1,2Smt. Tarawati Institute of Biomedical & Allied Science, Roorkee, India.
3Lala Lajpat Rai Memorial Medical College, Meerut, India.
A technique used to deliver medication to specific regions of the eye is known as ocular drug delivery. The goal of developing a medicine delivery system is to maximize effectiveness while reducing side effects. In the traditional ocular delivery method, noninvasive oral, topical, and ocular inserts are preferred over parental routes such as implants, systemic, intracameral, and subconjunctival. Using various chemical agents, API formulations—designated F1 were created for the investigation. Melting point of CTZ was found 142.2°C which complies with the reported literature 141-145°C. Which confirm that sample is CTZ. The conducted study of partition coefficient found 5.80±0.21 that CTZ. The sample of known concentration of the CTZ in PB 7.4 pH is stored in various temperature for the analysis of any change during storage condition for a definite period of 2 days at 25°C is initial too after same rang 0.105 and at 40°C is intail 0.105 after 0.107 nm and formulation f1heaving Hight drug releasing time 73.196±0.13.Transcorneal permeation study of opt formulation and it is expected that opt formulation show maximum permeation. Ocular irritancy is important and opt formulation should be non-irritant. opt formulation was proposed to sterilized by UV chamber and UV sterilized opt formulation is supposed undergo microbial test and expected that opt formulation may not show any microbial growth. Stability study of opt formulation is proposed as per ICH guidelines for general case at accelerated condition 40±2°C/75%RH±5RH.
Ocular drug delivery refers to a method employed to administer medication to targeted areas of the eye. A drug delivery system is designed and developed to optimize efficiency while minimizing adverse effects In conventional ocular delivery system, non-invasive Topical, Oral and Ocular Inserts are selected over Parental route like Systemic, Intracameral, Subconjunctival and Implants, due to ease of bulk scale manufacturing, high patient acceptability, drug product efficacy, stability and cost effectiveness. Among the non-invasive, Topical drug delivery are highly utilized as most of medical prescription includes conventional Topical eye drop, solution, suspension, ointment and gel. Topical ocular delivery systems are self- administrable and frequent dosing is possible if requested in contrast to Invasive delivery system which required skilled professional to administrate the drug. Solution, suspension, ointment and ophthalmic gel are popular dosage forms Topical ocular system.
1.1. Traditional surface-level eye medication delivery system
A diverse array of ophthalmic products is accessible in the market, with conventional eye drops comprising 70% of all prescriptions. Although the topical administration of medications appears to be the optimal route for delivering drugs, topical formulations must navigate various physicochemical barriers include drug lipophilicity, solubility, molecular size and biological barriers include pre-ocular barriers, corneal layers, systemic absorption from conjunctival capillaries system, blood aqueous barrier and blood retina barrier Topical eye drop, solution, suspension is commonly used but have limitations. Ointments offer advantage over eye drops such as increased contact time, reduced nasolacrimal drainage, minimization of tear dilution and higher effective concentration at site of application.[6] Main disadvantage is blurred vision however, the use of water- soluble bases called the gels has increased recently due to their advantage such as spreadability, stability and low irritancy. Consequently, the topical route is the most appropriate method for administering ocular formulations, provided that traditional ophthalmic formulations address the factors influencing drug absorption, permeability, and bioavailability [9] which can’t be achievable by conventional ocular dosage forms.
