Dr. K. V. Subba Reddy Institute of Pharmacy, Dupadu, Kurnool, Andhra Pradesh 518218
This review article highlights Health-Related Quality of Life (HRQoL) as an essential multidimensional metric in healthcare, capturing physical, psychological, and social well-being. It explores the dynamic and individualized facets of HRQoL in chronic disease contexts, emphasizing notable gender disparities. The paper reviews economic evaluation approaches such as QALY estimation and assesses the selection, development, and psychometric validation of HRQoL instruments. Challenges—including proxy response use, scoring interpretation, and instrument adaptation—are discussed, alongside the necessity for robust methods to ensure valid, patient-centered outcomes in both clinical practice and research. The article underscores HRQoL’s rising value in health policy, intervention evaluation, and decision-making, reinforcing its critical role in optimizing patient care and guiding resource allocation.
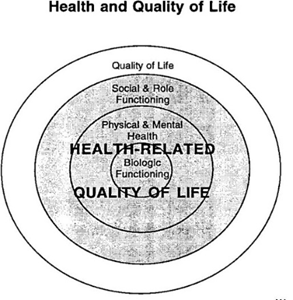
1.1 Definition [1]
Health-related quality of life (HRQoL) refers to a person’s well-being as it relates to their health conditions or diseases, and has become a focus for policymakers, researchers, and healthcare professionals. It is particularly vital that HRQoL research addresses the values and needs of both patients and their families. Due to its complex, multidimensional nature. HRQoL has been challenging to define, and literature suggests at least four distinct definitions. One widely used definition describes HRQoL as the degree to which an individual is capable to function in daily life and their personal sense of well-being across holistic well-being. Here, “functioning” indicates the ability to perform certain predetermined activities, while “well-being” captures the individual’s own subjective feelings
1.2 Significance of HRQOL[2]
Measuring Health-Related Quality of Life (HRQoL) plays an important role in healthcare services and intervention programs.
According to Revicki (1989), the medical focus has shifted from mainly addressing infectious diseases to emphasizing chronic diseases, where the study of quality of life and changes in functioning related to disease become central.
2.Approaches of health-related quality of life (HRQoL)[3]
can be approached in two main ways
2.1 Population centralized HRQOL
Population-level health-related quality of life (HRQoL) measures assess the overall well-being of communities or entire nations. The CDC uses tools such as the “Healthy Days Measures” survey to collect information on residents’ health and quality of life. These assessments are designed to spot health inequities, track changes over time, and strengthen public health initiatives, reflecting the WHO’s wider view of health as more than just the absence of illness.
2.2 Individual centralized HRQOL
A population-based approach to evaluate health-related quality of life (HRQoL) may overlook individual differences. An individual-focused method recognizes that personal experiences shape beliefs about illness, influencing coping strategies and outcomes. Debate exists regarding whether these beliefs directly impact quality of life or if they do so indirectly through coping mechanisms. Measuring HRQoL individually enhances diagnosis, outcome prediction, treatment evaluation, and understanding illness causes.
3. Nature Of HRQOL: Stable or Dynamic
The nature of Health-Related Quality of Life (HRQoL) for subjects with severe or life-threatening diseases is dynamic, changing over time as patients navigate different illness stages. Their emotional responses, needs, and perceptions shift, often referred to as "response shift," where individuals adjust their standards for wellbeing. For example, cancer patients experiencing fatigue may come to accept it as "normal" or find it discouraging based on their mental preparedness. Social comparisons also affect HRQoL, with individuals assessing themselves against others, engaging in upward, lateral, or downward comparisons to bolster self-esteem or motivate improvement. However, excessive downward comparison can harm identity and motivation. Understanding the evolving subjective perspective of HRQoL emphasizes the need for individualized chronic disease care.
4. Variations in Perceived HRQoL Across Genders
Gender differences in health-related quality of life (HRQoL) have been consistently observed across chronic diseases, with women generally reporting poorer outcomes than men. Studies show that women with conditions such as chronic heart failure and cystic fibrosis experience more emotional distress and lower physical activity levels. Adolescent females with cystic fibrosis report worse mental health compared to males, while women with heart disease often
more heavily on social support, which affects their HRQoL. Physiological factors, including co-morbidities and disease onset age, contribute to this disparity. Women tend to have multiple health conditions and experience illnesses differently than men. Psychosocial factors, such as social support and emotional needs, also play significant roles in shaping HRQoL
Understanding these differences is crucial for creating targeted health interventions to enhance HRQoL for both genders.
