Pranveer Singh Institute of Technology (Pharmacy), Kanpur, Uttar Pradesh, India 209305
An ongoing state of hyperglycemia brought on by either insulin resistance or insufficiency, or both, is a hallmark of diabetes mellitus (DM), a chronic, complex metabolic disease. Long-term therapy is still difficult because of side effects, poor effectiveness, and the inability to avoid ?-cell loss, even with the availability of several synthetic antidiabetic medications. Combinations of several medicinal plants, or polyherbal preparations, have drawn a lot of interest recently as useful substitutes or supplements to traditional therapy. By acting on a variety of target molecules, such as nuclear factor erythroid 2-related factor 2 (Nrf2), AMP-activated protein kinase (AMPK), insulin signaling (IRS/PI3K/Akt), and peroxisome proliferator- activated receptor gamma (PPAR-?), these formulations improve insulin sensitivity, promote ?-cell regeneration, and lower oxidative stress and inflammation. Herbs such as Gymnema sylvestre, the plant Momordica Trigonella foenum-graecum, Curcuma longa, Cucumis sativus, and Lagenaria siceraria have phytochemicals that contribute to these synergistic effects, including flavonoids, alkaloids, terpenoids, and saponins. Additionally, polyherbal therapy exhibits potential as a supplement to contemporary medicine, enhancing glycemic control and reducing adverse drug reactions. Widespread clinical adoption is hampered by issues including standardization, quality control, and insufficient clinical validation. The evidence-based use of polyherbal formulations can be facilitated through the integration of contemporary statistical, Pharmacological, and regulatory frameworks, providing a safe, economical, and comprehensive approach to long-term diabetes care.
Diabetes mellitus (DM) is a chronic, multifactorial metabolic disorder characterized by a persistent elevation in blood glucose levels (hyperglycemia) resulting from defects in insulin secretion, insulin action, or a combination of both. Insulin, a peptide hormone produced by the β-cells of the pancreatic islets, plays a crucial role in maintaining glucose homeostasis by facilitating the uptake and utilization of glucose in peripheral tissues such as muscle and adipose tissue, while simultaneously inhibiting hepatic glucose production. When insulin secretion is inadequate or the body’s tissues become resistant to its action, glucose accumulates in the bloodstream, leading to sustained hyperglycemia and various metabolic abnormalities. Diabetes mellitus (DM) is a collection of metabolic syndromes that are characterized by hyperglycemia. The underlying causes of these syndromes can vary from insulin resistance linked to overweight and lifestyle factors (as observed in Type 2 DM) to autoimmune damage to pancreatic β-cells (as seen in Type 1 DM). The disorder is a multifactorial and systemic condition that is impacted by a complex interplay of genetic susceptibility, triggers in the environment, sedentary lifestyle, unhealthy eating habits, and obesity. Diabetes has become the one of the more significant public health issues of the twenty-first century within the last few decades. Rapid urbanization, decreased levels of exercise, and the global trend toward processed, high-calorie foods are all major contributors to its rising prevalence in both industrialized and developing countries. The disease affects people of all ages and socioeconomic backgrounds, and because of its progressive nature and related complications, it places a significant burden on healthcare systems as well as the global economy (1).
The International Diabetes Federation (IDF) Diabetes Atlas, 10th edition (2023) estimates that 537 million individuals (aged 20–79) worldwide today have diabetes, and that figure is expected to increase to 643 million by 2030 and 783 million by 2045. The primary causes of this concerning rise include growing urbanization, obesity, sedentary behavior, and changes in lifestyle [2]. Nearly 80% of all occurrences of diabetes occur in nations with low to middle incomes, which have a disproportionately larger burden of the disease. Probably the most affected are the Western Pacific and South-East Asian regions, with China and India having the highest rates of diabetes. According to the Indian Council of Medical Research (ICMR)–INDIAB Study (2023), more than 101 million persons in India alone have diabetes [3]. These patterns suggest that diabetes has spread to epidemic proportions, severely taxing national economies and healthcare systems [4]. Equally worrisome is the financial cost of diabetes. Approximately USD 966 billion was spent on diabetes care worldwide in 2021, a 316% rise over the previous 15 years (5). This financial burden results from indirect expenses including lost productivity, disability, and early death in addition to the direct costs of medical treatment, insulin, and antidiabetic medications. In addition to hyperglycemia, diabetes is linked to a number of microvascular and macrovascular problems that greatly raise morbidity and mortality, such as nephropathy, neuropathy, retinal disease, cardiovascular diseases, and stroke. Diabetes is one of the top 10 causes of death worldwide, according to the World Health Organization (WHO), and it causes over 6.7 million deaths per year. Due to their capacity to target several pathogenic processes responsible for diabetes, traditional medical systems—especially herbal and multi herb formulations—have attracted increasing interest. Therefore, investigating polyherbal techniques as supplemental or alternative therapies in diabetes care requires an assessment of the worldwide prevalence of diabetes [5].
