
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Amity University, Lucknow Campus,
2 Sakshi College of Pharmacy Kanpur,
3 Maharishi University Lucknow,
4 Rapti Academy of Health Sciences Nepal,
5,6,7,8,9 KIPM Technical Campus Gorakhpur,
10 Swami Vivekanand Subharti University, Meerut
Cardiovascular disorders continue to be a leading cause of morbidity and mortality worldwide, necessitating ongoing research for novel therapeutic interventions. Reserpine, an indole alkaloid derived from the Indian snakeroot plant (Rauvolfia serpentina), has garnered significant interest as a potential candidate for managing cardiovascular conditions. Reserpine's primary mechanism of action involves inhibiting the vesicular uptake of neurotransmitters, leading to a reduction in sympathetic nervous system activity. This results in vasodilation and decreased cardiac output, making it a valuable option for hypertension management. Several clinical studies have demonstrated its efficacy in lowering blood pressure and improving overall cardiovascular health. Furthermore, reserpine exhibits antiarrhythmic properties by stabilizing electrical activity in the heart, which may be beneficial in arrhythmia management. Hence, reserpine presents a promising avenue for the management of cardiovascular disorders, particularly in cases of hypertension and arrhythmias. Its unique mechanism of action makes it an attractive option, albeit with some associated risks. Therefore this comprehensive review examines the potential of reserpine in the context of cardiovascular disorders, encompassing its pharmacological properties, mechanisms of action, and clinical applications.
Hypertension, or high blood pressure, stands as the leading cardiovascular risk factor for mortality globally, including in high-income regions. Epidemiological data from around the world indicate that approximately 40-45% of the population has hypertension.(1) However, awareness of this condition is only around 50%, and merely 45-50% of those diagnosed receive treatment with antihypertensive drugs. Unfortunately, treatment control is less than satisfactory, with less than 20% of patients worldwide and almost 40% in Europe achieving proper control of their blood pressure.(2,3)
Observational evidence from various studies suggests that reducing mortality in individuals with hypertension is closely tied to achieving and maintaining target blood pressure levels rather than simply undergoing treatment without achieving adequate control. Research from randomized controlled trials specifically related to hypertension also supports the idea that lowering blood pressure below the traditional threshold of 140/90 mmHg for systolic and diastolic blood pressure, respectively, leads to greater cardiovascular benefits and reduced mortality compared to lowering blood pressure above this threshold.(4-6)
Reserpine is a medication primarily used to treat high blood pressure, often in combination with a thiazide diuretic or vasodilator. Extensive clinical trials have shown that using reserpine alongside a thiazide diuretic can reduce mortality in people with hypertension. While the use of reserpine as a standalone drug has declined since its FDA approval in 1955, it is still recommended to combine reserpine with a thiazide diuretic or vasodilator when initial drug treatment alone doesn't sufficiently lower blood pressure. In 2012, the combination pill of reserpine and hydrochlorothiazide was the 17th most commonly prescribed among the 43 available combination antihypertensive pills.(7)
Reserpine's antihypertensive effects primarily result from its antinoradrenergic actions, which are due to its ability to deplete catecholamines and other monoamine neurotransmitters from peripheral sympathetic nerve endings. These substances typically control heart rate, the strength of cardiac contractions, and peripheral vascular resistance.(8) Hence, in this article we will discuss about the reserpine source, its pharmacological properties along with its mechanism and clinical applications.