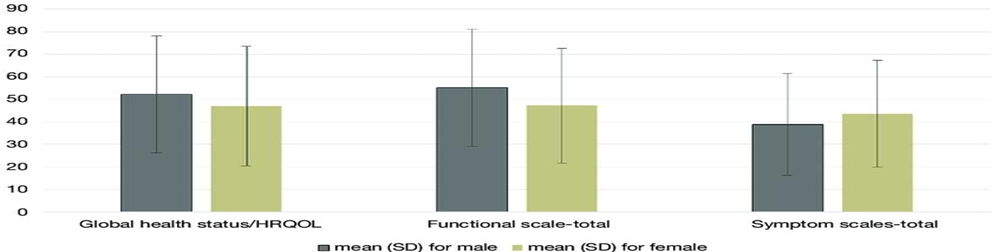
Graphical Representation of Gender Difference in HRQOL
5. Methods Of Economic Evaluation [4]
Health-related quality of life (HRQoL) plays a key role in assessing medical interventions, which are typically evaluated through three approaches: cost-benefit analysis (CBA), cost-effectiveness analysis (CEA), and cost-utility analysis (CUA). CBA measures both costs and benefits in monetary terms but generally does not account for HRQoL. CEA compares costs with health outcomes, though it lacks a universal metric, making comparisons across different programs challenging. In contrast, CUA uses quality-adjusted life years (QALYs) to combine both life expectancy and quality of life into a standardized measure, enabling meaningful comparisons between interventions. In this way, HRQoL data strengthens economic evaluations and guides the prioritization of healthcare decisions.
5.1 Measuring Outcomes for Economic Analysis:
In cost-utility analysis (CUA), utility weighting assigns values to health states from death to optimal functioning, emphasizing the impact of health conditions on quality of life (QoL) rather than just survival. Conditions like arthritis and depression can significantly lower health-related quality of life (HRQoL) without affecting life expectancy, an effect often overlooked by traditional survival analysis. A holistic evaluation of health outcomes should consider both benefits and side effects of treatments, focusing on patients' overall well-being and not merely on lifespan. This comprehensive approach ultimately enhances economic evaluations by merging quantity and quality of life measures.
5.2 Early HRQoL Instruments for QALY Estimation
First-generation measures for calculating Quality-Adjusted Life Years (QALYs) involve categorizing patients by their functioning levels and well-being, assessing health states on a preference scale from 0.0 (death) to 1.0 (perfect health), and recording the duration spent in each state. This approach helps accurately estimate QALYs by reflecting both the quality and length of life in various health states.
5.3 Uses of HRQOL Measures
Federal agencies, especially the Department of Health and Human Services, use HRQoL (Health-Related Quality of Life) measures to track the health of populations. These instruments are vital for evaluating overall health status, detecting trends, and guiding public health priorities by drawing on individuals’ self-reports of physical and mental well-being.
5.4 The Centers for Disease Control and Prevention [5]
In the United States, health-related quality of life (HRQoL) is frequently measured with the question, “In general, how would you rate your health?” This item appears in major national surveys such as the National Health Interview Survey (NHIS) and the Behavioral Risk Factor Surveillance System (BRFSS). The NHIS further incorporates elements from the Patient-Reported Outcomes Measurement Information System (PROMIS). While these surveys typically produce comparable health scores, responses from the NHIS are often more favorable, likely because the survey is administered by interviewers. In addition, the Medicare Health Outcomes Survey (MHOS) gathers HRQoL information from around 1,000 Medicare beneficiaries each year, supporting federal efforts to track and improve population health.
5.5 Economic Evaluation in Clinical Trials [6]
Growing attention is being given to assessing the cost utility of treatments within randomized clinical trials; however, health-related quality of life (HRQoL) is frequently not measured directly, which can introduce bias into the results. To improve accuracy, HRQoL utility measures should ideally be incorporated prospectively. Only a few large trials, including the National Emphysema Treatment Trial, the Diabetes Prevention Program, and the Look AHEAD Trial, were specifically designed to capture these measures from the outset. Integrating HRQoL assessments enhances the comprehensiveness of evaluations by considering both clinical outcomes and patients’ perspectives on quality of life, which is vital for healthcare decision-making and reimbursement.
5.6 Use and effectiveness of HRQOL measures.
Research suggests that health-related quality of life (HRQoL) measures enhance communication between healthcare providers and patients, aiding shared decision-making. However, evidence on their effect on patient HRQoL changes is inconsistent. Institutions like the University of Utah and Stanford have integrated PROMIS measures into routine care. While experts believe HRQoL measures can elevate healthcare quality, challenges remain in proving direct HRQoL improvements. Their growing use indicates an increasing emphasis on patient perspectives in evaluating treatment and care quality.
6. General Overview of Study Design[7]
Measures of health-related quality of life (HRQoL), which reflect patient-reported outcomes, are increasingly utilized in clinical trials and comparative research. These measures capture patients' views on health, including symptoms and satisfaction with care, and inform clinical decision-making by highlighting treatment effects that clinician-reported measures might overlook. The significance of HRQoL is acknowledged by organizations like the American Heart Association and the U.S. Food and Drug Administration, promoting their use in clinical care and research. Valid conclusions from HRQoL data necessitate robust measurement tools and understanding psychometric methods for analysis. This article reviews these strategies and offers a guide for authors and reviewers involved in HRQoL data assessment.
6.1 Use Cases of Study Design[8]
Studies indicate that using health-related quality of life (HRQoL) measures can improve dialogue between patients and healthcare providers, supporting shared decision-making. Yet, the evidence regarding their impact on actual improvements in patient HRQoL remains mixed. Institutions such as the University of Utah and Stanford have adopted PROMIS measures as part of routine clinical practice. Although many experts argue that HRQoL measures have the potential to enhance overall care quality, demonstrating clear improvements in HRQoL remains a challenge. Their expanding use highlights the growing importance of incorporating patient perspectives when assessing treatment and healthcare quality.
