The purpose of review to highlight benefits of Ibuprofen over other NSAIDs. A comprehensive analysis of clinical studies, including randomized controlled trials, meta-analyses, and observational research, was conducted to evaluate outcomes in various conditions such as musculoskeletal injuries, osteoarthritis, rheumatoid arthritis, and postoperative pain. The data reveal that ibuprofen provides effective analgesia comparable to other NSAIDs while often exhibiting a more favorable gastrointestinal safety profile. However, differences in pharmacokinetics, dosage regimens, and patient-specific factors play a critical role in its clinical performance relative to agents like diclofenac, naproxen, & selective COX-2 inhibitors (NSAIDs). Additionally, the risk of adverse cardiovascular events varied across studies, underscoring the need for personalized therapeutic strategies. The findings highlight that while ibuprofen remains a reliable first-line option for many patients, individualized treatment decisions based on overall health status, comorbidities, and specific clinical scenarios are essential. This review offers key insights for doctors, pharmacist and researchers striving to optimize pain management protocols.
Keywords
Ibuprofen, NSAIDs, Anti-Inflammatory Drug, Anti-Pyretic, OTC Drug
Introduction
×
Ibuprofen is a widely used non-steroidal anti-inflammatory drug (NSAIDs) that is effective for relieving pain, reducing fever, and treating inflammation. It was developed by Dr. Stewart Adams & Colleagues & first marketed in the United Kingdom in 1969. [1,2] non-steroidal anti- inflammatory drugs (NSAIDs) have long served as a cornerstone in managing pain and inflammation across a wide array of clinical conditions. Their primary mechanism—blocking cyclooxygenase (COX) enzymes—leads to reduced prostaglandin synthesis, [3,4] a pathway central to both pain and inflammatory responses. Among these agents, ibuprofen has become one of the most widely used due to its established efficacy, favourable tolerability, and ready over-the- counter availability. [5,6] However, the landscape of NSAID therapy is far from monolithic. With the availability of numerous alternatives such as diclofenac, naproxen, and selective COX-2 inhibitors, there is a pressing need to scrutinize whether the clinical benefits of ibuprofen measure up favourably against its counterparts.[7] The impetus for this comparative exploration arises from both the clinical and pharmacological nuances that differentiate these drugs. Variations in molecular structure, COX isoenzyme selectivity, pharmacokinetics, and dosing strategies have translated into subtle—but sometimes significant—differences in therapeutic outcomes. Emerging randomized controlled trials, observational studies, and meta-analyses point to differences in analgesic potency, speed of onset, and safety profiles among NSAIDs. Clinicians today must balance these variables against individual patient factors, such as gastrointestinal or cardiovascular risk, comorbid conditions, and even socioeconomic considerations, to tailor optimal therapy.[8] This review aims to synthesize current evidence on the efficacy of ibuprofen relative to other NSAIDs. By examining differences in molecular mechanisms and clinical performance, we seek to offer a comprehensive perspective that supports evidence-based decision-making in the management of pain and inflammation. This comparative approach also aims to identify areas of debate and potential research gaps that may guide future investigations and improve patient care [1,7,11].
Fig 1.1 Mechanism of Action of Ibuprofen
Pharmacokinetics
Absorption: Rapidly absorbed from the gastrointestinal tract Peak plasma concentration: 1–2 hours after oral administration Bioavailability: ~80–100%.
Distribution: Extensively bound to plasma proteins (~99%) Widely distributed in tissues, especially at sites of inflammation.
Metabolism: Primarily metabolized in the liver via cytochrome P450 enzymes (mainly CYP2C9) Converts to inactive hydroxylated and carboxylate metabolites.
Excretion: Eliminated mainly via the kidneys (urine) Half-life: 2–4 hours in most individuals. Therapeutic
ACE inhibitors/ARBs: Reduced antihypertensive effect, risk of renal impairment.
Lithium: Increased lithium levels
Methotrexate: Increased toxicity risk.
Special Considerations: Avoid in patients with peptic ulcer disease, renal impairment, or severe heart failure Use with caution in pregnancy (especially 3rd trimester) Pediatric and geriatric dosing requires special care.[13]
A carboxylic acid group an aromatic ring with an isobutyl substituent at the para position A chiral center at the alpha carbon to the carboxyl group It is a racemic mixture, but the (S)-enantiomer is the pharmacologically active form (COX inhibition) SAR (Structure–Activity Relationship) of Ibuprofen Essential Features for Activity: Metabolism Primary site: Liver (via CYP2C9) Major pathways: Oxidation to inactive metabolites Conjugation (glucuronidation) for renal excretion. Primarily through urine Related Compounds Ibuprofen is part of the aryl propionic acid derivatives (profens), and analogs include: Naproxen Ketoprofen Flurbiprofen These maintain the carboxylic acid and aromatic moiety but vary in the side chains for potency and selectivity.[1]
SAR (Structural Activity Relationship)
Table 1.1 SAR of Ibuprofen [1,14]
Structural Component
SAR Insight
Carboxylic Acid (-COOH)
Crucial for binding to the COX enzyme active site; forms hydrogen bonds.
