Guru Nanak Institute of Pharmaceutical Science and Technology, 157F, Panihati, Kolkata-700114.
The neurological illness called as the autism spectrum condition (ASD) may be brought on by a dysbiosis in the gut microbiota. The neurological developmental illness called as the autism spectrum condition (ASD) is highly heritable and diverse. Deficits in behaviour, communication, and socialization are its defining characteristics. Research indicates that alterations in the composition of the gut microbiota are common in individuals with ASD and affect neurodevelopment and behavior via modifications in neurotransmitter regulation, metabolite synthesis, and immunological activation. According to research, the aetiology of autism spectrum disorder (ASD) is complex and found to be multifactorial – genetic and non-genetic factors. As a consequence of these clinical studies, prebiotics, probiotics, and dietary modifications have been suggested as a therapeutic approach to treat ASD by modifying the composition of the gut microbiota. Studies are being conducted on how antibiotics affect the gut microbiome but has been impeded by the persistence of heterogeneity seen in ASD patients, variability in microbiome composition, and a lack of standardised procedures, despite the hopeful results of these therapeutic approaches. There is very little data on the long-term benefits and adverse effects of this therapeutic approach. In conclusion, even if the role of gut microbiota in ASD pathogenesis and treatment is a rapidly evolving field, substantial challenges persist alongside promising opportunities.
The condition of autism was first described in the 1940s. Both Leo Kanner and Hans Asperger began publishing on the condition almost simultaneously [1]. Autism Spectrum Disorder (ASD), also known as Autism is a neurodevelopmental disorder manifests as a highly heritable and heterogenous neurodevelopmental disorder. [2, 3] ASD is distinguished by its spectrum nature, which entails a significant degree of heterogeneity in the phenotypic manifestations observed. This heterogeneity is characterized by varying levels of intellectual and language development, as well as intra-individual differences in cognitive profiles. [4, 5] Additionally, ASD is often associated with comorbidities with other developmental disorders and psychiatric conditions. It is a behaviourally defined neurodevelopmental disorder manifested as anomalies in social communication and interaction, sensory dysfunctions, repetitive behaviours, and interests varying levels of intellectual disability. [6] Studies have shown that a combination of behavioural therapies and specific therapeutic interventions which include the administration of drugs like Aripiprazole, Escitalopram, and antidepressants, which target neurotransmitters like serotonin in the brain has been used to censure an effective relief for these conditions. It has been noted to potentially improve communication, social skills, and adaptability but it is important to note that therapeutic interventions can sometimes lead to hyperactivity, aggression and various side effects including vomiting, irritability, increase in appetite, weight gain and sedation. [7, 8] Even if researchers have been trying to develop alternative treatments for ASD by investigating the molecular mechanisms underlying the pathology of it, the aetiology still remains unknown [9, 10]. Earlier studies have reported that patients with inflammatory bowel disease (IBD) experience frequent anxiety and bouts of depression. These mental health issues may have been linked to the changes in the brain structure and function and also the changes in the composition of the gut microbiome [11]. Throughout the years, parents of individuals diagnosed with ASD have reported to have been experiencing gastrointestinal (GI) symptoms such as constipation, abdominal pain, diarrhoea and vomiting [10]. Emerging studies have shown that along with these significant conditions mentioned, individuals diagnosed with ASD present with other clinical symptoms, including gastrointestinal disturbances (up to 70%), motor deficits (79%), sleep problems (50–80%), and intellectual disability (45%). With its potential etiology not clearly identified, many studies have linked the occurrence of ASD in individuals to the alteration in their gut microbial composition [12].
The human body hosting approximately 100 trillion microbial species where most microbial species reside in the gut. The gut microbiome (GM) primarily constitutes of commensal, symbiotic and pathogenic microbial communities which plays an important role in not only the somatic development but also psychiatric developments [13]. The GM is comprised of four major (Bacteroidetes, Firmicutes, Proteobacteria, and Actinobacteria) and two minor phyla (Verrucomicrobia and Fusobacteria). It has been noted in studies that a balanced relationship between the composition of gut microbial community and the host is necessary to maintain gut homeostasis as well as the host’s health by affecting nutrient processing, availability, and absorption [14]. Communication between the central nervous system and enteric nervous system is carried out by the vagus nerve. The afferent neurons of the vagus nerve (innervating the proximal colon and intestine) are influenced by the gut microbial community. The bidirectional communication observed between the gut microbiome and the brain with multiple routes (neural, endocrine, and immune pathways) is known as the gut-microbiota-brain-axis (GUMBA). The gastrointestinal microbiota (GM) stimulates the afferent neurons of the enteric nervous system (ENS), which sends signals to the brain through the vagus nerve, innervating the proximal colon and intestine. The GM is also capable of releasing various bioactive metabolites in the gut such as neurotoxins and neurotransmitters, like acetylcholine, gamma-aminobutyric acid (GABA), adrenaline, serotonin, dopamine, or neuroactive substances such as short-chain fatty acids (SCFAs). These substances can induce changes in the central nervous system (CNS) via the endocrine pathway. Alterations in the composition of gut microbiota can lead to fluctuations in the levels of metabolites like SCFAs and lipopolysaccharides, potentially compromising gut metabolism and triggering an augmented immune response and mitochondrial dysfunction [14, 15]. The imbalance in the gut’s microbial community is known as gut dysbiosis. Studies have shown subjects with ASD showed different abundance of Clostridiaceae, Lactobacillales, Enterobacteriaceae, and Bacteroides compared to subjects without ASD. Prebiotics, herbal treatment, and Faecal Microbial Transportation (FMT) process of a healthy subject can be used to stabilize microbiome balance which gives way to a symptomatic relief to individuals with autism spectrum disorder [16]. Subsequently, the aim of this review is to utilize the present-day knowledge about gut-bacterial dysbiosis and ASD and evaluate the role of prebiotics, probiotics, diet and herbal medicines in the treatment of ASD. This review aims to (i) report emerging literature showing changes in microbiota composition and metabolite production of ASD individuals compared to healthy controls, and (ii) discuss how these changes may contribute and/or perpetuate ASD pathology.
