Pharmacy (Pharmaceutics) Department, Sikkim Skill University.
Fat-based treatment delivery systems have shown great potential in considering the delivery of moderately soluble drugs only. The limited solubility of these molecules in water makes oral lipid-loving medications very difficult. Since, when it comes to oral administration of slightly water-soluble drugs, methods of delivery of fat-based drugs have shown an excessive amount of potential. The solubility phase, which may be a problem that limits the oral absorption rate of insufficiently soluble drugs in water, is eliminated when the drugs are pre-dissolved in oils, surfactants, lipid mixtures and surfactants. The choice of lipid excipients and the dosage form greatly affect the biopharmaceutical aspects of drug absorption and distribution in both the laboratory and In-vivo because oils differ not only in their structures and physicochemical appearance but also in their digestion and absorption pathway. SMEDDS or micro emulsifying auto emulsifying drug delivery systems have gained recognition for their ability to improve the solubility and bioavailability of easily insoluble drugs. In the current action, the micro- self-emulsifying drug delivery system (SMEDDS) has been developed to increase oral bioavailability and solubility rate for both lipophilic and hydrophilic drugs. The goal of the project is to develop a precisely optimized self-emulsifying drug delivery system (SMEDDS) poorly water-soluble drug. A preliminary screening was executed to identify the best mix of several excipients for the formulation. The significance of numerous independent variables on dependent (response) variables was examined using a 32 execute factorial design. Oil concentration and Smix ratio were the independent variables and dependent variables, which include emulsification time (s), drop size (nm), polydispersity index , and zeta potential (mV), studied in the current work.
The solubility of the drug, the dissolution, and its gastrointestinal lumen permeability of poorly soluble drugs are requisite factors that control the amount of absorption speed, along with the bioavailability of the drug[1]. In drug research and development, the poor solubility of therapeutic candidates results in a number of problems. A drug's rate of dissolution is significantly influenced by its aqueous solubility; low solubility frequently causes oral drugs to dissolve poorly and have low bioavailability; and drugs with aqueous solubilities less than 100 g/ml typically have dissolution-limited absorption. [2]. Today, more than 50% of newly discovered chemical entities that are pharmacologically active are lipophilic and have poor water solubility, which is a result of advances in modern drug discovery techniques[3]. Oral route is most favored and convenient route and avoid the drawbacks of parenteral delivery, nearly 35-50% of new drugs that are introduced in the pharmaceutical company have poor water solubility which will makes it difficult to develop an ideal oral dosage form. To overcome these strategies several reports have been developed like cyclosporin, permeation enhancer, and solid dispersion, micelles. But in recent last 10 to 15 years, there have been significant advancements that have gained attention in lipid-based drug delivery (LBDD)[4]. BCS(Biopharmaceuticals Classification System) considers dissolution, solubility, and intestinal permeability as the three main variables that control the rate and amount of absorption from immediate release solid oral dose forms (absorption)[5].
BCS: Biopharmaceutics Classification Systems
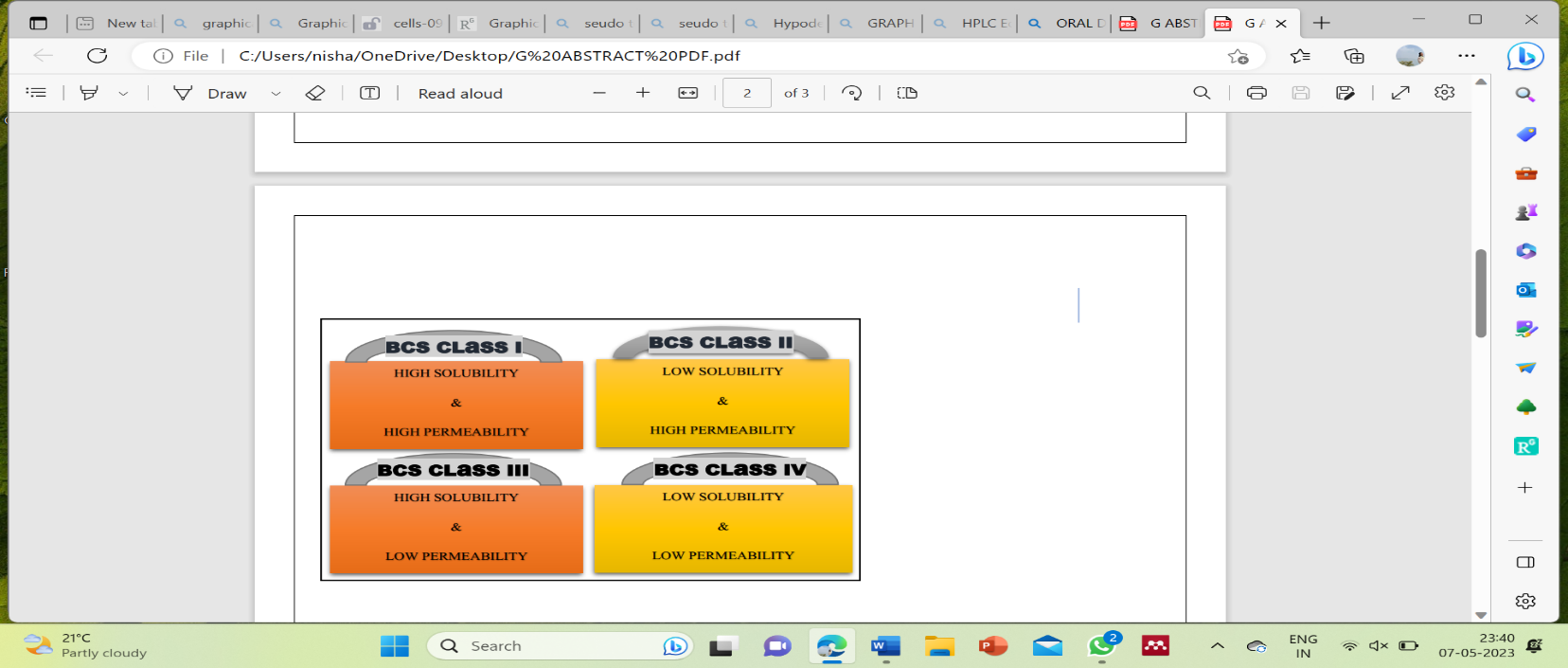
Based on the BCS, drugs are classified into four categories according to their solubility and permeability assets as follows, class I (high solubility–high permeability); class II( low solubility– high permeability ); class III (high solubility–low permeability); and class IV (low solubility– low permeability), BCS class II drug exhibit the low solubility but practical high membrane permeability belong to BCS class II (A, fenofibrate, cyclosporin, Aceclofenac, ritonavir (RTV) etc. [6][7,8]. Usually, techniques used for BCS class II drugs do little to improve the absorption of class IV drugs due to the limited membrane permeabilities. The best way to increase the bioavailability of class IV medications is to return to the lead optimization stage of drug development and change the way they are built so that they have the right physicochemical properties. [6].We suggest the following three qualities for the ideal BCS permeability class reference drug, a) The ideal marker medicine should ideally be nonionizable, b)have a fraction dose absorption in the range of 90%, and c) Be absorbed mostly