Plant Source
Reserpine is an indole alkaloid derived from the roots of Rauwolfia serpentina, a climbing shrub native to India. Rauwolfia serpentina, scientifically known as Rauwolfia serpentina (Linne) Bentham ex Kurz, belongs to the Apocynaceae family. It is an upright shrub, typically reaching a height of one meter, with cylindrical stems. These stems have pale bark and contain a light-colored, viscous latex.(9)
The leaves of Rauwolfia serpentina can be either simple and opposite or more commonly arranged in whorls of 3 to 5. The plant produces white or pale rose-colored flowers that are arranged in terminal and axillary cymes. Its fruit is a single, two-lobed drupe that turns purplish-black when it matures.Reserpine was first isolated in 1952 by Muller Schiltter and Bein. Its chemical formula is C33H40O9N2.(10)
History
Rauwolfia serpentina has a historical presence in Ayurvedic medicine, where it is known as "Sarpgandha" and "Chandra." "Sarpgandha" translates to "snake smell" or "repellent," suggesting its use as an antidote for snakebites. In the early 20th century, Sen and Bose, in 1931, reported the valuable and safe use of Rauwolfia serpentina in treating high blood pressure, noting that it achieved precision in blood pressure control unmatched by other drugs, whether Eastern or Western in origin.(11)
Further, in 1949, Vakil conducted extensive trials of various hypotensive remedies for hypertension over ten years, involving several thousand cases in both private and hospital settings. His findings revealed that Rauwolfia serpentina was the most effective drug in reducing both systolic and diastolic blood pressure. Importantly, it exhibited low toxicity, with only mild adverse effects. In a questionnaire distributed to 50 physicians across India, 46 of them voted in favor of Rauwolfia serpentina as the best antihypertensive agent based on their experiences. This solidified its place in medicine as a potent treatment for high blood pressure.(12)
Structure of Reserpine
The enzyme strictosidine synthase (STR1), found in the Indian medicinal plant Rauwolfia serpentina, plays a crucial role in the biosynthesis of the majority of indole alkaloids, including Reserpine. The biosynthesis of Reserpine involves several steps, as depicted in Figure 1.
1. The process begins with tryptamine and the monoterpenoid Secologanine, which combine to produce the glucoalkaloid Strictosidine in the initial step of biosynthesis.
2. The enzyme Strictosidine synthase (STR1) then plays a key role in the subsequent biosynthesis of Reserpine, facilitating the transformation of Strictosidine into Reserpine.(13,14)
This enzymatic process ultimately leads to the production of Reserpine, a valuable alkaloid with medicinal properties, within the Rauwolfia serpentina plant.
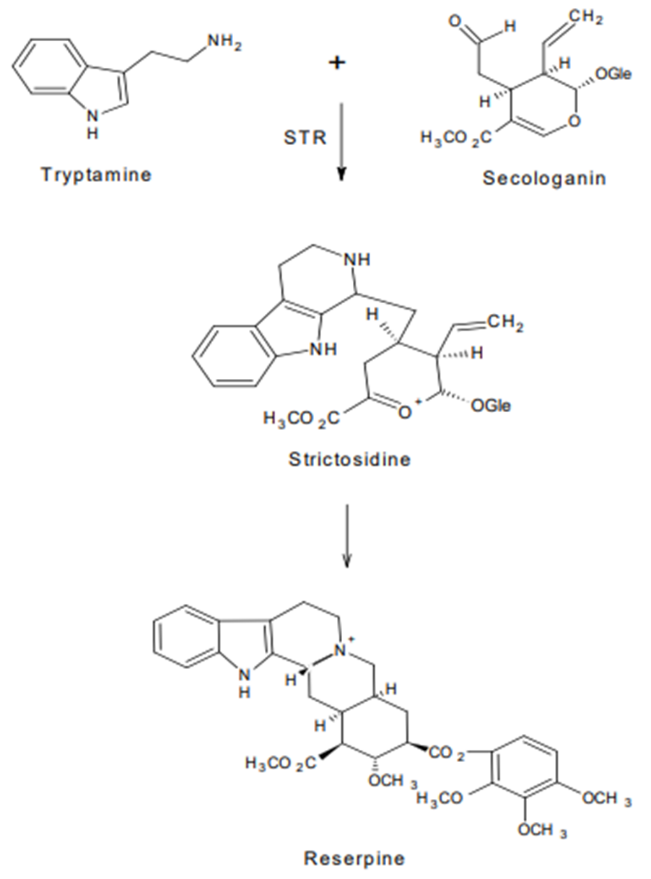
Fig 1:- Biosynthesis of reserpine.