Insulin, sulfonylureas, biguanides (like metformin), thiazolidinediones, α-glucosidase antagonists, DPP-4 inhibitors, and SGLT-2 inhibitors are examples of modern antidiabetic medications that are useful in reducing hyperglycemia and slowing the progression of the disease, but they have a number of clinical and pharmacological drawbacks that limit the long-term treatment of diabetes mellitus [6]. Unwanted side effects including hypoglycemia, gastrointestinal distress, weight gain, hepatotoxicity, and elevated cardiovascular risk are linked to several of these medications, which jeopardize patient compliance and quality of life [7]. Furthermore, rather than addressing the underlying pathophysiological abnormalities such β-cell malfunction, insulin resistance, oxidative stress, and low-grade inflammation, the majority of currently available medications mainly target symptomatic glycemic management [8]. Consequently, they are unable to stop the gradual decrease of β-cell mass and function that is seen in T2DM. Additionally, long-term use of synthetic medications can lead to pharmacological tolerance and decreased therapeutic efficacy, which frequently calls for combined therapy or dose escalation and increases the risk of adverse events [9]. The financial burden of ongoing medication and frequent clinical evaluation is another significant drawback. This is especially problematic in nations with low to middle incomes, where access to reasonably priced medications and healthcare facilities is still restricted [10]. Furthermore, none of the medications now on the market may totally prevent or repair diabetes-related microvascular and macrovascular consequences such nephropathy, neuropathy, retinopathy, and cardiovascular diseases, despite ongoing developments in pharmacotherapy [11]. These drawbacks have led to a growing shift in research focus toward poly herbal preparations and plant-based bioactives, which provide multi-targeted mechanisms with reduced side effects and better safety profiles, including improved insulin secretion, increased insulin sensitivity, prevention of glucose absorption, and decreasing oxidative stresses [12].
Due to their multiple modes of action, low adverse effects, and cost-effectiveness when compared to synthetic pharmaceuticals, herbal medicines have drawn a lot of attention as prospective treatment options for management of diabetes mellitus [13]. Herbal medicines work in a variety of ways, such as improving the pancreatic β-cell function, stimulating insulin secretion, improving glucose uptake through GLUT-4 translocation, inhibiting intestinal digesting carbohydrates enzymes, and lowering oxidative stress, in contrast with conventional diabetes medications that primarily target blood glucose levels [14]. They are especially useful in treating complicated metabolic diseases like type 2 DM because of these multitargeted processes[15]. Additionally, a number of polyherbal preparations have shown synergistic effects improving efficacy while reducing side effects—by combining numerous medicinal plants with complimentary processes [16]. The incorporation of herbal medications and multiple herbal formulations into contemporary therapeutic frameworks shows promise for creating safe, economical, and successful therapies for long-term diabetes control, given the growing prevalence of diabetes worldwide and the shortcomings of existing pharmacotherapy [17].
Traditional medical systems like Ayurvedic and Traditional Chinese Medicine, which place a strong emphasis on combining several herbs to achieve increased therapeutic efficacy and decreased toxicity, are the source of the idea of polyherbal formulation [18]. singular herb formulations frequently target specific metabolic pathways in the treatment of diabetes, while polyherbal mixtures incorporate a variety of bioactive chemicals that work in concert to modify several systems related to glucose metabolism [19]. Polyherbal preparations are justified by their capacity to produce combination or synergistic therapeutic benefits, in which various phytochemicals enhance the actions of one another, such as increasing insulin secretion, enhancing insulin sensitivity, suppressing α-glucosidase activity, and lowering oxidative stress [20]. Additionally, by balancing the possible toxicity of the individual components, the inclusion of numerous substances can reduce side effects and enhance tolerance and safety [21].Because some phytoconstituents may improve the stability or absorption of others, polyherbal formulations also improve bioavailability and pharmacodynamic efficacy. A. This all-encompassing strategy treats the underlying pathophysiological disorders linked to diabetes, such as inflammatory disorders, dyslipidemia, and β-cell dysfunction, in addition to the symptoms management of hyperglycemia [22].