6.2 Health Utility Measures [9]
Health utility measures capture patient preferences for different health states and act as generic indicators of health-related quality of life (HRQoL). They can be gathered directly through approaches such as the standard gamble, time trade-off, or willingness-to-pay methods, or indirectly through HRQoL questionnaires that incorporate population-based preference weights. Utility values typically range from 0 (representing death or states worse than death) to 1 (indicating perfect health) and are used to calculate quality-adjusted life years (QALYs). As a central tool in cost-effectiveness analysis, QALYs provide a standardized way to assess health outcomes and support healthcare resource allocation by expressing the value of health states in terms of both longevity and quality of life.
6.3 Interpretability of HRQOL Measures
Health-related quality of life (HRQoL) scores can be difficult to interpret due to unfamiliar scales. To enhance understanding, these scores are compared to reference populations, such as the PROMIS Global Health scores, which have a mean of 50 and a standard deviation of 10. A score of 40 indicates worse HRQoL than about 84% of the population. Minimal important difference (MID) thresholds, representing meaningful changes in scores, vary by context but are often estimated as half a standard deviation. For PROMIS, an MID of 5 points signifies clinically significant changes at both individual and group levels, aiding in clinical trial sample size estimation and differentiating statistical from clinical significance.
6.4 Proxy Reporting in HRQoL Measures
A significant challenge in HRQoL measurements is the exclusion of patients with cognitive, linguistic, or motor impairments, which causes selection bias. Proxy respondents, usually caregivers, are used to complete HRQoL surveys instead. However, many HRQoL instruments lack validation for proxy use, and research shows that proxies often rate impairments more severely than patients. It is essential for studies to report how proxy responses are managed and to conduct sensitivity analyses excluding these responses to evaluate their effect on findings.
6.4.1 Study Subject Considerations
7. Instrumentation [10]
7.1 Selection of Pre-existing HRQOL Instrument:
The selected HRQoL instrument must align with the study's goals and be relevant to the patient group. It should be available in a comprehensible language, culturally appropriate, and suitable for the reading level of the population studied. Modifications to existing instruments require caution, as they can impact validity, and any necessary changes, including translations or adaptations, require permission from the original developer.
7.2 Creation of the HRQoL Instrument:
Developing a new Health-Related Quality of Life (HRQoL) instrument necessitates a clear rationale and adherence to essential steps: defining the patient population, conducting a literature review, creating a conceptual model, generating domain-specific items, offering adequate response options, and engaging experts and patients via interviews. Field testing is crucial to ensure the survey is concise, easy to complete, and acceptable to respondents. Validating the instrument is essential, and opting for an existing validated measure is generally recommended to minimize the extensive work involved in development.
7.3 Assessment of the HRQoL Instrument[11]
All health-related quality of life (HRQoL) instruments must be validated in the specific patient population they are used in, referencing relevant literature for validity and reliability or assessing key psychometric properties. Modifications, including translation and cultural adaptation, need clear descriptions and re-evaluation of psychometric properties. Established guidelines by Hall et al. and Beaton et al. offer recommendations for these processes, ensuring accurate measurement of outcomes in intended patient groups.
Content validity in HRQoL instruments ensures relevance and comprehensiveness for the measured concept and studied population. Evaluation methods include expert opinions and qualitative patient stakeholder input. Floor and ceiling effects, occurring when over 15% of respondents select the lowest or highest response options, can diminish response variability, complicating differentiation between patients and detecting changes. Significant floor or ceiling effects thus undermine the instrument's capacity to measure meaningful differences or improvements.
Construct validity of an HRQoL instrument assesses its effectiveness in measuring the intended theoretical concept. This is evaluated through convergent validity, where strong correlations exist with similar constructs (e.g., anxiety and depression). Discriminant validity ensures low or no correlation with unrelated constructs (e.g., anxiety and physical functioning). Additionally, demonstrating expected differences in HRQoL scores among groups differing in characteristics, such as illness severity, supports construct validity. These assessments collectively confirm the instrument's reliability in measuring health-related quality of life.
Reliability of an HRQoL instrument means it should consistently produce stable and repeatable results. For comparisons made at the group level, it is recommended that the reliability coefficient be at least 0.70.
Responsiveness in HRQoL instruments refers to their ability to capture meaningful changes in health status over time, typically assessed by detecting statistically significant variations in HRQoL domains among patients who report improvement or deterioration. Demonstrating responsiveness also enables the determination of minimal important differences (MIDs), which establish thresholds for clinically relevant change. In addition, methods such as factor analysis and item response theory (IRT) support instrument validation and refinement by examining item relationships, verifying domain structures, and evaluating reliability.
REFERENCES



P. T. Nagaraju, B. V. Ramana, Y. Sai Pravallika, Review Article on Health Related Quality of Life, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 720-727. https://doi.org/10.5281/zenodo.17294810
 10.5281/zenodo.17294810
10.5281/zenodo.17294810