Prevalence Of Autism Spectrum Disorder
The chances of developing autism are highly influenced by both genetic and environmental factors. According to Global Burden of Disease study (2010), globally 52 million (estimated) have autism, equating to a prevalence of 1 in 132 individuals. According to the World Health Organization (WHO), the international prevalence of autism spectrum disorder (ASD) stands at 0.76% ranging across all racial, ethnic, and socioeconomic groups; diagnosis is not uniform across these groups with Caucasian children having identified with ASD more often than Black or Hispanic children. According to the Centres for Disease Control and Prevention (CDC) report in the United States, the prevalence of ASD among 8-year-old children was 1 in 59 in 2014 (estimating about 1.68%) and 1 in 54 in 2016 (estimating slightly above average to a 2.5%). Studies claim that in Italy, the prevalence of ASD among 7–9-year-old children was 1.15% whereas in Asia, the prevalence of ASD has been reported to be 3.9%, with a prevalence of 0.14 to 2.9% in the Arab countries around the Persian Gulf [17]. According to Autism and Developmental Disabilities Monitoring Network (ADDM), the prevalence of autism spectrum disorder has doubled more in the United States with approximately 1 in 44 children diagnosed, between the years 2000 – 2002 and 2010 – 2012 though the prevalence of the ASD has significantly stabilized between the years 2014 – 2016. The report published in 2018 estimated that 1 in 59 children were diagnosed with ASD [18].
A 2014 CDC data revealed that white, non-Hispanic children were approximately 20% more likely to be identified with ASD before non-Hispanic African American children; white non-Hispanic children were about approximately 50% more likely to be identified with ASD than were Hispanic children. However, a survey of adults in the general population has shown that rates of individuals affected by autism in black and minority ethnic groups may be lower than in the rest of the population; though data obtained from indigenous and Aboriginal cultures are very limited [17].
Causes Of Asd:
While “autism” was initially introduced to describe a behavioural symptom of self-withdrawal in schizophrenic patients, it was later introduced as the umbrella term to define the heterogenous group of neurodevelopmental disorders where the symptoms manifest themselves difficulties in cognitive abilities and language levels. Syndromic ASD has multifactorial causes – non-genetic and genetic. Non-syndromic ASD has causes still relatively undetermined [19].
ASD is a highly heritable neurological disorder with a rarer de novo inherited variants in over 700 genes. Twin studies confirmed that monozygotic twins were more likely share a diagnosis than dizygotic twins, suggesting a genetic effect – it was found 60% concordance for monozygotic twins versus no concordant dizygotic twins [20, 21].
Symptoms of ASD
According to the studies conducted by Centres for Disease Control and Prevention (CDC), ASD manifests as symptoms like evading or lacking sustained eyes contact as the early signs. In the early stages, there is a noticeable lack of display of facial expressions such as happiness, sadness, anger and surprise along with absence of active participation in social interactions. In some cases, the child fails to show empathy and has a significant lack of behavioural awareness. There is a distinct observation of a child demonstrating repetitive behaviours as the signs of having Autism Spectrum Disorder. The key symptoms of ASD include impaired social behaviour and repetitive movements [22, 23].
Gut Microbiome
The human body, currently hosts trillions of microorganisms, known as microbiota on skin, in respiratory tract, digestive tract, etc. Microbiota, in general, refers to the commensal, pathogenic and symbiotic microbes found in the multicellular organism, including bacteria, Protista, fungus and viruses.

Figure 1: The key symptoms of ASD include impaired social behaviour and repetitive movements.
Gut microbiota is specifically referred to the symbiotic bacteria that is found in the gastrointestinal tract of human beings. These microorganisms include bacteria, fungi, viruses, archaea, and protozoa [24]. The human gastrointestinal tract consists of more than 1000 species of bacteria with an estimated 1011 to 1012 density of bacterial cells in the colon, making it the most densely microbial habitats. They can be termed as the metabolic machinery or sometimes referred to as the “virtual organ” because the gut microbiota can influence the physiology via neural, hormonal, and immunological pathways. The bacteria are found to be colonizing the human gut since the birth, some studies have suggested, it might even be in uterus. The gut microbiota supposedly assists with the maintenance of health but studies have they can also disrupt the homeostatic regulation and has an influence on the pathophysiology of several neurobiological disorders [25, 26].