It is caused by intricate relationships between environmental triggers, lifestyle choices, and genetic predisposition, all of which interfere with the metabolism of fats and carbohydrates [23]. While Type 2 diabetes mellitus is characterized by insulin resistance, decreased insulin production, and progressive β-cell failure, Type 1 diabetes mellitus (T1DM) is characterized by an absolute lack of insulin due to autoimmunity destruction of pancreatic β-cells [24]. A hyperglycemic condition is maintained when peripheral tissues, especially the muscles of the skeleton, the fat cells, and the liver, become less sensitive to insulin. This leads to decreased glucose absorption and raised liver production of glucose [25]. Reactive oxygen species (ROS) and inflammatory cytokines, including TNF-α and IL-6 are produced in excess, which disrupts mitochondrial function and insulin signaling pathways, further compromising glucose homeostasis [26].Through pathways including advanced glycation end-product (AGE) accumulation, polyol pathway activation, and oxidative mitochondrial damage, prolonged hyperglycemia is associated with microvascular (retinopathy, nephropathy, neuropathy) and macrovascular (atherosclerosis, coronary artery disease) complications [27].
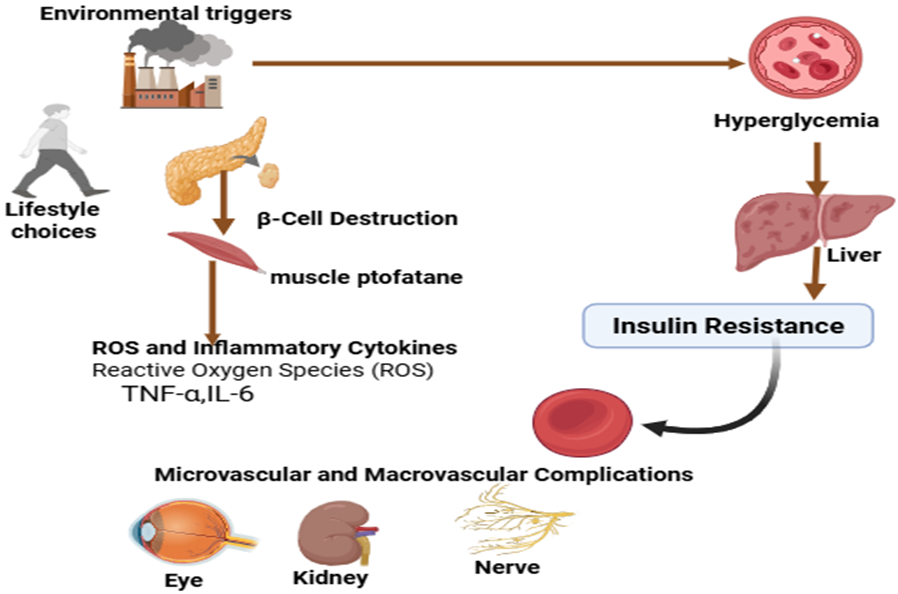
Fig. No. 1: Pathophysiology of Diabetes Mellitus (DM)
2.1 Glucose Homeostasis
Managing a normal blood glucose level and cellular energy supply requires a specific equilibrium between glucose production, consumption, and storage, which is known as glucose homeostasis [28]. Insulin and glucagon, which are secreted by pancreatic β- and α-cells, respectively, work in concert to regulate the process [29].Increased blood glucose levels following a meal stimulate the release of insulin. Through GLUT-4 translocation, insulin enhances the absorption of glucose in muscular and adipose tissues and stimulates the formation of glycogen in the liver, which lowers blood glucose levels. In contrast, glucagon promotes hepatic glycogen breakdown and gluconeogenesis in order to maintain euglycemia following fasting or energetic deprivation [30]. Resistance to insulin, insufficiency, or both can upset this delicate equilibrium in diabetes mellitus, resulting in chronic hyperglycemia. Comprehending glucose homeostasis facilitates the identification of therapeutic targets for the restoration of sensitivity to insulin and β-cell function. Polyherbal formulations exhibit potential because of their minimal adverse reactions and multiple targeting mechanisms [31].