Mechanism of action
Chopra, Gupta, and Mukherjee conducted studies indicating that alkaloids, particularly Reserpine, had a significant hypotensive effect. This effect was attributed to the depression of central nervous system mechanisms. Additionally, Reserpine exhibited an inhibitory effect on the musculature of blood vessels, and they observed a decrease in the output of the isolated heart.(15)
Reserpine was found to reduce reflex vasomotor responses, suggesting its influence on the peripheral vessels independent of its nervous activity. This effect was observed in rabbits using a method developed by Gallagher, involving the perfusion of the isolated hind limb with a blood-Dextran medium at a constant rate. Changes in vasomotor tone were indicated by alterations in perfusion pressure. Interestingly, the injection of Reserpine into the systemic circulation of rabbits resulted in an immediate drop in systemic blood pressure, accompanied by an immediate increase in limb perfusion pressure instead of the anticipated decrease, which was expected to be mediated through the nervous system. Moreover, injecting Reserpine directly into the artery of the perfused hind limb caused an immediate decrease in vasomotor tone.(16,17)
Chopra, Gupta, and Mukherjee noted that a notable feature of all these reactions was their remarkably prolonged duration, suggesting that the drug binds to the musculature. They also gathered evidence indicating that this direct peripheral effect might play a role in Reserpine's hypotensive action in humans.(18)
Furthermore, McQueen, Doyle, and Smirke reported that a direct peripheral effect could be involved in Reserpine's hypotensive action in humans, corroborating the findings of Chopra, Gupta, and Mukherjee.(19)
Preparation and Dosage
In cases of severe hypertension, Reserpine may be administered via intravenous or intramuscular injection, and its effects typically begin to manifest within a few hours. Parenteral therapy with Reserpine is recommended for hypertension treatment when oral administration is not feasible.
Powdered Rauwolfia refers to the finely powdered root of Rauwolfia serpentina, which meets the official requirements for Reserpine-rescinnamine group alkaloids. It should contain no less than 0.15% and no more than 0.20% of the Reserpine-rescinnamine group alkaloid, with calculations based on Reserpine content.(20,21)
As for dosage, the usual initial dose of Reserpine is 500 mg once a day for 1-2 weeks, followed by a maintenance dose of 100 to 250 mg once a day. Patients taking Reserpine should be advised to notify their physician if they experience any changes in mood.(22)
For condition like Refractory Hypertension
Refractory hypertension is a challenging clinical condition where all available medications and doses fail to effectively control blood pressure. It's distinct from resistant hypertension, which is characterized by blood pressure that remains inadequately controlled despite treatment with three or more appropriately dosed medications. Resistant hypertension also includes individuals who require four or more appropriately dosed medications for blood pressure control.(23-25)
Research indicates that while refractory hypertension is relatively rare, it presents a significant challenge for clinicians who aim to achieve better blood pressure control and prevent cardiovascular events.(26) Unfortunately, there have been limited developments in new drugs to manage both resistant and refractory hypertension, despite the introduction of medications like endothelin receptor antagonists, neutral endopeptidase-angiotensin-converting enzyme (ACE) inhibitors, and renal denervation. Some experts propose that resistant hypertension may be linked to volume excess, while refractory hypertension could result from inadequately controlled activity of the sympathetic nervous system.(27-30)
A study by Siddiqui et al. offers intriguing insights into the treatment of refractory hypertension. The researchers repurposed an old drug, reserpine, which was once used in combination with thiazide diuretics or vasodilators to treat hypertension. Reserpine depletes catecholamines from peripheral sympathetic nerve endings, affecting heart rate, myocardial function, and peripheral vascular resistance. Although its use has declined over the years with the introduction of newer antihypertensive drugs, reserpine's mechanism of action remains relevant to hypertension treatment.(31-33)
The study explored the potential of low-dose reserpine (0.1 mg daily) in six patients with refractory hypertension. The trial was carefully designed, excluding other sympatholytic medications before starting reserpine treatment. Chlorthalidone and a mineralocorticoid receptor antagonist were included as part of the multidrug regimen. The results were promising, with significant reductions in systolic and diastolic blood pressure observed in office and ambulatory settings.(34)