Composition of Gut Microbiomes
The colonization of the newborn baby gut begins during birth. The gut microbiota is mainly composed of four major phyla, approximately 90% – Bacteroidetes (16.9%), Firmicutes (79.4%), Proteobacteria (1%), and Actinobacteria (2.5%) and two minor phyla - Verrucomicrobia and Fusobacteria [27]. The gut flora is mainly constituted of commensal bacteria which communicate with each other in the host-gut epithelium to maintain gut homeostasis and enhance host immunity. The composition of the gut microbiota changes with age, sex, BMI, and may also vary according to the intestine anatomical regions [28].
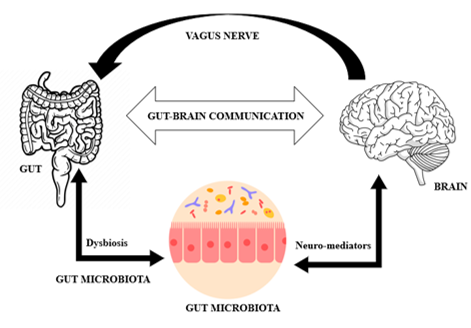
Figure 2: The gut has a bidirectional communication with the brain through the complex biochemical signalling known as gut-brain-axis (GBA)
The colonization of gut microbes starts in an infant’s gut. Within the first six months of a child’s life, bacterial groups such as Enterobacteriaceae, Bifidobacteriaceae and Clostridiaceae has been noted to show an increase in their concentration. The children who are born by Caesarean section, they are observed to show a high abundance of Bifidobacterium (Genera: Clostridium) and a low abundance of Streptococcus (Genera: Ruminococcus) [27]. The Bacteroides genus is notably not detected in the faeces until 6 – 18 months after birth. Preterm infants show low diversity with an increased colonization of potentially pathogenic bacteria from the Enterobacteriaceae family of the Proteobacteria phylum and reduced levels of strict anaerobes such as Bifidobacterium, Bacteroides, and Atopobium In a reference man (age: 70 kg), the total number of bacteria present is approximately 3.8 x 1013 cells which is comparable to the number of human host cells (3.8 x 1013). An imbalance in the composition of gut microbiome can cause disruption in homeostatic regulation and can affect the health of the host through many ways such as energy absorption, choline, short chain fatty acids, gut-brain axis and bile acids. [29]. The variations of specific microbiota at the genus and species levels depends on geographical, environmental, dietary, genotypical factors and factors related to age, diseased state, the lifestyle of an individual and antibiotics [30].
Table 1: Studies shown the major groups of gut microbiotas in children, adults and older adults are –
|
Dominant Phyla |
Children |
Adults |
Older Adults |
References |
|
Firmicutes |
+ |
+ |
+ |
[27] |
|
Bacteroidetes |
+ |
+ |
+ |
[27] |
|
Actinobacteria |
+ |
+ |
+ |
[27] |
|
Verrucomicrobia |
+ |
+ |
|
[27] |
|
Fusobacteria |
|
+ |
|
[27] |
|
Bifidobacteriaceae |
|
|
+ |
[27] |
|
Proetobacteria |
|
+ |
|
[27] |
The Gut-Brain Axis:
The gut has a bidirectional communication with the brain through the complex biochemical signalling known as gut-brain-axis (GBA). This GBA is mediated by CNS, ENS and Gastrointestinal microbiota (GM). The spinal cord, the autonomic nervous system (ANS) and the vagus nerve (VN) are connected to both gut and the brain and the communication is carried out by the VN and the ANS in the spinal cord. The ANS is constituted of three components: the sympathetic nervous system (SNS), parasympathetic nervous system (PNS) and enteric nervous system (ENS). The bidirectional communication of the GBA is carried out by the ENS of the GIT in addition to ANS and VN [30].
The VN is the tenth cranial nerve involved in the connecting neuronal pathways and transferring the signals through different pathways, including the autonomic nervous system (ANS), enteric nervous system (ENS), hypothalamic–pituitary–adrenal (HPA) axis, sympatho-adrenal axis, and descending monoaminergic pathways. The ENS is a complex network of neurons comprising of two main plexuses – the myenteric and submucosal plexus which is responsible for regulating gut functions such as motility, secretion and absorption. The communication between the ENS and CNS is done through the intestinofungal neurons and the ganglia of the SNS by relaying sensory information via primary afferent neurons following vagal afferent routes. The gut microbiota creates a direct neuronal influence via the ANS and VN. Vagal activation has been shown positive impacts on the GM [31]. The ANS which is a neural network comprising of SNS and PNS, along with neuronal and neuroendocrine signalling, regulates the gut physiology and hence, regulates body homeostasis. Any disbalance in the gut physiology or gut dysbiosis has been noted to have been the cause of intestinal disorders, including inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) and neurological and psychological disorders including, anxiety, depression, autism spectrum disorder, Alzheimer’s disease, Parkinson’s disease [31].