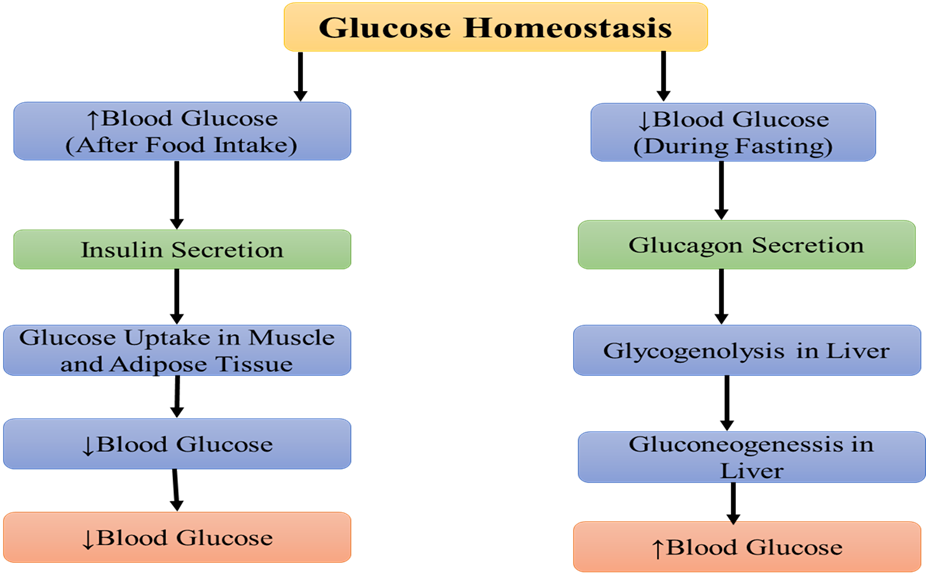
Fig. no.2: Glucose Homeostasis
2.2 Mechanisms Leading to Insulin Resistance and β-Cell Dysfunction
The two main flaws in the pathophysiology of type 2 diabetes mellitus are resistance to insulin and β-cell dysfunction. The muscles of the skeleton, adipose tissue, and the liver are examples of insulin-responsive tissues that develop resistance to insulin when they do not react to insulin sufficiently, which results in decreased glucose absorption and greater production of glucose in the liver [32].Insulin receptor signaling is disrupted by long-term exposure to high levels of free fatty acids and pro-inflammatory cytokines like TNF-α and IL-6, especially through serine phosphorylation of insulin receptor substrate (IRS) proteins, which reduces GLUT-4 translocation and glucose utilization [33]. Moreover, oxidative damage is a major factor in the formation of β-cell malfunction and resistance to insulin. Overproduction of reactive oxygen species (ROS) damages mitochondria and triggers stress signaling mechanisms that suppress insulin signaling and encourage β-cell death [34].Endoplasmic reticulum (ER) stress, glucotoxicity, and lipotoxicity all contribute to the development of β-cell dysfunction by decreasing insulin expression of genes, secretion, and β-cell mass. Thus, by comprehending these pathways, polyherbal compositions with anti-inflammatory, antioxidant, and sensitizing properties might be designed to effectively manage diabetes [35].
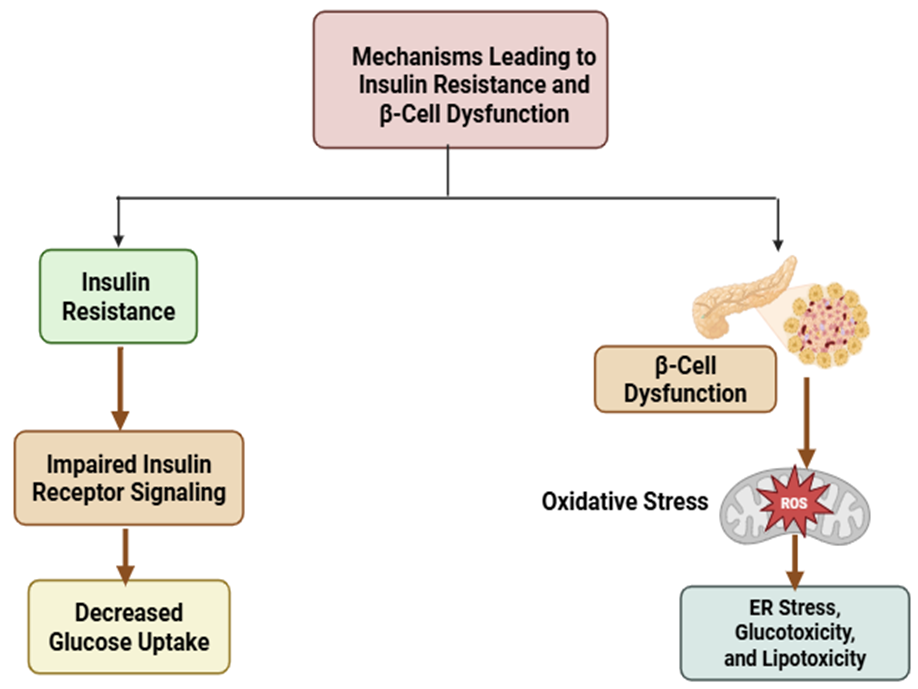
Fig.no.3: Mechanisms Leading to Insulin Resistance and β-Cell Dysfunction
The bioactive secondary metabolism products found in medicinal plants, also known as the phytochemicals, are a large and structurally varied class of natural substances that play a major role in controlling insulin action and glucose homeostasis. These chemicals act as protection mechanisms against stress caused by the environment, pathogens, and herbivores but have no direct role in developing plants or reproduction. It's interesting to note that many of these very same biochemical characteristics have therapeutic benefits for people, especially for metabolic diseases like diabetes mellitus[36]. Some glycemic control-related phytochemicals presented in (Table no.1).