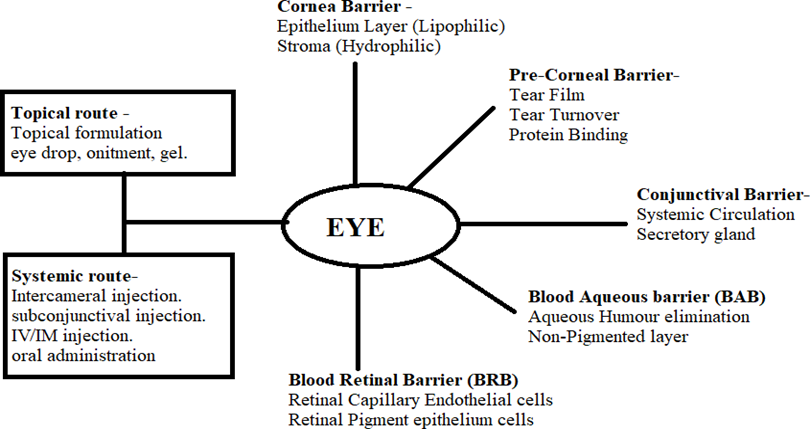
Fig 1.1: Administration Routes and Ocular Barriers
Human eye is a sophisticated sensory organ with complex physiology and anatomy being a sensory organ human eye is protected by various structural and functional defensive barriers which serve as a barrier and diminish the absorption and penetration of drugs administered via the topical route . The structural and functional defensive barriers are:
Human eye globe has pole to pole (anterior to posterior) diameter of 22mm to 27mm with circumference of 69 to 85 mm approximately, [17,18,19] Human eye can be split in two unequal segments. [8,1,6] Anterior Segment one-third of the eye and rest is Posterior Segment. Anterior Segment comprise of Cornea [16,11], Conjunctiva [20,21], Aqueous Humour [22,23], Iris [24], Ciliary Body [25] and Len [26,27]. Posterior Segment composed of sclera [8,28], Choroid [12,29], Retinal [30,31] and Vitreous Humour.
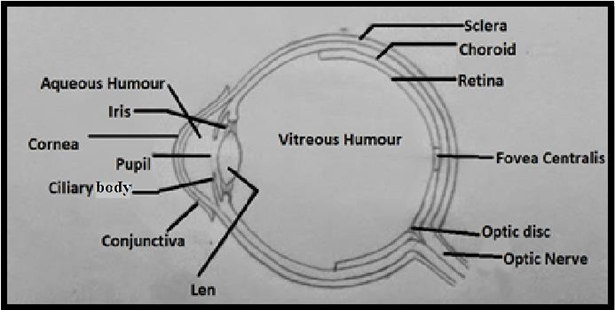
Fig 1.2: Diagram of Human Eye
Anterior segment consists of Anatomical barriers comprise of static barriers (Tear film, Corneal epithelium and stoma, blood aqueous barrier) and dynamic barriers (lymphatic and capillaries system of Conjunctiva) influence the absorption, penetration and ultimately bioavailability of drug administrated through topical route.
Tear film which is a pre-corneal barrier consist of three layers lipid, aqueous, mucin each have specific secreting gland with specific function Lipid layer is secreted form Meibomian glands of eyelid consist of phospholipids, glycolipids, cholesterol, esters and triglycerides, act as barrier for hydrophilic drugs. Aqueous layer secreted by Lacrimal gland (wolfing gland, Krause gland), is not completely aqueous it consists of protein, electrolyte, anti-microbials, immunoglobulin, making up to 60% of tear film, restricting lipophilic entry. Mucin layer secreted by Goblet cell of Conjunctival, mucin attached to cornea forming glycocalyx as shown in (Fig 1.4), a barrier for xenobiotics. [35,36,37,38,39] Tear film consist of both hydrophilic and lipophilic compartment thus effect the absorption and penetration of both hydrophobic and hydrophilic drug.