by passive transcellular permeability with no/minimal carrier-mediated active intestinal transport (influx or efflux)[9]. BCS classification system, poorly water-soluble drugs are categorized as Class-II. In these, the absorption process's dissolution is rate-limiting stage. Oral administration of such medications, the key issue is to increase drug solubility and dissolution. High lipophilicity and extremely low water solubility are characteristics of a biopharmaceutics classification system (BCS) Class IV molecule[10], and BCS Class IV are more likely to show extremely high inter- and intrasubject variability due to their weak solubility and permeability. Thereby, they are typically poor oral medication candidates unless the drug dose is indeed very low[11]. Formulation strategies are necessary to improve its solubility and oral bioavailability[12].The solubility properties of poorly water-soluble pharmaceuticals have been improved through the development of numerous approaches. Some of these include solvent change co-precipitation , solid dispersion , inclusion complexes with β-cyclodextrins, nanosuspensions, microencapsulation , soluble salts formation , lyophilization and liquid-solid technique[7]. Amorphous formulations include "solid solutions," unlike other solubilization techniques, amorphous formulation has the ability to increase apparent solubility without hampering permeability, and therefore achieving and maintaining supersaturation without modifying the equilibrium solubility of the drug.[12,13]. Solid dispersion can be defined as “dispersion of one or more active ingredients in an inert excipient or matrix, where the active ingredients could exist in finely crystalline, solubilized, or amorphous states” [13]. Solid lipid nanoparticles (SLN) have recently attracted a lot of attention because of their capacity to improve bioavailability while also enabling precise and targeted drug delivery. They are therefore used as likely candidates for carriers of oral intestinal lymphatic delivery. Liposomes are the most complex category of lipid-based drug delivery systems, and they have been shown to improve the efficacy of a variety of difficult-to-deliver medications[6]. These liposomes demonstrated high permeability to the nuclear membrane as well as the cell membrane[14]. Emulsion-based is one of the first techniques for delivering lipophilic medicines. Microemulsions and Nano emulsions are the two types of emulsions now being used to increase the oral bioavailability of poorly soluble drugs. The special properties include great industrial scalability (due to low energy needs for manufacture), super solvency, tiny droplet size, thermodynamic (microemulsions) or kinetic (nano emulsions) stability, and utilization of lipidic excipients as absorption enhancers[6,15].
Lipid Based Formulations:
Lipid based formulation have gained increasing interest in pharmaceutical field because of their potential to improve the bioavailability of drug molecules which are poorly soluble in water[6]. A common requirement for all the types of lipid formulation is that they should be able to keep the drug in the solubilized form in the gastrointestinal tract (GIT)[16]. The term "solubility refer the amount of solute that dissolves in a given amount of solvent ." The drug solubility is the dissolution rate at which the drug molecule or the dosage form allows for entering the solution, and it is essential when the time of dissolution is restricted[1]. Lipid-based formulation techniques, specifically the self-emulsifying drug delivery system (SEDDS), are widely known for their potential as an alternate technique for the delivery of hydrophobic drug, which are associated with poor water solubility and low oral bioavailability [17]. SEDDS is one of the techniques used to enhance the oral bioavailability of poorly soluble medications by delivering and sustaining the drug dissolved in micro droplets of oil during its transit through the gastrointestinal system (GIT)[18]. Microemulsions formed by the SMEDDS exhibit good thermodynamics stability and optical transparency.
Types Of Self Emulsifying Drug Delivery System:
Self-emulsifying systems, self-micro-emulsifying systems, and self-nano emulsifying systems are among the types of these systems (SEDDS, SMEDDS, and SNEDDS). When added to an aqueous medium while being gently stirred, these stable isotropic mixtures of (natural/synthetic) oil, (solid /liquid) surfactant, and co. surfactant results in the formation of fine O/W emulsions, micro-emulsions, and nano-emulsions, respectively. The outcome was that these formulations were distributed easily into the GIT, where the stomach's motility produces the necessary agitation for self-emulsification[17,19].