Table no. 1:-Glycemic Control-Related Phytochemicals and Their Mechanisms
|
Sr. No |
Phytochemical Class |
Mechanism of Action |
Plant Sources |
References |
|
1.
|
Flavonoids |
Improve the sensitivity of insulin and production; suppress α-glucosidase and α-amylase; increase GLUT-4 translocation; and lessen the impact of oxidative stress. |
Camellia sinensis, Citrus limon, Trigonella foenum-graecum |
[37] |
|
2. |
Alkaloids |
Boost insulin sensitivity, inhibit the gluconeogenesis of the liver, and activate pancreatic β-cells. |
Berberis aristata, Catharanthus roseus |
[38] |
|
3. |
Terpenoids
|
Activate PPAR-γ and AMPK pathways, improving glucose uptake and lipid metabolism. |
Momordica charantia, Gymnema sylvestre |
[39] |
|
4.
|
Saponins
|
Reduce inflammatory responses, increase the receptors for insulin sensitivity, and delay the absorption of carbohydrates by blocking α-glucosidase. |
Panax ginseng, Tribulus terrestris |
[40] |
|
5. |
Phenolic acids |
Reduce postprandial glucose levels, block enzymes that hydrolyze carbohydrates, and shield β-cells from harm caused by reactive oxygen species (ROS). |
Cinnamomum verum, Syzygium cumini |
[41] |
|
6. |
Tannins |
Delay the absorption of carbohydrates, suppress intestinal α-amylase, and shield β-cells from oxidative damage. |
Syzygium cumini, Punica granatum |
[42] |
|
7. |
Lignans |
Minimize lipid peroxidation, increase antioxidant enzyme activity, and enhance hepatic glucose metabolism |
Linum usitatissimum (flaxseed), Sesamum indicum |
[43] |
Due to its capacity to identify active ingredients, standardize dosages, and conduct mechanistic research, single-herb therapy which uses extracts or extracted bioactive substances from a single plant species has been extensively used in both traditional and contemporary phytotherapy for diabetes. Pharmacokinetic profiles and regulatory review are made easier by the comparatively large amount of a recognized active (such as berberine, charantin, or the gymnemic acids) that single-herb formulations can supply [44]. comparative overview of Polyherbal and Single-Herb Therapy presented in (Table no. 2).
Table.no. 2:- A Comparison of Polyherbal and Single-Herb Therapy for the Management of Diabetes
|
Sr. No. |
Parameter |
Single-Herb Therapy |
Polyherbal Therapy |
References |
|
1. |
Definition |
Uses a single medicinal plant's components or extraction for a particular therapeutic purpose.
|
Contains two or more herbs to produce complementary or synergistic effects for the treatment of complex diseases. |
[45] |
|
2 |
Mechanism of Action |
Primarily affects one or a small number of molecular targets such as inhibiting enzymes or the production of insulin. |
Modifies several mechanisms, including oxidative stress, β-cell protection, and sensitivity to insulin. |
[46] |
|
3 |
Efficacy |
Restricted ability to manage complex diabetes. |
Improved response to glucose, antioxidants, and inflammation. |
[47] |
|
4 |
Clinical Scope |
Ideal for research that is both target-based and mechanistic.