Conjunctiva is a thin, semi-transparent, highly vascularized, mucin secreting tissue forming the inner lining of the both the eyelids. Conjunctiva consist of the Epithelial layer and Subepithelial Stroma.[20,50] Conjunctiva is also a static barrier more permeable than cornea still effect the bioavailability of ophthalmic inserters. Barriers of Conjunctiva involve Epithelium layer, lymphatic and capillaries system, Secretory glands. Blood capillaries absorb small molecule and eliminate them in systematic circulation, it is very sensitive to irritation, lymphatic is efflux system eliminating molecules specially lipophilic component in Conjunctiva area and then ultimately in circulation. Nasolacrimal drainage of topical administrated drug in ocular results in 90% loss of instilled drug, immediately after introduction in ocular, drug is diluted with lacrimal fluid and then the diluted mixture is drained into nasolacrimal drainage
Factors of ocular environment influence the drug absorption and penetration by topical route is pH and tonicity of the ocular. pH of the ocular is around 7.4 any drug formulation with slight acidic or alkaline nature installed in ocular will result in irritation of ocular tissue and secretion of excess tear leads to tear drainage and tear dilution and if installed formulation is not isotonic with ocular tear and tissue that will results in strong physiological reflex and elimination of the dosage from ocular thus ultimately leads to poor absorption of drug.
Due to limited ani-fungal agents for ocular fungal infections available in market, thus the treatment of fungal keratitis is challenge for ophthalmologist and failure of available anti- fungal agents lead to surgery [64]. Natamycin is a polyene amphoteric macrolide antibiotic with anti-fungal properties, in 1978, approved for treatment of fungal keratitis by FDA [59,64,66,67], it is still the only approved anti-fungal for fungal keratitis, currently available as topical eyedrop. Natamycin eye drop is useful only in early stage of fungal keratitis but not effective against deeper corneal ulcers [63], activity of Natamycin against Candida species, non-filamentous fungal species which are also one of the major causative organisms for fungal keratitis, is weak to moderate[63,60], frequent topical application is required due to high molecular mass (665.75Da), poor penetration of topical natamycin in cornea and conjunctive and poor bioavailability due to precorneal barrier (Tear turnover, nasolacrimal drainage, Capillaries and lymphatic drain into blood)[21]. Due to time consuming diagnostic methods and limited treatment present for fungal keratitis makes fungal keratitis second global cause of blindness thus ,there is a serious need for more anti-fungal drugs for keratitis and improve drug delivery strategies.
Novel drug delivery system are suitable alternative of conventional ocular dosage forms[7,1]. Noble drug delivery system mainly vesicular carries are predominant in ocular drug delivery, commonly studied are liposome and niosome[70]. Main concern with lipid based vesicles system is low physicochemical stability, high scale up cost in manufacturing. In way of resolving concern of lipid based vesicle system, pro liposome, niosome and proniosome delivery system emerged as a suitable and affordable solution. Proniosome vesicle system is a new aspect to overcome physicochemical instability and manufacturing concern, however inheriting all advantages and unique properties of conventional lipid and surfactant-based vesicle system Which are controlled release.
2.1.1 UV spectroscopy
In order to ascertain the wavelength of maximum absorption (λ max) of the CTZ, 10 mg/10 ml CTZ solution in methanol was scanned using UV spectrophotometer within the wavelength range of 200–400 nm against methanol as blank. The spectrophotometric identification was carried out using Jasco UV/Visible double beam spectrometer (V-630) with 1cm matched quartz cells.
Melting point was determined by capillary method wherein the CTZ powder was placed in thin walled capillary tube. The capillary containing the sample was inserted into the melting point apparatus (Veego Instruments corporation). The temperature at which CTZ on the walls of capillary tube was observed to melt was taken as the melting point of drug.
The FTIR was performed for the structural clarification of pure drug where the presence of functional group in drug was identified. The analysis was carried out by using FTIR spectrometer, Agilent technological (Cary 630). CTZ was taken and put on the diamond crystal Knob adjusted so that it can touch the sample. Sampling range was 4000-650cm-1.
DSC measures the temperature and heat flow associated with transition in material as a function of time and temperature in controlled atmosphere. Thus through DSC we can identify whether there is any impurity or altered in API or not. Approx. 2-10 mg of drug was weighed directly in the aluminium pan and placed in the equipment under room temp. and the heating range was around 5ºC per minute in nitrogen atmosphere and then the thermogram peak was observed.
Pre-formulation studies are much important prerequisite for the formulation development. It includes physical and chemical properties of a drug molecule and along with excipients in order to develop safe, effective and stable dosage form.