Figure 3: Schematic representation of the mechanism of action of gut-brain axis and subsequent effect of gut dysbiosis on behaviour and pathophysiology
GBA and GM:
Studies have shown gut-brain-axis is related to the gut microbiota and the gut microbiota has emerged as the key regulators of gut brain functioning thus leading to distinct “Microbiota-Gut-Brain Axis.” GM uses neurotransmitters such as [31] –
Gut microbiota influences the CNS via several mechanisms, such as alteration of the microbial population, stimulation of the immune system and through neural pathways and tryptophan metabolic pathways and via microbial metabolites. GM influences CNS by synthesizing or mimicking different neuroactive compounds e.g., serotonin, melatonin, histamine, GABA, acetylcholine and catecholamines. Several studies have shown that the GM influences the development, functions and disorders of the CNS and ENS via the interactions with pattern recognition receptors (PRRs) like Toll-like receptors 2 and 4 (TLR2 and TLR4). Studies have shown germ-free (GF) mouse models recognise the influence of gut microbiota on stress responses and synaptic markers related to brain development. The GF mice have shown increased blood-brain barrier permeability. Gut microbiota especially Bacteriodetes and Firmicutes is known to ferment dietary fiber to produce SCFAs such as acetate, butyrate and propionate which can increase the expression of claudin and occluding and hence resulting in the reduction of blood-brain barrier (BBB) [32]. SCFAs is essential for human well-being because SCFAs act as the primary source of energy for human colonocytes and their metabolites are blocking the activation of transcription factors in astrocytes and microglia by blocking proinflammatory factors which leads to cerebral homeostasis. Microglia are influenced by gut microbiome composition. Alteration in gut microbiota is associated with neurological disorders. Gut dysbiosis have shown to lower the numbers of myenteric neurons, bowel motor dysfunctions, dysregulated hormone signalling, reduced expression of brain-derived neurotrophic factor (BDNF) and altered neurotransmission [32].
Gut Dysbiosis And Asd:
Gut-brain crosstalk has been implicated in the development of psychological and neurological diseases. Clinical studies have shown that in transgenic animal models for Alzheimer’s disease (AD) and Parkinson’s disease (PD), gut microbiota has a significant interplay with these neurodegenerative conditions [33]. ASD patients are known to experience various other issues including gastrointestinal issues, seizures, anxiety, hyperactivity, inattentive behaviours, language disorders and delayed cognitive development or learning skills in the later stages of life. Recent studies have found a keen relationship between the gut dysbiosis and ASD. Studies conducted shows the comparison between patients suffering from only ASD versus the patients suffering from ASD along with showing symptoms of GI disorders [34, 35]. A 2016 study conducted observed that irrespective of sex and age, GI problems was noted in a high frequency in patients suffering from ASD. If the subject population is accounted to be of 100%, it was noted 8.7% of the subjects did not show GI symptoms (GI dysfunction score is 0), 35% displayed mild GI problems. Approximately, 56.3% which constituted most of the study population displayed severe GI symptoms [36, 37]. The most prevalent GI disorders included hard or voluminous stools (58.9%) and constipation (35.6%). The prevalence of GI symptoms in children and adolescents with ASD ranged between 0% and 69%, with an estimated overall prevalence of 33%. Among the subject population, 54.9% were observed to show conduct problems. Notably, within the subgroup devoid of GI disorders, conduct problems were observed in 20% of individuals. This percentage increased to 41.9% in the subgroup characterized by mild GI dysfunction, and surged to 67.9% in subjects with severe GI dysfunction [38]. When the gut microbiota of children without ASD was compared with the gut microbiota of children with ASD, it was shown that the latter was less diverse and showed lower levels of Bifidobacterium and Firmicutes and higher levels of Lactobacillus, Clostridium, Bacteriodetes, Desulfovibrio, Caloramator and Sarcina. A decrease in Bifidobacterium spp. and mucolytic bacteria Akkermansia muciniphila in the gut microbiota of autism subjects compared to subjects without ASD [37]. In subjects with ASD, gut dysbiosis disrupts the host-microbiota homeostasis which leads to various physiological disorders. This disruption can cause impairments in both gut permeability and the blood-brain barrier. The increase in the gut permeability, also known as “leaky gut”, allows proinflammatory endotoxins like lipopolysaccharide (LPS) which modulates CNS activity. In subjects with autism, there is an increased abundance of certain bacterial species like Clostridium, Bacteriodetes, Desulfovibrio, Proteobacteria and Lactobacillus while there is a decreased abundance of Bifidobacterium, Blautia, Dialister, Prevotella, Veillonella, and Turicibacter [38]. GI distress is observed in patients with ASD has been identified as a new comorbidity. ASD is associated with chronic GI symptoms such as altered bowel habits, abdominal pain and food intolerance. Studies have shown that children that the composition of microbiota in children with ASD exhibit differences in their gut and oral microbiota composition to neurotypical children. The prevalence of GI issues in children with ASD is reported to be 23 – 90%. There is an also increased risk of malignancy specially colon cancer [38]. Children with ASD children, regardless of GI issues, tend to have higher levels of Sutterella species. Moreover, children with ASD who experience functional gastrointestinal disorders have increased levels of Ruminococcus torques. Children with ASD typically show higher relative abundances of Bifidobacteraceae, Lactobacillaceae, and Veillonellaceae phyla, while healthy children usually have dominant levels of Prevotellaceae. Additionally, bacterial taxa such as Bacteroides, Coprococcus, Akkermansia, and various Ruminococcus species are more abundant and diverse in children with ASD. However, studies regarding certain bacteria like Clostridium, Sutterella, Desulfovibrio, and Lactobacillus in ASD children have been inconsistent across studies due to variations in factors like antimicrobial use, gastrointestinal symptoms, and diet [39]. Constipation is strongly correlated with specific bacterial patterns in both ASD and neurotypical individuals, with ASD children often exhibiting higher levels of Clostridium cluster XVIII and Escherichia/Shigella. Conversely, Haemophilus parainfluenzae and Faecalibacterium prausnitzii abundances are lower in ASD children, even after correcting for multiple testing. Also, there is a trend towards higher Candida levels in ASD subjects compared to neurotypical ones [40, 41].
