Their portability enhances flexibility and promotes technology-enabled patient engagement9.
2A.1.3. Barcode Scanners and RFID [Radio Frequency Identification] Readers
Barcode and RFID technology are essential elements of Barcode Medication Administration (BCMA) and automated inventory management. Barcode scanners verify medication labels during dispensing and administration, ensuring adherence to the “five rights”: right patient, right drug, right dose, right route, and right time. RFID readers allow real-time tracking of medication movement within the pharmacy and improve stock accuracy. These tools significantly reduce the risk of human error and enhance the safety and reliability of medication distribution10.
2A.1.4. Automated Dispensing Cabinets (ADC)
Automated dispensing cabinets are safe, computerized devices for storing and retrieving medications that make dispensing procedures more efficient. ADCs guarantee accurate recording of prescription transactions, prevent stock inconsistencies, and lessen unlawful access. ADCs enhance audit capabilities, provide safer and more effective medication management, and automatically update inventory levels when coupled with PIS and EHR platforms 11.
2A.1.5. Server Infrastructure or Cloud-Based Computing Systems
Significant databases, patient profiles, medical records, and system apps are stored on servers or cloud-based platforms. Centralized storage, safe data backup and easy access to health information across several pharmacy departments or medical facilities are all made possible by these technologies. Furthermore, cloud-based systems improve scalability, which is crucial for telepharmacy, multi-branch hospital systems, and collaborative care settings as it allows several users to interact with real-time data at once 12.
2A.2. Software Architecture Supporting Pharmaco-cybernetics
2A.2.1. Electronic Health Records (EHR)
Electronic health records act as encompassing online databases of patient information, including prescription histories, laboratory findings, allergies, diagnoses, and practitioner notes. EHRs ensure pharmacists have access to current and correct data at the time of service, facilitating effective drug evaluation and minimizing therapy duplication. Clinical decision-making, communication, and flawless continuity of care are all boosted by their integration across healthcare units 13.
2A.2.2. Pharmacy Information Systems (PIS)
The primary component of software utilized in pharmacy operations is the Pharmacy Information System. Computerized order entry, drug interaction assessment, medication verification, and dispensing workflow management are all covered. Likewise, PIS tracks pharmaceutical utilization, automates inventory control, and keeps audit trails. These traits enhance precision, lower dispensing errors, and optimize the pharmacy's overall workflow14.
2A.2.3. Clinical Decision Support Systems (CDSS)
Real-time clinical alerts are provided by CDSS, via intelligent modules built into PIS or EHR systems. These include cautions about medication interactions, redundant treatment, contraindications, improper dosage, and modifications for hepatic or renal impairment. CDSS improves patient safety, encourages sensible drug usage, and helps professionals make knowledgeable treatment decisions by providing evidence-based recommendations15.
2A.2.4. Mobile Medication Management Applications
Apps for managing medications are used to encourage drug literacy and patient adherence. Features that involve dose reminders, pill monitoring, drug identification tools, educational resources, and safe patient-pharmacist contact are all provided by these apps. They assist pharmacists with remote monitoring while permitting patients to have an active role in their healthcare16.
2A.2.5. Database Management Systems (MySQL, Oracle, MS Access)
Structured clinical and pharmacy-related data is stored in database management systems. These platforms enable the development of centralized collections that offer individualized data retrieval, generate reports, and render performance monitoring straightforward. Sensitive health information is dealt with in a safe, dependable, and well-organized approach according to their sophisticated storage architecture17.
2A.2.6. Telepharmacy and Communication Platforms
Telepharmacy options offers remote consultations, prescription assistance, verification services, and follow-up monitoring when utilized with communication tools like Zoom, Microsoft Teams, or dedicated pharmacist-patient portals. Since they enhance access to crucial therapeutic care while maintaining constant interaction between patients and healthcare professionals, these systems are particularly advantageous for people in underserved or isolated regions18.