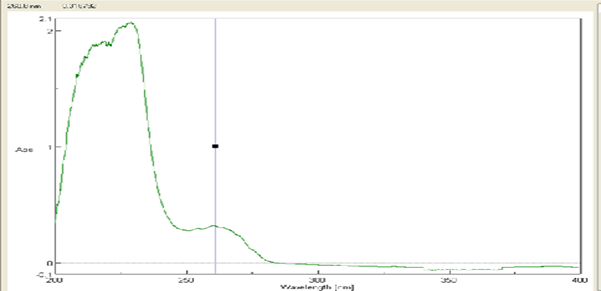
Fig 3.1: UV spectroscopy of CTZ
Melting point [130]
The melting point was ascertained using the capillary method within the melting point apparatus manufactured by the Veego Instruments Corporation, following the procedure mention in 4.2.2. Melting point of CTZ was found 142.2°C which complies with the reported literature 141-145°C. Which confirm that sample is CTZ.

Fig 3.2: Melting point of CTZ
The FTIR analysis was employed to identify CTZ and assess the purity of the sample., the spectrum was run between 400-4000 cm -1 as per BP utilizing 630 FTIR spectrophotometer Instrument Agilent Cary as shown in fig 5.3. The spectrum obtained is similar to report spectrum.
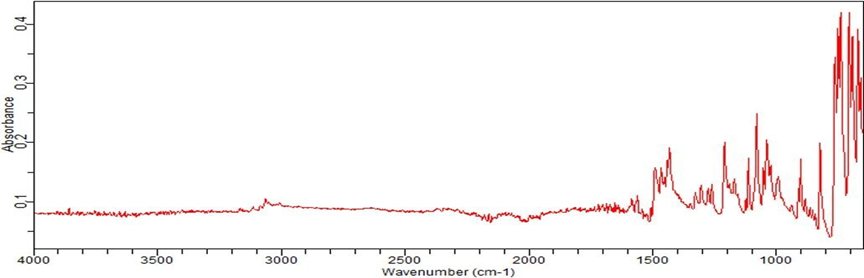
Fig 3.3: FTIR spectrum of CTZ
DSC of the pure drug CTZ was proposed and anticipated to show an endotherm peak.
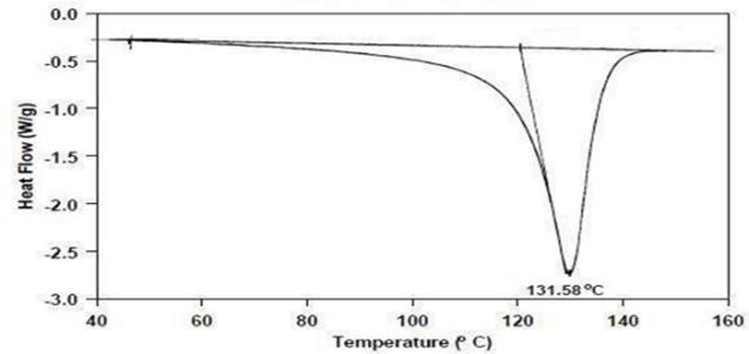
Fig 3.4: DSC Thermograms of CTZ
The solubility of the CTZ in different solvent (PB 7.4 pH, Methanol, Ethanol) is studied and the result is show in table 5.2 and fig 5.4 below. The procedure followed was mentioned in 4.3.1,
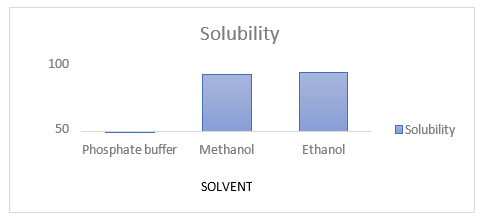
Fig 3.5: Solubility Of CTZ In Different Solvents
Table 3.1: Solubility of CTZ in different solvents
|
S. No. |
Name of solvents |
Solubility (mg/ml)±S.D (n=3) |
|
1 |
PB 7.4 pH |
0.36±0.11 |
|
2 |
Methanol |
83±0.02 |
|
3 |
Ethanol |
85±0.05 |
Partition coefficient of CTZ
The conducted study of partition coefficient found that CTZ is lipophilic in nature as shown in Table 5.3 hence have affinity for lipids.