Aromatic Ring
Provides lipophilicity, essential for fitting into the hydrophobic pocket of the COX enzyme.
Para-lsobutyl Group
Enhances hydrophobic interactions and increases anti-inflammatory potency.
Alpha-Methyl Group (on propanoic acid Contributes to chirality and chain)
improves fit in COX active site; (S) - enantiomer has much higher activity.
Advantages of Ibuprofen over other NSAIDs
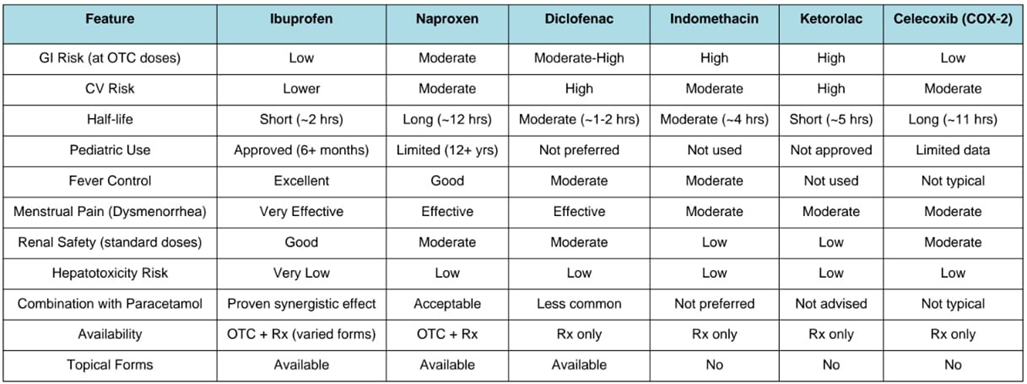
Lower Gastrointestinal (GI) Risk (at OTC doses): Compared to NSAIDs like naproxen or indomethacin, ibuprofen tends to have a lower risk of causing GI side effects (e.g., ulcers, bleeding) when used at over-the-counter (OTC) doses.[15]
Shorter Half-life: Ibuprofen has a relatively short half-life (about 2 hours), allowing for more flexible dosing and quicker elimination, which may reduce the risk of prolonged side effects.[13]
Better Tolerability: It is generally well-tolerated by a broad population and is often recommended for children and elderly patients (under supervision), unlike some stronger NSAIDs.[1]
Lower Cardiovascular Risk (compared to diclofenac): Ibuprofen has a lower associated risk of cardiovascular events than diclofenac or COX-2 selective inhibitors like celecoxib.[7]
Widely Available and Cost-effective: It’s inexpensive, available in various forms (tablet, liquid, topical), and sold worldwide both OTC and by prescription.[1]
Antipyretic Efficacy: Ibuprofen is particularly effective in reducing fever. It's often preferred over acetaminophen in pediatric cases due to its dual antipyretic and anti-inflammatory effects.[17]
Effective in Dysmenorrhea: Studies have shown ibuprofen to be especially effective for menstrual cramps compared to other NSAIDs, likely due to its strong inhibition of prostaglandin synthesis in the uterus.[18]
Lower Risk of Renal Side Effects (at standard doses): When used in appropriate doses and durations, ibuprofen poses a lower risk of nephrotoxicity compared to more potent NSAIDs like ketorolac or indomethacin.[19]
Pediatric Safety: Ibuprofen is approved for use in children over 6 months, with a well- established safety profile, making it one of the few NSAIDs used in pediatric populations.[20]
Combination Flexibility: It is often used safely in combination with acetaminophen (paracetamol) for enhanced pain and fever relief, particularly in acute pain and post-operative scenarios.[21]
Available in Multiple Routes: Available orally, topically, and in IV formulations (e.g., for perioperative pain), allowing tailored use depending on clinical context.[1]
Low Risk of Hepatotoxicity: Unlike acetaminophen, ibuprofen does not typically cause liver damage, which is beneficial in patients with hepatic concerns.[22]
Table 1.2 Advantages of Ibuprofen over other NSAIDs [1, 6, 7, 21, 22, 23]
Therapeutic Uses
Ibuprofen is among the most versatile NSAIDs used for a broad range of clinical conditions: Acute Pain and Postoperative Relief: Single oral doses (200–400 mg) effectively manage postoperative pain in adults, with number-needed-to-treat (NNT) values between 2 and 4, comparable to other NSAIDs.[5] The intravenous formulation (100–400 mg) offers similar analgesic efficacy with fewer adverse effects compared to ketorolac, making it valuable in perioperative settings.[10]
Musculoskeletal and Rheumatoid Conditions: Widely used for osteoarthritis, rheumatoid arthritis, and juvenile idiopathic arthritis, ibuprofen alleviates joint pain, stiffness, and swelling—often as a first-line, over-the-counter agent.[12]
Dysmenorrhea: Ibuprofen remains the gold standard for menstrual pain, significantly reducing uterine prostaglandin levels and cramp severity; its OTC availability provides convenient access.[18]
Fever Management: Superior to acetaminophen in pediatric fever reduction due to combined antipyretic and anti-inflammatory effects, with strong evidence supporting use beyond infancy.[20, 17] Headache, Dental, and Renal Colic Pain: Effective for tension and migraine headaches, dental procedure pain, and renal colic by mitigating prostaglandin-mediated nociception. [12]
Topical and Acne Use: Selected topical applications target superficial inflammation, such as acne, though evidence is currently limited.