(Self Emulsifying Drug Delivery System)SEDDS : SEDDS are simple binary compositions of a drug and a lipophilic phase that are thermodynamically unstable in aqueous or physiological conditions or lipophilic phase, surfactant & drug. Lipid droplets between 200 nm and 5 um are provided by SEDDS formulations, increasing the surface area available for absorption. Dispersion seems turbid, and a ternary phase diagram is primarily used in the construction of SEDDS. The HLB value of the surfactant used in SEDDS is under 12[19].
(Self-Micro-Emulsifying Drug Delivery System) SMEDDS: SMEDDS not only provides the same benefits as emulsions in terms of aiding hydrophobic drug solubility, but also deals around the issue of emulsions creaming over time. SMEDDS may be conveniently stored since it is component of a system that is thermodynamically stable[18]. SMEDDS are isotropic mixtures of natural or synthetic oils, solid or liquid surfactants, and hydrophilic cosolvents/co-surfactants that have the unique ability to create fine oil-in-water (o/w) microemulsions with mild agitation followed by dilution in aqueous media, such as GI fluids[20].
SNEDDS: are droplets smaller than 50 nm that are created by a moderate agitation of an isotropic combination of oil, surfactant, and co. surfactant to create an O/W emulsion. In SNEDDS, the excipients—which produce nanodroplets—are broken down. These droplets formed greater surface areas, which are available for the absorption of poorly water-soluble medications, as a result of lower interfacial tension. Moreover, SMEDDS/SEDDS require a higher concentration of the surfactant, whereas SNEDDS require a surfactant with an HLB value of at least 12[19].
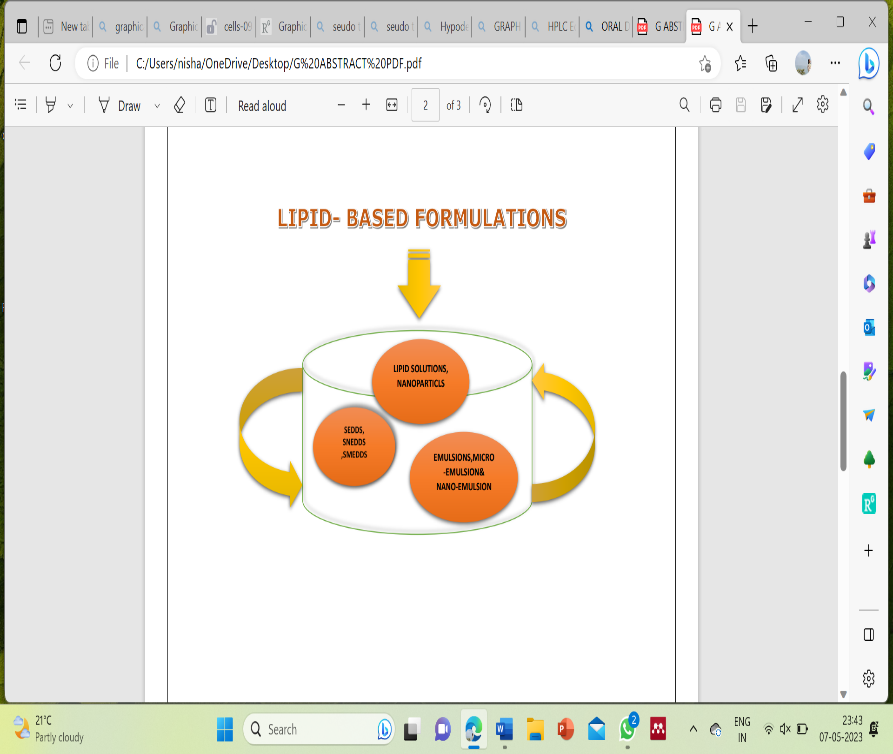
Fig:1 Lipid-based formulations often used in drug delivery.
Merits:
Demerits:
Factors Affecting the SMEDDS Formulation
If a drug does not have very high solubility in any one of the components of SMEDDS, especially the lipophilic phase, it is not suitable for SMEDDS. The most challenging medications to deliver via SMEDDS are those with limited solubility in water and lipids (usually with log P values around 2. The solubility of the drug in oil phase has a significant impact on SMEDDS' potential to keep the drug in the solubilized state. Previously stated, if a surfactant or co-surfactant plays a more significant part in the solubilization of a medication, there may be a risk of precipitation since the dilution of SMEDDS will reduce the solvent capacity of the surfactant or co-surfactant[21]. Equilibrium Solubility measurements subsequently could be done to predict potential scenarios of intestinal precipitation[18].
The polarity of the lipid phase is one of the variables that determines the rate at which drug released from microemulsions. The fatty acid's chain length and degree of unsaturation, the molecular weight of micronized for their tendency to prevent crystallization and, as a result, develop and maintain the supersaturated state for extended periods of time, and the polarity of the droplet is governed by the HLB[21].
The drug's oil phase solubility has a significant impact on SMEDDS's potential to keep the drug in dissolved form. The dilution of SMEDDS can cause the solvent capacity of the surfactant or co-surfactant to be minimized resulting in precipitation when the drug is solubilized using surfactant and co-surfactant[22].
Mechanism Of Self-Emulsification (SMEDDS)
Self-emulsification's mechanism is still not completely understood. However, Reiss asserts that self-emulsification develops when the entropy change that favours dispersion is greater than the energy used to increase the surface area of the dispersion. Additionally, a traditional emulsion's free energy may be characterized by an equation and is a direct function of the energy needed to establish a new surface between the two phases[23].

Methodology [Preliminary Test]: -
The solubility of poorly soluble drugs in various solvents (oils, surfactants, and co-surfactants) is the most critical parameter for the screening components for nano emulsion. As, the objective of this study is to create an oral formulation, although the medication's solubility in oils is particularly essential because it directly affects the nano emulsion's potential to sustain the drug in its solubilized state[24].