Table 3.2: Partition coefficient of CTZ
|
Organic phase |
Aqueous phase |
Observed value (Log P) (n=3) |
Reported value (Log p) |
|
n-octanol |
Water |
5.80±0.21 |
6.30 |
Preparation of calibration curve of CTZ in methanol [62]
The calibration curve of CTZ in Methanol was prepared by using UV spectrophotometer. The concentration range of 50-300μg/ml was selected in accordance to the reported literature and the statistical parameter are summarized.
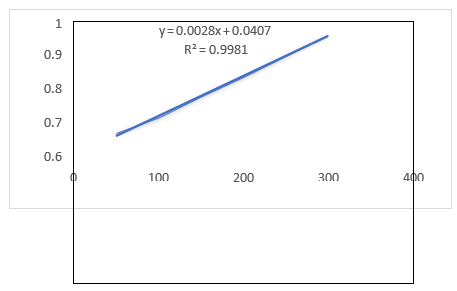
Fig 3.6: Calibration curve of CTZ in methanol
The ?max of CTZ in PB 7.4 pH was found to be 262nm. The reported ?max is 261nm. The UV spectrum of CTZ in PB pH 7.4 is shown in Fig 5.6.
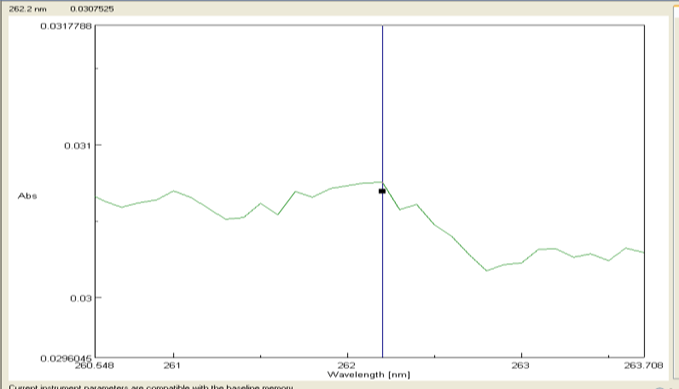
Fig 3.7: λmax of CTZ in PB 7.4 pH
The sample of known concentration of the CTZ in PB 7.4 pH is stored in various temperature for the analysis of any change during storage condition for a definite period of 2 days as shown in table 5.7 below.
Table 3.3: Intrinsic stability of CTZ
|
Solvent |
UV absorbance(abs) of sample stored at different temperature |
|||
|
25°C |
40°C |
|||
|
Phosphate buffer pH7.4 |
Initial |
After 24hr |
Initial |
After 24hr |
|
0.105 |
0.105 |
0.105 |
0.107 |
|
Selection of Surfactant is based on HLB value, transition temperature length of alky chain and gelling property as all these effect the formulated of proniosome, Span 60 have low HLB value (4.7) and high transition (53°C) remain solid at room temperature and act as gelling agent during cooling step of proniosome formulation and Tween 60 and Tween 80 trials are done for CO-surfactant and Tween 60 is selected as Tween 80 prepared formulation is yellow liquid in appearance whereas tween 60 prepared formulation is semi-solid in appearance as describe in table 5.8.