2B. METHODS TO IMPLEMENT PHARMACOCBERNETICS SYSTEMS
2B.1. System Architecture and Platform Design
2B.1.1. Interoperable Core Platform:
Develop a unified digital ecosystem that seamlessly links electronic health records (EHRs), pharmacy information systems (PIS), and clinical decision support systems (CDSS) with a dedicated health card module (physical smart card or secure digital wallet). The health card stores encrypted core identifiers (patient ID, demographics), key diagnoses, verified allergies, adverse drug reactions, and a summarized medication profile (active drugs, doses, durations) with secure hyperlinks to the full longitudinal history in the central EHR repository. This ensures rapid, portable access even in offline or cross?institutional scenarios, using standards like FHIR for interoperability.
2B.1.2. Pharmacist?Led Best Possible Medication History (BPMH) Capture:
At admission, transfer, and discharge, pharmacists systematically collect and reconcile medication histories using a structured process enhanced by the national history?sharing program (e.g., “Patient’s In?home Medications at a Glance”) and patient?facing tools like mobile apps or health card scans. AI?assisted reconciliation algorithms automatically compare patient reports, community pharmacy claims, and EHR data to flag omissions, duplications, and discrepancies, with pharmacist verification as the final step.
2B.2. AI?Assisted Medication History Analysis
Machine Learning Model Development: Train supervised and unsupervised ML models (e.g., random forests, neural networks) on de?identified historical datasets containing patient demographics, medication timelines, laboratory values, vital signs, and documented adverse events. Models learn to identify patterns linking specific drug combinations, dose ranges, and patient phenotypes (e.g., renal impairment, polypharmacy) to outcomes like acute kidney injury, serotonin syndrome, or bleeding events.
1. Retrieves the patient’s full medication history via health card/EHR linkage.
2. Compares the new proposal against past therapies, flagging incompatible or high?risk overlaps (e.g., prior NSAID + new anticoagulant).
3. Generates ranked alternatives with evidence?based rationale (e.g., “Switch to paracetamol; prior NSAID caused GI bleed”).
4. Suggests patient?specific dose adjustments based on organ function, weight, and pharmacogenomic data if available. Alerts are tiered by severity (interruptive for critical risks, passive for moderate) to minimize fatigue.
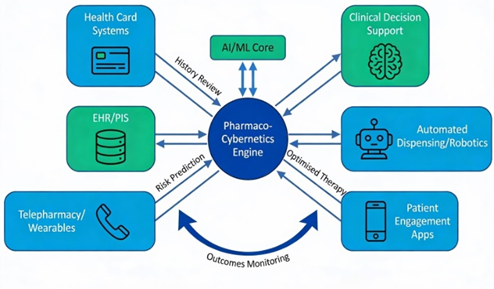
Fig.1 Conceptual Framework of
Pharmacocybernetics Systems
RESULTS AND DISCUSSION
A. Expected Clinical and Operational Outcomes of Pharmacocybernetics
1. Medication safety
Reducing pharmaceutical errors is the primary goal of Pharmacocybernetics. Bar-code scanning, automatic alarms and electronic prescribing are illustrations of technologies that help ensure that every patient gets the right drug at the right dosage. Electronic workflows that are standardized diminish the risk of miscommunication and handwritten mistakes. Enhanced digital tracking also makes it simpler to maintain track of earlier responses, allergies, and prescription histories, which assists in preventing catastrophic consequences.
2. Improved Clinical Decision-Making
Pharmacists can make safer and more precise treatment decisions by using electronic health records (EHRs) to access real-time patient information. Allergies, past medical history, current prescriptions, and lab results can all be swiftly reviewed. Drug interactions and improper dosages can also be warned about by decision support systems. This makes it easier for pharmacists to monitor the patient's reaction and suggest the best course of treatment.