Potential mechanisms linking gut microbiota and ASD:
Gut microbiota is non-genetic and inheritable and previously shown is influenced by various factors and it has great impact on immune, metabolic and neuronal developments and in any case of GM dysbiosis leads to neurological conditions like ASD. Gut dysbiosis means imbalance between the composition of beneficial and harmful gut microbiota and individuals suffering from ASD have noted to be suffering from gut dysbiosis [42].
The term “leaky gut” is coined to explain the potential mechanism behind the relation between gut dysbiosis and ASD. Due to leaky gut, in children suffering from autism, neurotoxic and cytotoxic molecules including opioid peptides which are produced by the pathogenic bacteria in the gut enter the systemic circulation and hence activate the immune mechanism causing tissue damage and GI inflammation. And these toxic molecules trigger the neurotransmitter function in the brain and this disruption causes abnormalities in behavioural patterns which resembles the symptoms of ASD such as decreased socialization, decreased response to pain, abnormal language and repetitive behaviours leading to confusion, delirium and even coma. Leaky gut can also be associated with the chemicals produced by yeast in case of children suffering from ASD [42, 43].
Another mechanism that has been associated with the gut dysbiosis and ASD is the genetic mutations of the CHD8 gene. The study reported that mutations in the chromodomain helicase DNA-binding protein of CHD8 gene of ASD patients are associated with transit constipation and gut motility. Another subtype of ASD, Pitt-Hopkins syndrome reports that the mutation in the transcription factor 4 gene (haploinsufficiency) causes constipation and gastroesophageal reflux. Enteric glial cells (belonging to the ENS) helps to regulate gut functions and inflammation [44, 45].
Current Treatment Approaches For Asd:
Behavioral Interventions:
Studies have shown that high-intensity applied behaviour analysis (ABA) has improved cognitive functioning and language skills in children suffering from ASD [46]. The ABA involves the use of strategies based on the principles of behaviour to improve socially behaviours by adhering to seven main dimensions:
The behavioural intervention is done over 20-40 hours per week to children. For adults, behavioural intervention includes video modelling, peer feedback, imitation and reinforcement to teach conventions of appropriate social interpersonal interaction [47].
Medication Treatment in ASD:
The significant treatment of ASD remains behavioural intervention. Yet medication treatment is done to treat the comorbidities of individuals suffering from ASD. Atypical antipsychotics such as aripiprazole, risperidone and haloperidol are used to treat the irritability, aggression and self-injurious behaviour in ASD. Stimulant medication such as methylphenidate, atomoxetine, clonidine and guanfacine are used to treat the attention-deficit/hyperactivity disorder symptoms that accompany individuals suffering from ASD. Exogenous melatonin (both immediate-release and extended-release formulations) is used for the sleep disorders to improve sleep patterns in individuals suffering from ASD. Personalized or precision medicine is the new method to approach the treatment plan of ASD. It is based on an individual’s genetic patterns [48, 49].
Gut-Microbiota based Therapies:
Since up to 70% of children with ASD have been reported to have impaired GI functions, it is concluded that a relationship between ASD and gut dysbiosis is prevalent. In a study, gut microbes were transferred from anxious mice to extroverted mice and vice versa. The results were observed after 3 weeks – the anxious mice showed tendency of being more sociable with prompt responsiveness and the extroverted mice showed more tendency of nervousness with delayed responsiveness. And with the help of the GBA hypothesis, another treatment approach of ASD adopted by clinicians was recommendation of gut microbiota eubiosis based therapies including a plant-based dietary plan, probiotics, prebiotics, FMT, MTT and treatment with antibiotics [50].