Method: Determination Of Solubility (API):
Solubility of poorly soluble drugs in different solvents (oils, surfactants, buffers and co-surfactant) was examined by shake-flask method and sonication. An accurately measured 5 ml of each solvent separately was taken in a vial. To each vial, an excess amount of drug was added and properly sealed, stirred using vortex mixer for 15 min and then sonicated for a period of 2 h to attain equilibrium[25].The samples that had been equilibrated were taken out of the shaker and centrifuged at 3000 rpm for 15 minutes. A 0.45 lm membrane filter was used to filter the supernatant, followed by filtration. The filtrate was suitably diluted with methanol and drug dissolved in various vehicles was analysed by UV spectrophotometer[24,26].
construction of calibration curve in 0.1n HCL and 6.8 PH phosphate buffers:
Drugs which has a concentration of 1000 g/ml, was dissolved in 10 ml of volumetric flask using the appropriate buffer. A concentration of 10 g/ml was obtained by diluting 1 ml of the stock solution to 100 ml. Following dilutions of this stock solution in buffer were performed to obtain 5g/ml, 10g/ml, 15g/ml, 20g/ml, 25g/ml, etc. The maximum absorbance was monitored at α max

Drug -Excipients Compatability Study: -
The chemical interaction between the medicine and excipients can be done with the aid of the IR spectrum, in the wavelength range of 4000-400cm-1 by using FTIR spectrophotometer method. To examine any potential interactions between the medicine and the excipient, the IR spectra of the physical mixture was compared to that of the pure drug[27]
Selection of Surfactant and Co-Surfactant: -
The mixture was slowly heated at 45–60°C to uniformly mix the components and were brought to 25- 30 ?C by leaving at room temperature. The isotropic mixture of each component was accurately weighed and diluted with distilled water to yield a fine emulsion. The emulsions were then allowed to stand for 2 h, and transmittances were assessed using UV spectrophotometer with distilled water as blank. The emulsion had been visually analysed for the presence of turbidity or phase separation[25].
The simple to comprehend microemulsion system's phase behaviour is studied using a pseudo ternary phase diagram. These diagrams are useful for determining the self-micro emulsifying regions and for modifying the concentration of the oil and the emulsifier to co-emulsifier ratio. A triangular representation of a pseudo ternary phase diagram can be used, with each corner of the diagram representing 100% of each component. When using pseudo-ternary phase diagrams, a corner will often stand in for a binary mixing of two components, such as surfactant/ co-surfactant, water/drug, and oil/drug[20]. The methods are used to plot ternary phase diagrams are namely Dilution method and Water Titration method are shown in Figure 2.
Water Tritration Method: - At room temperature, homogenous liquid solutions of oil, surfactant, and cosurfactant with water were titrated to create the pseudo ternary phase diagrams. Oily mixes of oil, surfactant, and co-surfactant were created in ratios ranging from 9:1 to 1:9 and weighed in the identical screw-cap glass tubes before being vortexed. Each mixture was then slowly titrated with drops of distilled water and stirred at room temperature to attain equilibrium[28].
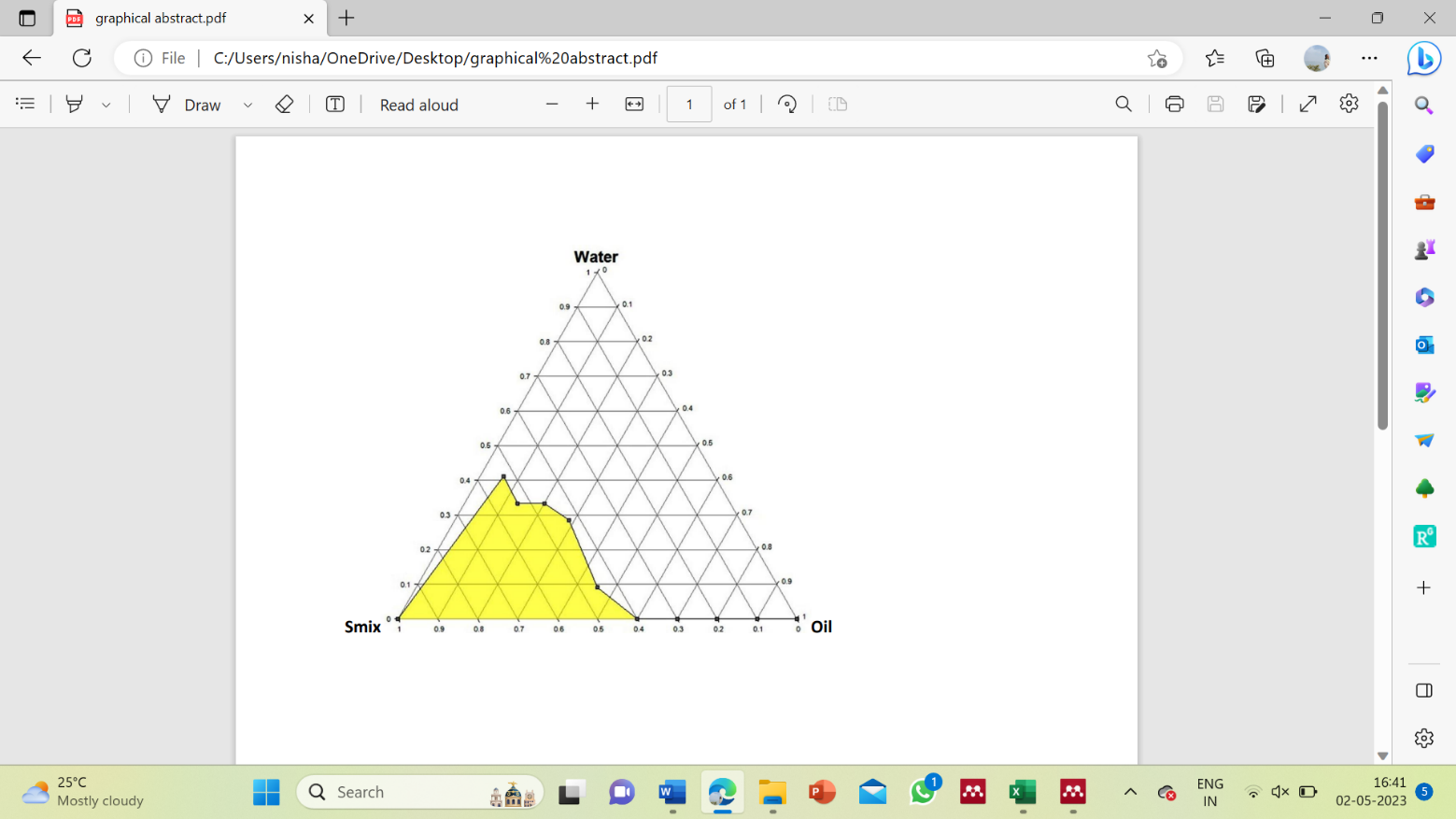
Fig:2 Pseudo-ternary phase diagrams of o/w micro-emulsion region at different ratios[24].