Table 3.4: Trials for selection of co-surfactant
|
Surfactant: Co-surfactant |
Appearance |
|
Span 60: Tween 60 |
Semi-solid white gel |
|
Span 60: Tween 80 |
Liquid yellow |
Preparation of CTZ proniosome
Proniosome is prepared by coacervation phase separation method. The required amount of Surfactant, CTZ and Cholesterol were added in a sterilized clear dried wide mouth glass vial of diameter 2.5 cm with high of 10 cm having a stopper, the glass vial is sterilized by Autoclave at 121 °C for 20 mins before adding of excipients. The concentration of Surfactant and Cholesterol are in table 5.10 respectively, To the glass vial containing weighted amount of (Surfactant, CTZ and Cholesterol) ethanol (0.4ml) is added in predetermined quality, after mixing of all the ingredient glass vial is closed with help of stopper. The closed glass vial is transferred to water bath heated at temperature (60 to 70°C) for 5 to 10 min with continuous stirring until lipids are completely dissolved and clear mixture is formed. To the prepared mixture warm distilled water (0.15ml) is added then again transferred to water bath at same temperature the mixture in vial is heated until clear or translucent solution in vial is produced. The mixture in vial is keep at room temperature for cooling for gelification to give proniosome with semi-solid gel like consistency. For initial trials, study nine different combination of surfactants (W/W%) decreasing concentration of span 60 against tween 60 to form stable gel.
3.8 Entrapment efficiency
Table 3.5: Entrapment efficiency of CTZ proniosome
|
S. No. |
Span60:Tween60 |
HLB |
EE% |
|
F1 |
9:1 |
5.63 |
89.95±0.3 |
|
F2 |
8:2 |
6.56 |
84.13± |
|
F3 |
7:3 |
7.49 |
80.45± |
|
F4 |
6:4 |
8.43 |
71.09± |
|
F5 |
5:5 |
9.23 |
68.56± |
In-vitro release study was proposed to be determined by membrane diffusion technique with few modifications utilizing USP Dissolution apparatus multi-tech instruments corporation and membrane proposed to be used was Cellulose membrane. (pose 12000- 15000 MWT Cut off).
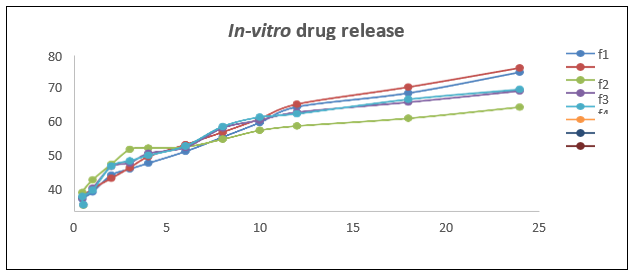
Fig 3.8: In-vitro release study of Clotrimazole in pH 7.4
Particle size and PDI of opt formulation
As per observed from result, particle size of the optimized is 188 nm with Polydispersity index (PDI) value less than (<1). Optimized formulation is nano in size thus suitable for ocular delivery as less 10µm particle size is non-irritant in ocular and nano size provide high penetration in cornea.
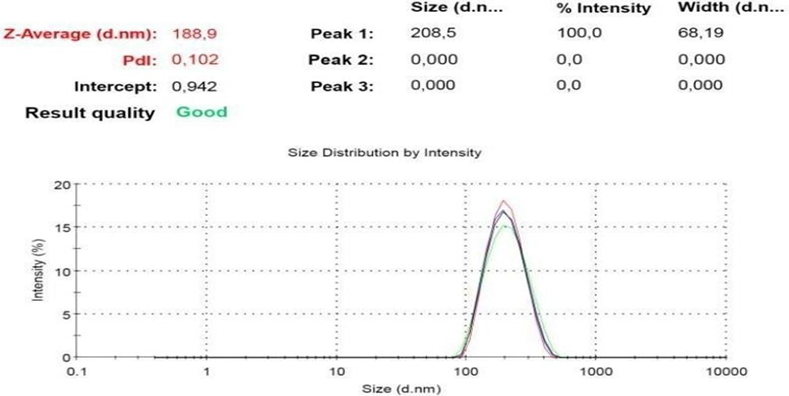
Fig 3.9: Particle Size and PDI
The electrophoretic mobility was determined by the Malvern Zetasizer 7.13. the measurement of ZP allows predictions about the storage stability of the formulation. At higher ZP, particle aggregation is less likely to occur, due to electrical repulsions. The pH of the formulation influences the ZP. In general, the Z.P was found in the range of at least ± 30 mv for sterically stabilized formulations.