3. Enhanced Efficiency
Pharmacists spend less time on tedious, manual tasks because of automation technology including robotics, automated dispensing cabinets, and electronic order processing. Pharmacists may utilize more time supervising patient care, including counselling, reviewing pharmaceutical therapy, and collaborating with other healthcare professionals, as these systems takes care of typical tasks. Faster service and more effective pharmacy operations stem from this.
4. Better Patient Engagement
Patients can stay more active in their own care with the help of digital tools like telepharmacy platforms, text message alerts, and prescription reminder apps. Reminders for visits, refills, and doses can be sent to patients. They can consult with pharmacists remotely via telepharmacy, which is especially advantageous for people who live in remote or underserved regions. Patients are encouraged to ask questions as necessary and to take their prescriptions as instructed.
5. Population Health Management
Informatics enables medical teams to concentrate on the health of large populations rather than just specific patients. Pharmacists can analyze prescription patterns, identify populations at risk for specific ailments, and keep an eye on trends in chronic diseases by evaluating data from EHRs, pharmacy databases, and public health systems. Planning health programs, upgrading treatment standards, and evaluating which drugs to add to the formulary can all benefit from this information.
B. Key Barriers to Pharmacocybernetics Adoption in Healthcare
1. Interoperability Issues
The inability of various health information systems to communicate seamlessly is one of the main problems in Pharmacocybernetics. Software from many suppliers is frequently used by hospitals, clinics, labs, and pharmacies; these systems are not necessarily compatible with one another. Important patient data, such as prescription histories, test findings, or allergy history, may therefore not move easily between platforms. Potential prescription errors, duplicate tasks, and missing data can result from this fragmentation. Coordinated system design, standardized data formats, and consistent communication protocols are crucial for ensuring interoperability19.
2. High Implementation Costs
It can be costly to implement Pharmacocybernetics systems. Expenses include recruiting IT professionals, upgrading infrastructure, buying devices and software, and performing ongoing system maintenance. This technology may be too costly for smaller hospitals, community pharmacies, and organizations with limited resources. The long-term expenses of updates, licenses, and employee training might be substantial even in cases when funding is available. The adoption of cutting-edge digital systems is frequently slowed down or limited by these financial obstacles.
3. Workflow Disruptions
New technologies can cause short-term disruptions to current workflows. Employees may need to pick up new procedures and adjust to changes in their daily responsibilities. Pharmacy operations may slow down during the first transition phase, orders may take longer to complete, and staff may become frustrated while they get used to the new system. Troubleshooting, system testing, and training sessions can all take up time and resources. These interruptions may have an impact on productivity and potentially jeopardize patient safety if they are not properly planned20.
4. Data Security and Privacy
Sensitive patient data is maintained in vast quantities due to the growing usage of digital tools and electronic health records. Cyber-attacks, data breaches, unauthorized access, and unintentional data loss are all possible threats to these digital systems. Strong cyber security techniques, including encryption, secure user authentication, frequent system updates, and staff data protection training, are necessary to ensure patient privacy. Healthcare firms must also abide by privacy laws, which can be difficult to maintain and require a lot of resources21.
5. Technology Acceptance
The adoption and utilization of Pharmaco-cybernetics by healthcare professionals is a critical factor in its success. Some employees may be reluctant to implement new systems because they are unfamiliar with them, are afraid of taking on more work, or worry that technology will take their jobs. Others might like more conventional paper-based approaches. Effective training, staff participation in system design and selection, and transparent communication of the technology's advantages are all necessary for fostering user confidence. The effectiveness and impact of the informatics system may be diminished if resistance continues.
C. Emerging Trends in Pharmaco-cybernetics
1. Artificial Intelligence and Machine Learning
Artificial intelligence (AI) and machine learning (ML) are expected to play a major role in transforming pharmacy practice. These technologies can analyze large sets of health data to identify patterns, predict patient outcomes, and assist in early detection of medication-related problems. AI-driven systems may streamline processes such as medication reconciliation by automatically comparing prescriptions and patient histories to identify discrepancies. Furthermore, ML algorithms can support personalized medicine by suggesting drug therapies tailored to a patient’s unique characteristics, medical conditions, and treatment responses22.