Composition Of (Self Micro-Emulsifying Drug Delivery System) SMEDDS:
Ideal Drug (API) Candidate Used in Smedds Formulation:
The Biopharmaceutics Classification System is a helpful tool for pre-formulation decision-making from a biopharmaceutical standpoint (BCS)[29]. For medications in BCS classes III, or I formulations are created using a straightforward methodology. Contrarily, to achieve a satisfactory and uniform bioavailability following oral administration, BCS class II or IV medications necessitate careful formulation designs based on the pharmaceuticals' physicochemical and biological features[2]. The pace at which a BCS class II medicine dissolves determines how much of it is bioavailable. As a result, a slight increase in the dissolving rate might occasionally lead to a considerable increase in bioavailability. BCS class II medicines are typically characterised by low solubility and high permeability in their chemical composition. Transcellular passive transport accounts for the majority of drug absorption from oral administration[30,31]. The rate at which pharmaceuticals dissolve is positively impacted by increased saturation solubility and effective surface area, and efforts to improve these parameters during pre-formulation research and formulation design could do so. Boosting the drug's dissolving rate will increase the bioavailability of BCS class II drugs[29]. It is believed that crystal modification, particle size reduction, self-emulsification, pH manipulation, and amorphization can improve how BCS class II drugs dissolve [32]. Others are only suitably solubilized in solutions that are fully organic and comprise either one solvent or a combination of solvents/surfactants, whereas other poorly water-soluble compounds are sufficiently solubilized in solutions comprising an aqueous/organic cosolvents [33].
Excipients Used in SMEDDS Formulation:
Considering, pharmaceutical acceptability and the toxicity issues the selection of excipients is great issues and really critical[28].Self-emulsification has been proven to be specific to the nature of the oil/surfactant and co-surfactant; the surfactant concentration and oil/surfactant and co-surfactant ratio; and the temperature at which self-emulsification develops. Also, supporting these facts it has been shown that only extremely precise pharmaceutical excipient combinations could result in effective self-emulsifying systems[34,35]. Although it is necessary to evaluate the relative solubility and affinity of the drug for each component in the design of SEDDS/SMEDDS, the importance should be on the system's overall solubilizing power rather than the solubility of the drug in each component separately. The oily phase, surfactant, and co-surfactant are three components that can be natural, semi-synthetic, or synthetic[27].
Lipids/Oils: -
Oils consider the most important excipients used in the formulation of SMEDDS[37]. Dietary oils composed of medium and long chain triglycerides are frequently utilized in lipid-based formulations, along with a variety of solvents and surfactants. Having both a lipophilic (fatty acid) and a hydrophilic part, many lipids are amphiphilic by nature[14]. Depending on the molecular nature of the triglyceride, oils can solubilize the lipophilic part of drug, aid in self-emulsification, and also enhance the proportion of the drug delivered by the intestinal lymphatic system, improving absorption from the GI tract[28]. Naturally occurring oils and fats are comprised of mixtures of triglycerides which contain fatty acids of varying chain lengths and degrees of unsaturation. Triglyceride vegetable oils have many advantages as the foundation of self-emulsifying drug delivery systems. They are commonly ingested in food, fully digested and absorbed, and therefore do not present any safety issues and generally regarded as safe (GRAS)[36]. Triglycerides can be further classified as long chain triglycerides (LCT), medium chain triglycerides (MCT) and short chain triglycerides (SCT)[38]. Vegetable oils are glyceride esters of mixed unsaturated long-chain fatty acids, commonly known as long-chain triglycerides (LCT). In recent years, much attention has been focused on MCT for the formulation of SMEDDS. MCT is easy for digestion as compared to LCT, which converts to diglycerides, monoglycerides, and free fatty acids. This conversion is facilitated by several gastric and intestinal enzymes like lipase, pancreatic lipase, etc[20]. Such as fractionated coconut oil and palm seed oil, as well as triglycerides of caprylic/capric acid, such as Miglyol 812 and Captex 355, are used in the development of a self-emulsifying system[20]. MCT have a higher solvent capacity than LCT and are less prone to oxidation[39]. Medium chain mixed glycerides are not susceptible to oxidation, have greater solvent capacity and promote emulsification[14].