|
It requires clinical validation but shows promise for multiple target, holistic therapy. |
[48] |
4. Polyherbal Formulations for Diabetes: Evidence and Mechanisms
Due to its capacity to target several molecular pathways at once, polyherbal compositions have drawn increasing attention as a comprehensive therapeutic approach for diabetic mellitus, especially type 2 diabetes [49]. Polyherbal combinations combine the pharmacological actions of several phytoconstituents, including flavonoids, alkaloids, terpenoids, and saponins, to produce synergistic glucose-lowering effects while reducing side effects, in contrast to single-herb treatments that work by one or two pathways. The effectiveness of poly herbal formulations in enhancing oxidative stress indices, the metabolism of lipids, and glycemic management has been shown in a number of clinical and preclinical investigations [50].Combinations of Gymnema sylvestre, Momordica charantia, Trigonella foenum-graecum, and Curcuma longa, for instance, have been demonstrated to increase insulin secretion, upregulate GLUT-4 expression, and block enzymes that break down carbohydrates, such as α-amylase and α-glucosidase. These results suggest that complementary mechanisms such as anti-inflammatory, anti-oxidative, and insulin-sensitizing effects can help multi-component herbal therapy restore glucose homeostasis [51].Mechanistically, poly herbal formulations have a "network pharmacology" effect by modifying signaling cascades such AMPK, PI3K/Akt, and PPAR-γ pathways, which together enhance β-cell protection and insulin sensitivity. The interaction synergy among bioactive ingredients has been further demonstrated by advanced computational research and metabolomic profiling, verifying conventional formulations using contemporary pharmacological frameworks. The standardization, quality assurance, and clinical verification of these intricate mixes continue to present difficulties despite encouraging outcomes. The absence of extensive randomized controlled trials, potential herb-herb interactions, and variability in the phytochemical composition are the main obstacles to regulatory adoption. For polyherbal formulations to be widely accepted in the therapy of diabetes, these problems must be resolved through quality-assured production and scientific validation [52].
4.1 Commonly Used Antidiabetic Plants and Polyherbal drugs
Polyherbal formulations can target several metabolic pathways at once, they are becoming more widely acknowledged as useful therapeutic approaches for the control of diabetes mellitus. Traditional and contemporary formulations have combined a variety of medicinal plants rich in bioactive chemicals, including alkaloids, flavonoids, terpenoids, phenolics, and saponins, to generate synergistic antihyperglycemic actions [53]. (Table no. 3).
Table no. 3. Herbs used in Diabetes Management
|
Sr. No. |
Herbs |
Mechanism of Action |
References |
|
1 |
Gymnema sylvestre |
Increases the production of insulin and encourages the renewal of pancreatic β-cells. |
[54] |
|
2 |
Momordica charantia |
Increases the absorption of glucose through GLUT-4 translocation and AMPK activation. |
[55] |
|
3 |
Trigonella foenum-graecum |
Increases the snsitivity to insulin by activating PPAR-γ. |
[56] |
|
4 |
Curcuma longa |
Lowers oxidative stress as well as inflammation while promoting insulin sensitivity and β-cell defense. |
[57] |
|
5 |
Tinospora cordifolia |
Improves the transmission of insulin and metabolism of glucose while acting as an antioxidant. |
[58] |
|
6 |
Cucumis sativus |
enhances consumption of glucose and has antioxidant and β-cell protecting properties. |
[59] |
|
7 |
Lagenaria siceraria |
improves metabolic function, increases production of insulin, and lowers oxidative stress. |
[60] |
4.2 Synergistic Mechanisms of Polyherbal Combinations
Through the synergistic interactions of several naturally occurring phytochemicals that target different metabolic pathways involved in signaling via insulin and glucose regulation, polyherbal formulations achieve their antidiabetic effects. This multi-target strategy reduces the drawbacks of a single compound therapy while increasing therapeutic efficacy [61].
Enhancement of Insulin Secretion
A number of herbal mixtures increase the insulin production and release via stimulating pancreatic β-cells. For example, both experimental and clinical investigations have demonstrated that the leaves of Gymnema sylvestre, Tinospora cordifolia, and Momordica charantia enhance β-cell regeneration and upregulate insulin gene expression. Gymnemic acids, alkaloids, and saponins found in these botanicals enhance insulin production triggered by glucose [62].