Diet Intervention:
Individuals suffering from ASD show a stringent food selection, defects in food digestion and absorption. There is a distinct lack in sufficient scientific and clinical evidence that supports the role of dietary interventions as part of ASD management. It has been noted that most autistic children are underweight due to lack of nutritional supplements. Recent studies have shown that dietary fiber significantly increases microbial diversity. Dietary interventions include of dietary fibers and ketogenic diets. Ketogenic diets are rich in fat which are a common approach to manage ASD. Gastrointestinal bacteria, such as Firmicutes, Clostridia, Bacteroides and Desulfovibrio carry out microbial fermentation of dietary fibers and produce SCFAs, butyrate, acetate and propionate. The importance of dietary fibers has been studied in several epidemiological studies – SCFA, a neuroactive compound is produced by GM, leads to alteration of metabolic and immune system function and it regulates the gene expression. SCFA, like butyrate acts like blocking enzymes called histone deacetylases (HDACs) which leads to blocking of modifications of histone proteins – leads to neurodegenerative diseases. Childrens affected by ASD are noted to produce more SCFAs because of their difference in metabolism and differences in how their bodies break down dietary fiber. Sodium butyrate is known to increase histone acetylation which promotes gene expression. However, when SCFA (propionate) is injected into the brain development has been linked to autism-like behaviours. Ketogenic diets are known to manage ASD; Omega-3 fatty acids are also known to shown beneficial for ASD. Oxidative stress has been linked to ASD and use of antioxidants like vitamins and flavonoids has been known to improve symptoms but evidence is limited. Other supplements like fermentable saccharides and polyols are noted to improve ASD symptoms yet scientific evidence is lacking [51]. ASD children have calcium deficiency which leads to gastrointestinal problems. The Feingold diet is a diet which eliminates artificial additives and observed to improve ASD symptoms yet not enough evidence exists to support this effectiveness. Studies have shown lower enzyme activity and increased levels of dietary peptides in urine, indicating poor protein digestion and leaky gut in children with ASD. The gluten-free and casein-free (GFCF) diet, constituting of intake of gluten and casein, is a common dietary intervention for ASD which results in decreasing the GI problems which associated in ASD. Studies have shown that deficiencies in Vitamin A, D, B6, B12 and folate have worsened ASD symptoms. Omega-3 and omega-6 fatty acids supplementation have shown improvements in cognitive development in children born preterm showing early signs of ASD. There are also studies shown that allergenic food has been exacerbating ASD symptoms. The oligoantigenic diet is prescribed which focuses on eliminating suspected allergenic foods [50].
Probiotics and Prebiotics:
Probiotics are living microorganisms that improve gut health by increasing the production of SCFAs and by regulating intestinal transit. Hence, they are regarded as a treatment plan of ASD. Studies have been conducted where children affected with ASD who have received probiotics for 3 months have showed increased levels of beneficial gut bacteria and improvements in the symptoms associated with ASD such as communication skills and better social skills [52, 53]. A study was conducted – a placebo controlled, double blind, crossover-designed feeding trial (12-week study duration); one group received 3 weeks of placebo followed by probiotic treatment while the other group received the same but in opposite sequence, i.e., they received the probiotic treatment first followed by the placebo. The results thus obtained showed that when supplemented with L. plantarum WCSF1, there was a significant change in the composition of microbiota – increase in the composition of beneficial bacteria like Enterococci and Lactobacilli and there is a reduction in the composition of harmful bacteria e.g., the Clostridium. These changes in the composition have resulted in improved bowel movement and stool consistency. But it was observed that other GI symptoms such as bloating, abdominal pain and flatulence were not significantly changed. When Development Behavior Checklist questionnaire assessed the behavior score of the individuals with ASD, the behavior score was significantly improved [42].
When probiotics were combined with other interventions such as oxytocin or fructo-oligosaccharides, it further improved the ASD symptoms and gut microbiome. A study where patients with ASD received either probiotics or a placebo for 28 weeks with both groups also received oxytocin at week 16. The result showed that the group receiving both oxytocin and probiotic showed reductions in autism scale scores and GI symptoms [53]. Studies showed that the effect of the combination therapy of both probiotics and prebiotics is significantly higher than only probiotics [54]. In a different approach, study focused on combining exclusion diets with prebiotics – this combination resulted in reduced GI symptoms in children with ASD. This showed a significant increase in sociable behaviour and an increase in beneficial gut microbiome [53, 55].