Surfactants: -
In order to facilitate the dispersion process during the preparation of SEDDS, the surfactant of choice must be able to lower interfacial tension to a very low value, provide a flexible film that can easily deform around the droplets, and be of the appropriate lipophilic character to provide the correct curvature at the interfacial region [36]. Surfactants are amphiphilic and they can dissolve/solubilize a relatively high amount of hydrophobic drug compounds[20]. The high HLB and subsequent hydrophilicity of surfactants is necessary for the immediate formation of o/w droplets and rapid spreading of the formulation in the aqueous environment, providing a good dispersing/self-emulsifying performance. Surfactants used in\SMEDDS are mainly a) non-ionic, b) anionic, c) cationic or zwitterionic Surfactants. In comparison to cationic and anionic surfactants, these non-ionic surfactants are less harmful. The compounds with an HLB value greater than 10 are commonly regarded as non-ionic surfactants and are responsible for producing fine, uniform emulsion. Each dosage form's formulation should take into account the fact that any excipients used in the formulation might not be harmful to the patient. The most commonly used surfactants for self-emulsifying formulation are emulsifiers with a natural source, including polyoxyl 35 castor oil (Cremophor EL), polyoxyl 40 castor oil (CremophorRH40), polysorbate 80 (Tween 80), etc., are less dangerous than those with a synthetic source-soluble[20].
A predetermined group of lipid excipients with an intermediate hydrophilic-lipophilic balance adsorb at the oil-water interface (HLB, 8–12). They can create emulsions when sheared and are sometimes called "dispersible" in water. Although these substances can form micelles, they don't have enough hydrophilicity to self-emulsify[14].
These surfactants are most typically used to create self-emulsifying medication delivery systems. Materials with an HLB value of around 12 or higher can produce micellar solutions at low concentrations by dissolving in pure water over their critical micellar concentration[14]. These compounds can be created by mixing polyethene glycols and hydrolysed vegetable oils (PEG). Ethylene oxide reacts with a common substitute alcohol to produce alkyl ether ethoxylate (for example, cetostearyl alcohol ethoxylate, or cetomacrogol)[40].
The use of a single surfactant is infrequently produce transiently negative interfacial tension and use of high concentration cause GI irritation [36]. The co-surfactant and surfactant work together to reduce interfacial tension to an extremely low, briefly negative value. At this point, the interface would develop into finely dispersed droplets and then absorb additional surfactants and surfactant/co-surfactants until their bulk condition is sufficiently diminished to restore interfacial tension to its original positive value. In the absence of a co-surfactant, the surfactant forms a highly stiff film and can only produce microemulsion within a very narrow concentration range. Co-surfactants give the interfacial film the flexibility it needs to adapt to the various deformations needed to create microemulsion throughout a wide range of compositions[36]. Since alcohol and other volatile co-solvents in the traditional self-emulsifying formulations are known to migrate into the shells of soft gelatin or hard sealed gelatin capsules, resulting in the precipitation of the lipophilic drug, these systems may exhibit some advantages over the other formulations when incorporated in capsule dosage forms[28]. Co-solvents effectively dissolve the hydrophobic drug or hydrophilic surfactant in the lipid base. In some cases, these solvents serve as co-surfactants in microemulsion systems. Common cosolvents include polyethylene glycol 400, propylene glycol, ethanol, and glycerol. Polyoxyethylene, propylene carbonate, tetrahydrofurfuryl alcohol, polyethylene glycol ether (glycofurol), and other substances are additional cosolvents[20].
Statistical Optimization of Self Micro Emulsifying Drug Delivery Systems
At first Bendse and Kikuchi presented a continuum technique to structural optimization of topology[41].It is generally accepted that full and fractional factorial designs at 2- and 3-levels are the most frequently utilized experimental designs in manufacturing organizations. A factorial design would let a researcher to investigate the cumulative effect of the factors (or process/design parameters) on a outcome. Both full and partial factorial designs are acceptable[42]. The application of conventional optimization methods to large-scale problems which require a lot of computational time to find the objective function for a given set of parameters can be extremely challenging. A DOE technique is used to create a response surface in order to get around this problem. In order to create a response surface on which to find the ideal condition, a set of appropriately selected design factors, in this case shape variables, are first taken. Effective computer use in optimization demands well-designed experiments to produce an appropriate surface[43].Design of Experiment (DOE) runs are selected in order to determine the response surface and identify the best optimal solution from among different possibilities[44]. In this optimization study, three DOE approaches have been employed: Latin Hypercube, Hammersley, and Box-Behnken[43].
Latin Hypercube design rn randomly samples the complete design space that is divided into equal probability zones(where r is the number of runs and n is the number of input variables) . Latin Hypercube design is particularly helpful for limiting the experiment to an established (user-specified) number of runs and for examining the interior of the parameter space. The objective of Hyper Study is to reduce the reciprocal correlation values to nearly zero.( Altair HyperStudy, Altair Engineering Inc., Troy, MI, 2011.)
Hammersley sampling is a productive sampling approach that provides accurate estimates of output statistics with a reasonable number of samples., Hammersley sampling, through the use a quasi-random number generator based on the Hammersley points one of the aspects of the quasi-Monte Carlo methods, to uniformly samples a unit hypercube. This has the advantage of having strong uniformity properties in just one dimension over Latin Hypercube sampling[43,45].
Box-Behnken designs are used to build higher order response surfaces with fewer runs than the conventional factorial approach. In order to maintain the higher order surface definition, this and the central composite approaches essentially suppress chosen runs. The Box-Behnken design fits a 2nd order equation with twelve middle edge nodes and three center nodes. With three extra samples obtained at the center, the central composite plus Box- Behnken creates a full factorial[43].
Formulation Optimization of Smedds Using D Optimal Design.