Improvement of Insulin Sensitivity
Insulin-sensitive herbs like Trigonella foenum-graecum, Curcuma longa, and Zingiber officinale are frequently used in polyherbal blends. These herbs activate the AMPK and PPAR-γ pathways, which increases insulin receptor activation and glucose absorption in skeletal muscle and adipose tissue. Better periphery insulin response and glycemic control follow from this [63].
Modulation of Glucose Transporters (GLUT-4)
Another method of polyherbal synergy is the stimulation of glucose transporters proteins, particularly GLUT-4 in adipose tissue and skeletal muscle. GLUT-4 translocation to the cell membrane is facilitated by bioactives such curcumin, catechins, and flavonoids from Momordica charantia and Cinnamomum verum, which aid in effective glucose absorption [64].
Inhibition of Carbohydrate-Metabolizing Enzymes
Strong inhibitory effect against α-amylase and α-glucosidase enzymes is demonstrated by polyherbal mixes containing Syzygium cumini, Aegle marmelos, and Trigonella foenum-graecum. This delays the intestinal absorption of glucose and the digestion of carbohydrate. This process helps to lower hyperglycemia after eating [65].
Antioxidant and Anti-inflammatory Pathways
By scavenging reactive oxygen species (ROS) and raising endogenous anti-oxidant enzyme levels like SOD, CAT, and GPx, the synergistic antioxidant actions of polyherbal mixtures combat oxidative stress. Furthermore, β-cells are shielded from death and insulin activity is maintained by anti-inflammatory effects through regulation of NF-κB and cytokines (TNF-α, IL-6) [66].
5.Phytochemical and Pharmacological Insights
Flavonoids, alkaloids, terpenoids, saponins, and phenolic acids are just a few of the many phytochemicals found in polyherbal formulations used to treat diabetes. These compounds work in concert to restore glucose homeostasis. These bioactive substances affect a variety of biological targets, such as improving insulin sensitivity, increasing insulin production, inhibiting digesting enzymes, and shielding pancreatic β-cells from oxidative damage.
Quercetin, rutin, and catechins are examples of flavonoids with potent anti-inflammatory and antioxidant properties that enhance peripheral tissue glucose consumption and inhibit β-cell death [67]. Tinospora cordifolia and Gymnema sylvestre alkaloids promote β-cell renewal and insulin release. By increasing GLUT-4 translocation and triggering AMPK signaling pathways, terpenoids and saponins present in Momordica charantia and Trigonella foenum- graecum improve glucose absorption. By scavenging reactive oxygen species (ROS) as well as upregulating antioxidant defense enzymes like superoxide dismutase (SOD) and catalase (CAT), phenolic compounds like curcumin and gallic acid reduce oxidative stress, improving insulin sensitivity and metabolic balance. Together, these phytochemicals act on complementary mechanisms to achieve comprehensive glycemic control, establishing the pharmacological basis for the efficacy of polyherbal medications in the treatment of diabetes [68].
5.1 Molecular targets and signaling pathways
By influencing numerous molecular targets and pathways of cell signaling involved in glucose metabolism, insulin signaling, and oxidative stress management, polyherbal formulations effectively treat diabetes. Compared to single-compound therapy, this multi-targeted approach decreases inflammation, improves insulin sensitivity, and supports β-cell function. The insulin receptor substrate (IRS)-PI3K-Akt pathway is activated by a number of polyherbal combinations, which improves GLUT-4 translocation to the plasma membrane in adipose tissue and skeletal muscle, hence promoting glucose uptake [69]. Bioactives like Momordica charantia's flavonoids, Trigonella foenum-graecum's saponins, and Curcuma longa's curcumin increase insulin receptor phosphorylation and boost insulin sensitivity. Adenosine monophosphate-activated protein kinase (AMPK), a crucial regulator of glucose and lipid metabolism, is activated by polyherbal mixtures rich in terpenoids and flavonoids in addition to insulin signaling [70]. AMPK activation improves glycemic control by increasing fatty acid oxidation, suppressing hepatic gluconeogenesis, and promoting glucose absorption in peripheral tissues. In addition to improving receptors for insulin sensitivity in adipose tissue and raising adiponectin levels, phytochemicals like fenugreek alkaloids and gingerols also affect peroxisome proliferator-activated receptor gamma (PPAR-γ), which aids in glucose management and lowers diabetic dyslipidemia [71]. Additionally, polyherbal preparations target redox and inflammatory signaling pathways, such as NF-κB, Nrf2, and MAPK cascades, which results in the upregulation of antioxidant enzymes like catalase and superoxide dismutase (SOD) and the suppression of pro-inflammatory cytokines like TNF-α and IL-6. This combined antioxidant and anti-inflammatory action preserves oxidative balance, shields pancreatic β-cells from apoptosis, and stops further insulin resistance. Overall, the synergistic antidiabetic activity of polyherbal preparations is based on the regulation of several interrelated molecular pathways: IRS/PI3K/Akt, AMPK, PPAR-γ, and Nrf2 [72].