Faecal Microbial Transportation:
Faecal Microbial Transfer is a process which is a non-pharmacological medical therapy – faecal material from a donor is transferred into the recipient either orally or endoscopically or rectally. Studies have shown that transplantation of faecal microbiota from ASD or typically-developing donors into germ-free mice showed that colonization with gut microbiota of ASD patients was effective to induce signature ASD behaviours [56, 57]. FMT has been successful in treating various conditions like recurrent C. difficile infection, IBD and IBS by adjusting gut microbial profile and restoring the balance of anti-inflammatory bacteria [58]. This approach has shown promising result in treating ASD so FDA approval was granted for FMT therapy in ASD children in 2019. [59] In case of autism spectrum disorder, studies have found that FMT has highly impacted the composition of gut microbiota in ASD affected individuals. Studies have shown that before the process of FMT, the microbiota composition of children with ASD differs from that of children without ASD, i.e., they show higher abundance of certain bacterial taxa at both the family and genus levels compared to children without ASD. Children with ASD show higher abundance of Christensenellaceae, Akkermansiaceae in family level and Christensenellaceae R 7 group, Akkermansiaceae, Coprococcus 2, Eisenbergiella and Tyzzerella 3 in genus level; Children without ASD is noted to have more of certain bacteria like Peptostreptococcaceae in family level and Romboutsia, Fusicantenibacter, Eubacterium eligens group in genus level [60, 61]. The FMT treatment was done for 4 weeks; it was observed that the gut microbiota diversity in children suffering from ASD remains the same but the differences in the gut diversity between ASD patients and healthy subjects decreased but after 8 weeks, the differences in the gut diversity between ASD patients and healthy subjects increased and went to how they were before FMT. Then it was concluded, that FMT is a temporary therapeutical solution for ASD [62, 63]. Correlations between neurotransmitter levels and GI symptoms were found. It was found 4 weeks of FMT, serotonin (5-HT) and GABA levels were noted to decrease but the level of dopamine increased. The change in result observed after 4 weeks were noted to be more significant but then the change observed, i.e., after 8 weeks the change was not notable and it remained stable [64, 65]. Another study FMT was noted to decrease the associated gastrointestinal symptoms that accompanied the individuals suffering ASD – constipation, diarrhoea, indigestion and abdominal pain. The improvements were noted to be persisting even 8 weeks, the benefits observed to be lasting up to two years post-treatment. And the studies evaluated FMT’s effects on behavioural symptoms in the children suffering from ASD showed significant decrease in ABC and CARS scores. FMT has started to prove itself to be a novel therapy for ASD patients [66, 67].
Antibiotics:
Vancomycin and metronidazole are antibiotics that have been used to treat ASD symptoms even though the drug metronidazole is not the preferred drug [68] due to lowered plasma propionate concentrations during the same period [69]. Even if antibiotics including the likes of amoxicillin have proven to improve autistic symptoms in a child but administration of antibiotics in a prenatal stage has been noted to elevate the symptoms of the autism spectrum disorder [70]. One study [71] concluded that the use of amoxicillin has shown to improve speech, eye contact and sleep behaviours and reduced repetitive behaviours. Another study concluded that the use of Vancomycin improved communication and was effective to treat several behavioural defects [72, 73]. An open-label study with 18 children diagnosed with ASD was conducted where the treatment regimen involved antibiotics administration for two weeks followed by an extended FMT for 7-8 weeks. This study concluded that the treatment notably improved gastrointestinal disturbances like constipation, diarrhoea, abdominal pain and indigestion i.e., the GI disorders symptoms that accompany the ASD behavioural symptoms. These improvements persisted for eight weeks after the treatment was stopped [68]. Antibiotics, commonly known to be prescribed to control infections have been studied to alter the composition of gut microbiomes of pregnant women and infants when the antibiotics are administered during the prenatal or intrapartum time [74]. The studies done on rodent models have concluded that the maternal use of oral antibiotics e.g., nonabsorbable sulphonamide, neomycin, bacitracin and pimaricin during either before conception or during early gestation has shown symptoms of suffering from ASD like impaired social interactions in the infants or children [68]. Even if the cause behind the development of ASD in the infant due to maternal antibiotic use remains unclear, a subsequent link between the alteration of gut microbiome because of usage of antibiotics has been studied [74, 75].
Herbal Treatment:
Herbal treatments and herbal medications have shown an incredible potential in case of alternative treatments for ASD. The most significant herbs include Curcuma longa, Yokukansan¸ Gingko biloba, and Zingiber officinale. Recent studies have noted that Centella asiatica, Acorus calamus, Asparagus racemosus and Camellia sinensis in ASD treatment. They have studied to be effective for ASD by being anti-inflammatory, antioxidant, anti-carcinogenic and neuroprotective properties. Studies have been conducted to note the effect of vitamin D in combination of vitamin B6 and magnesium but the results were not significant. Likewise, clinical trials to study the effect of omega-3 supplementation showed minimal and variable results and no conclusion could have been drawn to show that these medications are an effective alternative to traditional pharmaceutical treatments used to improve the symptoms of ASD [76].
Challenges In Incorporating Gut Microbiota Based Therapy In Asd Treatment
Microbiota-based treatments have shown promising future in improving the treatment procedure of ASD because this type of treatment is simpler and more cost-effective because effecting the composition of the gut microbiota is easier than developing new drugs or gene therapy. The usage of conventional prebiotics, probiotics and herbal medications as food supplements to cause gut eubiosis i.e., restore the gut microbiota homeostasis is an easier and simpler method. But there are certain challenges pertaining to the dietary intervention methods and prescription of probiotics and prebiotics. Dietary intervention including exclusion diets have been noted to lead to high amino acid excretion and nutrient malabsorption. There have been adverse events linked to FMT that have been noted [77, 78]. The adverse events studied are both short term (within 48 hours) and long term (3 months after FMT). The short-term effect is noted as 60% experience diarrhoea lasting less than a week, abdominal pain, fever and vomiting whereas the long-term adverse events have been rare with only one case of death due to sepsis and liver failure in a child who had primary immunodeficiency. To design a treatment of ASD pertaining to restore the gut microbiota homeostasis, further research is important to study the mechanisms through which dietary interventions, prescription of probiotics and prebiotics impact mental health. It is essential to consider other lifestyle modifications which proves to be challenging to develop a novel therapy to treat ASD.