A three-part system the oil (oleic acid), the surfactant (Labrasol), and the co-surfactant (Transcutol HP), was used to develop the mixed experimental study.The range of oil (oleic acid), the surfactant (Labrasol), and the co-surfactant (Transcutol HP),was chosen based on the prior phase diagram results. The Design Expert version 8 program was used to input the values of independent variables, and a batch matrix was prepared. All the Batches were prepared and evaluated .The amount of medicine released cumulatively, after 15 minutes, release were used as responses, the mean droplet size, and the emulsification time[46]. To evaluate and optimize the main effects, interaction effects, and quadratic effects of the formulation ingredients on the desired responses, full factorial statistical modelling was used. For analysing quadratic response surfaces and designing a mathematical model, Design-Expert, software (Stat-Ease Inc., USA) was used. Model equation obtained by 32 factorial design was used to analyse multiple linear regression analysis (MLRA) involving independent variables and their interactions for measured responses[47].
Y ¼ β0 þ β1X1 þ β2X2 þ β3X1X2 þ β4X1 2 þ β5X2 2 þ β6X1X2 2 þ β7X1 2 X2 þ β8X1 2 X2 2 ….ð1Þ
Where, Y is the dependent variable; β0, the intercept, is the arithmetic average of all quantities outcome of 9 runs; β1to β8 are the regression coefficients; X1 and X2 are independent variables; and X1X2 and Xi 2 (i = 1, 2) are the interaction and polynomial terms, respectively[47]. In order to identify the significant main/interaction effects that affect process variability, we need to construct a coded design matrix as the response of interest[42].
ADVANTAGES-
DISADVANTAGES-
Physicochemical Characterization Parameters for Self-Emulsifying Formulations: -
Visual Evolution: -
The primary self-emulsification assessment method is a visual inspection[49]. After diluting or reconstituting the self-emulsifying formulations, the percentage of transparency of the resulting micro/Nano emulsion is measured using a UV-visible spectrophotometer [50].
Robustness To Dilution
To achieve a uniform drug release profile and to ensure that the drug won't precipitate at higher dilutions in vivo, which could significantly slow down the absorption of the drug from the formulation, robustness to dilution is essential for SEDDS/SNEDDS [21,51]. SEDDSs should be diluted at different concentrations for evaluation, and their impacts on the properties of the resulting emulsion or Nano emulsion should be investigated [50].
Zeta Potential: -
Zeta potential is used to calculate the charge of the droplets. It is critical to evaluate the oil droplet charge in SEDDS. An increase in the electrostatic repulsive forces between the droplets typically prevents the coalescence of microemulsion droplets.[50]. On the other side, phase separation happens when electrostatic repulsive forces weaken. Based on the electrophoresis and electrical conductivity of the produced nano emulsion, Malvern Zeta Sizer Nano is widely used to measure the zeta potential of reconstituted SEDDS.[52].
Effect of pH: -
The pH of the aqueous phase significantly affects the phase behaviour of spontaneously emulsifying systems. [53]. This calls for more investigation into how the pH of the aqueous phase impacts the final nano emulsion. [54].
Effect of Temperature: -
Studies show that self-emulsification is specific to the temperature at which it occurs[53]. As a result, it is also able to study how temperature influences globule size [50].
Centrifugation: -
Using this method, the stability of the SEDDS during emulsion formation may be assessed. For this, the samples are diluted with distilled water and centrifuged for a predetermined period at a predetermined rpm to determine the phase separation. As a result, it can also study how temperature influences globule size.[24,50].
Dye Solubilization Test: -
The self-emulsifying drug delivery mechanism can be explained using dye solubilization. The self-emulsifying drug delivery mechanism can be explained using dye solubilization. This is accomplished by applying the water-soluble dye to the surface of the created nano emulsion; keeping an eye on how the dye is dispersed, or forms clumps makes it possible to determine the kind of the emulsion's internal and external phases. [21].
Transmission Electron Microscopy (TEM): -
The Nano emulsion created via SEDDS is examined using transmission electron microscopy to determine its shape [12].
Cloud Point Measurement: -
When the temperature exceeds the cloud point due to the dehydration of the preparation's components, irreversible phase separation will occur, making the preparation hazy and impairing medication absorption. So, to avoid phase separation in the digestive system, the cloud point for SNEDDS should be above 370 C.[12,50].