2. Block chain Technology
Block chain technology offers a secure and transparent way to manage medication-related information. Because block chain records are decentralized and cannot be easily altered, they can help protect patient data from tampering and unauthorized access. This makes block chain useful for ensuring the integrity of medical records, verifying the authenticity of medications, and improving the safety of the pharmaceutical supply chain. By tracking drugs from manufacturers to pharmacies, block chain may reduce the risk of counterfeit medications and improve overall trust in medication distribution systems23.
3. Health Card Systems
Health card systems will evolve into universal digital passports containing complete medication histories, allergies, pharmacogenomic data, and active regimens, accessible via NFC/smartphone for seamless cross?institutional prescribing and emergency care; integrated with AI for instant risk assessment and dose guidance24.
4. Pharmacogenomics Integration
Pharmacogenomics, or the study of how genes influence drug response, will become more and more integrated into standard clinical practice in Pharmacocybernetics. Pharmacists will be able to choose drugs and dosages that are more closely matched to each patient's unique genetic profile by integrating patients' genetic data with electronic health records and decision support systems. This individualized strategy can promote more effective medication management, lessen adverse drug responses, and increase treatment efficacy25.
5. Advanced Telehealth Services
It is anticipated that telehealth would grow considerably, providing pharmacists with new chances to provide care from a distance. Pharmacists may be able to manage pharmaceutical therapy, conduct virtual consultations, and monitor chronic illnesses in real time with the help of advanced telepharmacy platforms. Wearable technology and digital treatment tools can gather patient data and transmit it straight to medical professionals, enabling pharmacists to take action sooner when problems occur. These technologies will enhance continuity of care and help reach underprivileged populations with pharmaceutical services26.
6. Robotics and Smart Hospitals
Robotics and smart hospital technologies will further modernize medication distribution and compounding processes. Next-generation robots may be capable of preparing complex sterile products, managing inventory, and performing repetitive dispensing tasks with high precision. Smart hospital systems equipped with automated transport vehicles, sensor networks, and integrated data platforms can streamline pharmacy logistics and reduce human error. This level of automation allows pharmacists to focus more on clinical responsibilities while enhancing overall efficiency and safety within healthcare institutions27.
7. Emerging Role of Pharmaco-cybernetics in India’s Digital Health Ecosystem
Pharmaco-cybernetic systems in India should be integrated with the Ayushman Bharat Digital Mission (ABDM) to enable secure, interoperable, and patient-centric healthcare delivery, using the Ayushman Bharat Health Account (ABHA) number as a unique digital identifier to link prescriptions, dispensing records, and clinical outcomes. Leveraging ABDM infrastructure allows real-time data exchange among hospitals, pharmacies, laboratories, and regulators, improving medication traceability, reducing prescription errors, preventing duplicate therapies, and ensuring continuity of care. Additionally, ABDM-aligned systems support population-level pharmacovigilance through anonymized drug utilization and adverse drug reaction data, strengthening drug safety monitoring and regulatory oversight by agencies such as CDSCO, while empowering patients with access to their medication histories and enhancing informed clinical decision-making.
CONCLUSION:
ACKNOWLEDGEMET:
The authors express their sincere gratitude to all individuals and institutions who contributed to the successful completion of this work. We acknowledge the support, guidance, and resources provided by the faculty and management, which were instrumental in carrying out this study.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest associated with this manuscript.
FUNDING
NIL
REFERENCES


Vijaya Sindhuri Gopu*, Sujeev Kumar K, Vasavi Pachika, Pharmacocybernetics: Technology-Supported Information Systems in Patient Care Delivery and Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3384-3395. https://doi.org/10.5281/zenodo.18409586
 10.5281/zenodo.18409586
10.5281/zenodo.18409586