The study opens doors to reconsidering the use of older medications like reserpine, especially when addressing refractory hypertension. Further research and dose optimization could reveal its full potential in controlling blood pressure, offering a cost-effective and accessible option for patients facing this challenging condition.(35-37)
The study's findings raise a pertinent question: Why hasn't reserpine been considered earlier as a treatment for patients with suspected hyperadrenergic hypertension? While thiazide diuretics and mineralocorticoid receptor blockade have shown their importance in managing blood pressure in various patient groups, especially those with chronic kidney disease and resistant hypertension, there has been limited exploration of the role of the sympathetic nervous system, except for renal denervation studies.(38,39) Yet, the study's results highlight the potential significance of addressing sympathetic nervous system activity, particularly in patients with increased heart rate and refractory hypertension that has been largely unresponsive to beta-blockers.(40,41)
In summary, this proof-of-concept study makes a valuable contribution to the literature on refractory hypertension. The enrolled patients were well-phenotyped, confirming their refractory hypertension status through automated office readings, ambulatory blood pressure monitoring, and medication serum measurements to assess compliance. The results are indeed remarkable and should prompt further investigation of reserpine in larger clinical trials involving patients with both refractory and resistant hypertension. Additionally, this study could potentially incentivize pharmaceutical companies to produce reserpine in pill form again, making it more accessible to clinicians. Importantly, the 0.1 mg dose of reserpine was well-tolerated in this small clinical trial, which aligns with earlier trials' experiences where reserpine was part of a multi-drug regimen.(42)
Siddiqui and colleagues deserve commendation for their significant contribution to the literature, shedding new light on the pathogenesis of refractory hypertension and offering insights into future treatment approaches for this complex clinical condition.(43)
CONCLUSION
In conclusion, reserpine represents a noteworthy candidate in the armamentarium against cardiovascular disorders. Its ability to modulate sympathetic nervous system activity, resulting in vasodilation and reduced cardiac output, makes it a compelling option for managing hypertension, one of the most prevalent risk factors for cardiovascular events. Additionally, its antiarrhythmic properties offer potential benefits in the treatment of cardiac arrhythmias.
Nevertheless, it is imperative to acknowledge the caveats associated with reserpine therapy. Adverse effects, including depression, sedation, and gastrointestinal disturbances, as well as the potential for neuropsychiatric side effects upon long-term use, underscore the importance of careful patient selection and close monitoring. Clinicians should weigh the potential benefits of reserpine against its risks on a case-by-case basis. Future research endeavors should aim to refine our understanding of reserpine's mechanisms of action, optimal dosing regimens, and long-term safety profiles. Comparative studies against existing cardiovascular medications would also be valuable in establishing its place in contemporary treatment strategies.
In a field where cardiovascular disorders continue to exert a substantial toll on global health, reserpine's unique pharmacological properties offer promise for patients who may not respond optimally to current therapies. While it may not be a first-line option for all individuals, reserpine has the potential to carve out a valuable niche in the multifaceted landscape of cardiovascular care, providing an additional tool to combat these life-threatening conditions. Further research and clinical experience will be instrumental in realizing the full potential of reserpine as a therapeutic agent in the fight against cardiovascular disorders.
REFERENCES

Dr. Neeraj Jain, Dr. Neelam Jain, Pragati Mishra, Suraj Neupane, Devendra, Utkarsh Tiwari, Amrit Jaiswal, Abhishek Yadav, Richa Mishra, Ankita Tripathi, Reserpine as a Potential Therapeutic Agent for Cardiovascular Disorders: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3106-3114. https://doi.org/10.5281/zenodo.19217139
 10.5281/zenodo.19217139
10.5281/zenodo.19217139