Scanning Electron Microscopy (SEM): -
Scanning electron microscopy (SEM) (Supra 35 VP, Carl Zeiss, Germany) at 1000 magnification, working at 1 kV accelerating voltage, is used to study the morphology of s-SMEDDS and associated carriers.[55]
List Of BCS Class II and Class IV Drugs
|
Sl.no. |
Drug |
Category |
BCS Class |
Reference |
|
1. |
Aluminium Hydroxide |
Gastro Intestinal Agent |
IV |
[56,57] |
|
2. |
Albendazole |
Anti-Anthelminthic |
II |
[58] |
|
3. |
Abiraterone Acetate |
Anti androgen |
IV |
[59] |
|
4. |
Acetazolamide |
Anti Diuretic |
IV |
[56] |
|
5. |
Amphotericin B(Amb) |
Anti-Fungal |
IV |
[30] |
|
6. |
Aprepitant |
Anti-Emetic |
IV |
[60] |
|
7. |
Apigenin |
Anti-emetics |
II |
[61] |
|
8. |
Atorvastatin |
Anti-lipidaemia |
II |
[62] |
|
9. |
Baicalin |
Anti inflammatory |
II |
[63] |
|
10. |
Carbamazepine |
Anticonvulsant |
II |
[64] |
|
11. |
Carvedilol |
Anti-hypertensive |
II |
[65] |
|
12. |
Chlorthalidone |
Anti-Hypertensive |
IV |
[30] |
|
13. |
Ciprofloxacin |
Anti-biotic |
IV |
[66] |
|
14. |
Clofazimine |
Anti leprosy |
II |
[67] |
|
15. |
Curcumin |
Anti inflammatory |
IV |
[68] |
|
16. |
Colistin |
Anti-Microbial |
IV |
[30] |
|
17. |
Cyclosporin |
Immunosuppressive |
II |
[69] |
|
18. |
Danazol |
Anti-Estrogen |
II |
[70] |
|
19. |
Docetaxel |
Anti-Cancer |
IV |
[71] |
|
20. |
Domperidone |
Anti emetic |
II |
[46] |
|
21. |
Etravirine |
Anti-viral |
IV |
[72] |
|
22. |
Famotidine |
Anti-histamine |
II |
[73] |
|
23. |
Fenofibrate |
Antilipemic |
II |
[8] |
|
24. |
Furosemide |
Anti diuretic |
IV |
[74] |
|
25. |
Glyburide |
Anti-diabetics |
II |
[75] |
|
26. |
Indinavir |
Anti-viral |
IV |
[56] |
|
27. |
Ibuprofen |
Anti inflammatory |
II |
[26] |
|
28. |
Lopinavir |
Anti-HIV |
IV |
[7] |
|
29. |
Methotrexate |
Anti-cancer |
IV |
[76] |
|
30. |
Megestrol Acetate |
Anti-estrogen |
II |
[77] |
|
31. |
Nelfinavir |
Anti hypertension |
IV |
[56] |
|
32. |
Nilotinib |
Anti-cancer |
II |
[78] |
|
33. |
Nitrendipine |
Anti-hypertensive |
II |
[79] |
|
34. |
Paclitaxel |
Anti-cancer |
IV |
[71,80] |
|
35. |
Progesterone |
Anti Hormone |
II |
[36] |
|
36. |
Ritonavir |
Anti-viral |
IV |
[7] |
|
37. |
Saquinavir |
Antiviral |
IV |
[81] |
|
38. |
Telmisartan |
Antihypertensive |
II |
[82] |
|
39. |
Seocalcitol |
Anti neoplastic |
II |
[36] |
|
40. |
Valsartan |
Anti-hypertensive |
II |
[83] |
List Of Oil/Surfactants & Co-Surfactants Used in Smedds Formulation: -
|
Sl.no. |
Excipients(oils) |
Reference |
|
1 |
Corn oil, mono-, di-, triglycerides, |
[84] |
|
2 |
Capryol 90 (propylene glycol monocaprylate) |
[67] |
|
3 |
Captex 355 (glycerol caprylate caprate) |
[85] |
|
4 |
Capmul MCM L8 (glyceryl mono-dicaprylate1,2,3- propanetriol decanoic acid monoester) |
[36] |
|
5 |
Oleic acid/ethyl oleate |
[63] |
|
6 |
Soybean oil, Olive oil, Hemp oil |
[36] |
|
7 |
Labrafil M 1944 CS |
[36] |
|
8 |
Lauroglycol® 90 |
[36] |
|
Sl.no |
Excipients (surfactant) |
Reference |
|
1 |
Polysorbate 20 (Tween 20) |
[86] |
|
2 |
Polysorbate 80 (Tween 80) |
[76] |
|
3 |
Polyoxy-35-castor oil (Cremophor EL) |
[63] |
|
5 |
Polyoxy-40-hydrogenated castor oil (Cremophor RH40) |
[63] |
|
6 |
Polyoxyethylated glycerides (Labrafil M 2125 Cs) |
[87] |
|
7 |
Labrasol |
[63] |
|
8 |
Solutol HS-15 Sorbitan monooleate (Span 20) |
[88] |
|
9 |
Span 80 |
[76] |
Abbreviations
|
ABA-Abiraterone acetate |
|
AUC-Area under curve |
|
BCS-Biopharmaceuticals Classification Systems |
|
CMAX- Maximum plasma concentration |
|
FTIR-Fourier Transform Infrared Spectroscopy |
|
HPLC- High performance liquid chromatography |
|
LCT- Long chain triglycerides |
|
MCRPC- Metastaic castration resistant prostate cancer |
|
MCT-Medium chain triglycerides |
|
PEG-Polyethylene glycol |
|
SEDDS-Self emulsifying drug delivery systems |
|
SEM-Scanning electron microscope |
|
SMEDDS -Self Micro Emulsifying Drug Delivery Systems |
|
SMEDDS-Self micro emulsifying drug delivery systems |
ACKNOWLEDGEMENT:
I would like to express my sincere gratitude to all individuals and organizations who contributed to the successful completion of this A Systemic Review. First and foremost, I would like to thank Dr. Pragya Baghel whose guidance and support were invaluable throughout this project. Their expertise in Self-Emulsifying drug delivery systems provided me with the necessary insights and direction for this review. I also wish to acknowledge my HOD Dr. Sanjib Bahadur of Himalayan pharmacy institute for their assistance helped facilitate this research and enabled us to conduct a comprehensive review of the literature. My appreciation extends to all the researchers whose work is cited in this review. Without their significant contributions to the field of self-emulsification systems, this review would not have been possible. Lastly, I would like to thank our families and colleagues for their continuous support, encouragement, and understanding throughout this research process.
CONCLUSION
In this above review study, the solubility, dissolution, and gastrointestinal lumen permeability of poorly soluble drugs are the three main variables that control the rate and amount of absorption from immediate release solid oral dosage forms. BCS class II and Class IV drugs exhibit the low solubility.
REFERENCE


Nisha Limboo*, Divya Pradhan, Poor Aqueous Soluble Drugs; Challenges and Solution to Overcome with Self-Emulsification Systems: A Systemic Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 691-711 https://doi.org/10.5281/zenodo.15165250
 10.5281/zenodo.15165250
10.5281/zenodo.15165250