Future Aspects
Alleviating ASD symptoms by modifying the gut microbiota through dietary interventions is easier but every currently data related to preclinical studies needs to be validated and transformed to clinical studies. Microbiota-based therapies have offered significant effect in managing ASD through an easier and cost-effective approach. Further studies have noted that enhancing this approach by identifying and selecting specific microbes or creating genetically modified microbes for inclusion in next-generation probiotic supplements to optimize treatment outcomes [77, 79]. Modifying microbes with desirable properties is now an easier approach because synthesizing new organism with a few hundred genes is now achievable. Studies including B. fragilis has been noted to improve ASD-like symptoms in animals which further proved the effectivity of the approach of treating ASD by restoring gut-microbiome composition. Recent studies have shown that rehabilitation of a healthy microbiome including bacteria like F. prausnitzii and B. thetaiotaomicron can be done by adding sialylated milk oligosaccharides to the diet or including new fermentable fibers and dietary nutrients. FMT has been mainly being done particularly for the treatment of recurrent antibiotic-resistant Clostridium difficile infection. This is an engineered bacteria which has been noted to sense local environmental changes and trigger appropriate response to correct the dysbiosis.
CONCLUSION
The concept of how alterations in gut microbiota composition, its significant influence upon the neurodevelopmental diseases has been delved into. To design a treatment of ASD pertaining to homeostasis, more important for noting the mechanisms through which dietary interventions, prescription of probiotics and prebiotics impact mental health. It is essential to consider other lifestyle modifications which proves to be challenging to develop a novel therapy to treat ASD. Also, we have understood the prospect of different treatments of modifying the gut microbiota by dietary interventions, prescription of probiotics and prebiotics, antibiotics, herbal medicines and methods such as FMT and MTT which have been deemed to have the potential in improving the symptoms of ASD. The challenges and future opportunities that entailed such methods of treatments are identified in this thesis.
List Of Abbreviations
|
ASD |
Autism Spectrum Disorder |
|
PDD |
Pervasive Developmental Disorders |
|
DSM-5 |
Diagnostic and Statistical Manual of Mental Disorders, 5th edition |
|
ADDM |
Autism and Developmental Disabilities Monitoring |
|
CDC |
Centers for Disease Control and Prevention |
|
SSRIs |
Selective serotonin reuptake inhibitors |
|
IBD |
Inflammatory Bowel Disease |
|
GI |
Gastro-Intestinal |
|
GM |
Gut Microbiota |
|
GUMBA |
Gut-Microbiota-Brain-Axis |
|
GABA |
?-aminobutyric acid |
|
SCFAs |
Short Chain Fatty Acids |
|
CNS |
Central Nervous System |
|
FMT |
Faecal Microbial Transportation |
|
MTT |
Microbiota Transfer Therapy |
|
VN |
Vagal Nerve |
|
ANS |
Autonomic Nervous System |
|
HPA |
Hypothalamic–Pituitary–Adrenal |
|
ENS |
Enteric Nervous Nervous |
|
TLR2 |
Toll-like receptors 2 |
|
TLR4 |
Toll-like receptors 4 |
|
BBB |
Blood-Brain-Barrier |
|
BDNF |
Brain-Derived Neurotrophic Factor |
|
AD |
Alzheimer’s Disease |
|
PD |
Parkinson’s Disease |
|
IBS |
Irritable Bowel Syndrome |
|
MS |
Multiple Sclerosis |
|
CHD8 |
Chromodomain Helicase DNA-Binding Protein |
|
ABA |
Applied Behavior Analysis |
|
GBA |
Gut-Brain-Axis |
|
HDACs |
Histone Deacetylases |
|
GFCF |
Gluten-Free and Casein-Free |
ACKNOWLEDGEMENTS:
I, Suchandra Chatterjee, take this privilege to extend my sincere gratitude to my mentor, Dr. Sanchari Bhattacharya (Assistant Professor, GNIPST) for her invaluable insight and support throughout this project and who helped me with every step of this review project. I am also very grateful to all the faculty members, along with our Director Sir, Prof. (Dr.) Abhijit Sengupta (Director, GNIPST) and Prof. (Dr.) Lopamudra Datta (Principal, GNIPST) of Guru Nanak Institute of Pharmaceutical Science and Technology for providing me with such a platform to work hard and put up such work. I am indebted to my family members and all the well-wisher’s offering motivation and supported me with every step of this project.
REFERENCES



Suchandra Chatterjee, Sanchari Bhattacharya*, Debjeet Sur, Recent Advancements in the Treatment of Autism Spectrum Disorder Through Gut Microbiota: A Comprehensive Review, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 865-883. https://doi.org/ 10.5281/zenodo.14311293
 10.5281/zenodo.14311293
10.5281/zenodo.14311293