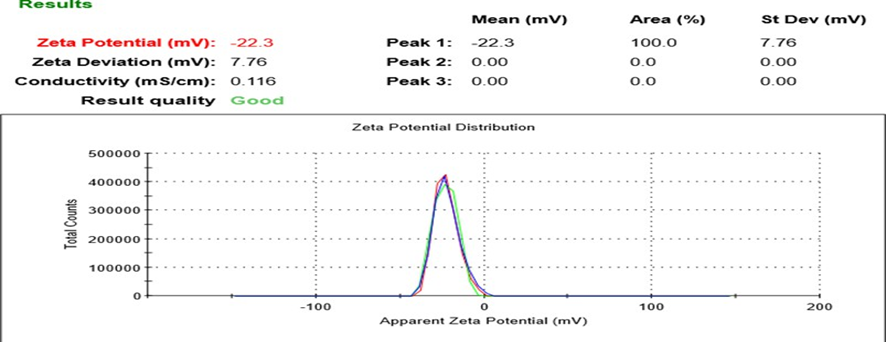
Fig 3.10: Zeta Potential
Stability study of opt formulation as per ICH guidelines
Stability study was to determine stability of opt F1 per ICH Q1A (R2) guideline at accelerated temperature. ICH Q1A guidelines for formulation supposed to be stored at normal temperature, have to undergo the stability evaluation at following temperature and for following time period.
Table 3.6: Formulation stored at normal temperature
|
Study |
Storage condition |
Period |
|
Long term |
25°C±2°C 60% RH±5% |
12 months |
|
Intermediate |
30°C±2°C 65% RH±5% |
6 months |
|
Accelerated |
40°C±2°C 75% RH±5% |
6 months |
During storage period F1 opt was evaluated for any physical change in appearance and chemical change in EE% and drug release. As per depicted form table, during storage phase, no significant change is observed in Entrapment efficiency, and release profile of selected formulation F1 at 25°C. At temperature 40°C, no significant change in slight reduction in Entrapment efficiency observed in end phase storage evaluation and slight increase in release profile at Q2 is observed. Physical appearance of F1 at 25°C and 40°C over the period of storage show no change like phase inversion, sedimentation and discoloring. Thus proniosomal gel provide more suitable and stable delivery system and diminish the stability limitation of conventional niosome hence proniosomal gel improve physical stability of niosome delivery system.
CONCLUSION
In recent decades, there has been a growing demand for more effective dosage forms that ensure high patient compliance. Current topical ocular dosage forms have not been successful in delivering an efficient dose, while injectable doses and implantation formulations are costly, require skilled personnel for drug administration, and do not promote patient compliance. A novel drug delivery system presents a suitable and effective alternative to conventional ocular delivery systems. Proniosome represents a new approach within this novel ocular delivery system, introduced as a modified type of non-ionic surfactant-based niosome to address the limitations of traditional niosomes. Proniosome can be administered to the ocular surface either in its proniosome form or can be converted to niosome immediately prior to application in the eye. The primary objective of the present study is to design and develop a system that prolongs the retention time on the ocular surface and effectively penetrates the barriers that hinder dose delivery; achieving both of these objectives will ultimately lead to enhanced ocular therapy. Additionally, the study aims to characterize and evaluate all parameters that contribute to the improvement of the active drug substance in ocular applications.
REFERENCES


Ankush Dwivedi*, Deepak Saini, Mahendra Kumar Shukla, Faisal Khan, Proniosomal Gel Based Ocular Delivery of Clotrimazole for Treatment of Fungal Keratitis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 271-285. https://doi.org/10.5281/zenodo.15789725
 10.5281/zenodo.15789725
10.5281/zenodo.15789725