6. Future Perspectives and Challenges
In order to transform traditional knowledge into standardised, evidence-based medications, polyherbal therapies for diabetes must incorporate contemporary analytical tools and systems-level methodologies. Network pharmacology, metabolomics, and high-resolution phytochemical profiling developments will make it possible to predict herb-herb and herb-drug interactions, identify active ingredient clusters, and rationally create synergistic formulations with enhanced safety and efficacy. To guarantee reproducibility and compliance with laws across manufacturers and markets, strong quality control utilizing proven chemical markers, fingerprinting (HPLC/LC–MS), and batch release criteria would be crucial [73]. In order to show clinical benefit and persuade regulators and clinicians of therapeutic value, it is imperative to advance from small exploratory research to adequately powered randomized controlled trials (RCTs) with standardized formulations, clear endpoints (HbA1c, fasting plasma glucose, insulin sensitivity indices), and long-term safety monitoring. In order to identify uncommon side effects and herb-drug interactions in practical applications, post-marketing pharmacovigilance techniques tailored for multiple- component botanical products are equally crucial. Lastly, precision phytotherapy—matching polyherbal formulations to patient endotypes (insulin-resistant vs. insulin-deficient phenotypes) using biomarkers and complementary diagnostics and integrating proven multiple herbal regimens with conventional pharmacotherapy and lifestyle in integrated care models should be the focus of future research. Transforming promising polyherbal science into safe, efficient, and widely available diabetes treatments will require addressing these scientific, legal, and practical issues [74].
6.1 Potential of polyherbal therapy as adjunct to modern medicine
A new supplementary strategy to managing diabetes is polyherbal therapy, which may work in concert with traditional antidiabetic medications to improve treatment results. Combining bioactive phytoconstituents from several herbs can affect various molecular targets, including PPAR-γ, AMPK, and GLUT-4, which can improve insulin sensitivity, increase glucose uptake, and reduce oxidative stress [75]. Co-administration of standardized polyherbal preparations with metformin or glibenclamide has been demonstrated in recent research to improve glycemic indicators, lipid profile, and antioxidant enzymatic levels more successfully than individual therapy. By minimizing the likelihood of adverse effects including hypoglycemia or gastrointestinal intolerance, such synergistic benefits may allow traditional medication dosage reductions [76]. Additionally, developments in metabolomics and pharmacogenomics are assisting in the prediction of possible pharmacokinetic interactions and the identification of herb-drug combination that are compatible, enabling a safer integration into contemporary medical practice. However, before complete therapeutic integration, issues including the absence of standardized formulations, the paucity of large-scale clinical studies, and potential herb-drug interactions must be resolved by thorough study and regulatory validation. Consequently, polyherbal preparations have great potential as supplements to contemporary medication for all-encompassing diabetes care when they are standardized and experimentally verified [77].
7. CONCLUSION
By focusing on several molecular pathways, such as insulin signaling, oxidative stress, and inflammation, multiple herbal formulations provide a comprehensive and scientifically promising approach to the management of diabetes mellitus. In contrast to traditional monotherapy, these formulations incorporate the synergistic effects of several phytochemicals that preserve pancreatic β-cells, improve glucose absorption, and increase insulin secretion. Polyherbal treatments can increase efficacy, reduce adverse effects, and enhance overall metabolic balance when taken in conjunction with conventional antidiabetic medications. But obstacles including inconsistent plant-based composition, lack of standardization, and inadequate clinical validation need to be addressed. In order to establish safety, efficacy, and regulatory approval, future research using new analytical, pharmacogenomic, and clinical techniques will be essential. All things considered, polyherbal therapy is a secure, efficient, and long-lasting supplement to contemporary diabetic treatment.
REFERENCES



Km Monee, Nishant Kumar, Nandani Yadav, Polyherbal Approaches for the Management of Diabetes, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 4088-4103. https://doi.org/10.5281/zenodo.19354237
 10.5281/zenodo.19354237
10.5281/zenodo.19354237