Neurological Protection (Early Data): Epidemiological studies suggest a possible reduced risk of neurodegenerative diseases (e.g., Parkinson’s), though causation remains unconfirmed.[20]
Adverse Effects and Safety Profile
Gastrointestinal (GI) Effects: Ibuprofen causes acid-related GI irritation and diminishes protective prostaglandins, leading to dyspepsia, ulcers, and bleeding. Estimated risk includes up to 20% of users developing GI discomfort, with serious complications significantly less frequent at OTC doses.[21, 24]
Higher doses and long-term use elevate the risks, but ibuprofen has a lower ulcerogenic profile than NSAIDs like indomethacin or piroxicam.[12,21]
Renal Effects: Prostaglandin inhibition constricts glomerular arterioles, reducing renal blood flow and GFR. Short-term use is usually safe in healthy individuals,[11] while chronic or high-dose use in vulnerable populations—elderly, heart failure, dehydrated patients—may precipitate acute kidney injury and fluid retention. [24]
Cardiovascular Risks: At doses ≥2400 mg/day, ibuprofen moderately increases risks of hypertension, myocardial infarction, and stroke. In lower, OTC doses and limited duration, cardiovascular risk is minimal compared to COX?2 inhibitors and diclofenac. [6, 8, 22, 23] A 2015 FDA advisory reiterates concern for high?dose uses. [20]
Other Adverse Effects
Hypersensitivity: Asthma exacerbations, urticaria, and rare severe reactions (e.g., Stevens– Johnson syndrome) occur, particularly in COX?1-sensitive individuals [21].
Skin: Potential for bullous dermatoses and photosensitivity, though noted to be weaker compared to other profens. [21]
Hepatic: Rare liver enzyme elevations, but generally lower hepatotoxicity risk than acetaminophen. [33]
Hematologic: Reversible platelet inhibition may interfere with aspirin cardioprotection when taken concurrently; timing should be managed accordingly [21].
Pregnancy: Use after 20 weeks gestation should be avoided due to fetal renal effects and oligohydramnios risk. [21]
Recent Research and Advances
Intravenous Ibuprofen in Acute Care: Recent hospital-based studies show IV ibuprofen use is linked to fewer adverse drug reactions and lower healthcare resource utilization compared to ketorolac, making it a favorable choice in acute and postoperative settings.[10]
Ibuprofen Analogues and Drug Design: Efforts aim to synthesize ibuprofen derivatives with retained anti-inflammatory activity but diminished side effects. New analogues are in preclinical stages targeting enhanced selectivity and reduced GI/renal toxicity.[4]
Pediatric and Fast-track Surgery Applications: Ibuprofen is increasingly utilized in pediatric fast-track cardiac and day-care surgery analgesia. Its ability to reduce opioid consumption and limit postoperative nausea/vomiting without major renal issues is particularly advantageous.[17]
Neuroprotective Potential: While epidemiological associations hint at neuroprotective benefits (e.g., Parkinson’s risk reduction), conclusive clinical trials are lacking. This remains an active area of investigation. [20]
Global Access and Public Health: Despite universal listing on WHO’s essential medicines list, misuse and lack of education continue globally, particularly in low- and middle-income countries, raising concerns over irrational use and preventable harm. [7,9]
CONCLUSION
In summary, ibuprofen remains a widely used and effective NSAID for managing various pain conditions, demonstrating comparable analgesic efficacy to other NSAIDs while often offering a more favorable gastrointestinal safety profile. Its pharmacokinetic properties, dosage flexibility, and accessibility make it a reliable choice for first-line treatment in musculoskeletal injuries, osteoarthritis, rheumatoid arthritis, and postoperative pain. However, individual patient factors, including cardiovascular risk and co-morbidities, necessitate careful selection to optimize therapeutic outcomes. As clinical evidence continues to evolve, healthcare professionals must adopt a personalized approach when prescribing NSAIDs, ensuring a balance between efficacy and safety. This review underscores the importance of tailoring treatment strategies to individual patient needs, reinforcing ibuprofen’s role as a versatile and dependable option in pain management protocols. Future research should further explore comparative long-term safety and effectiveness to refine prescribing guidelines.
REFERENCES
Rainsford, K. D. (2011). Ibuprofen: Discovery, development and therapeutics. Inflammopharmacology, 19(3), 105–113. https://doi.org/10.1007/s10787-010-0062-z
Sneader, W. (2005). Drug Discovery: A History. Wiley. (for historical development of ibuprofen)
Vane, J. R., & Botting, R. M. (1998). Mechanism of action of anti-inflammatory drugs. International Journal of Tissue Reactions, 20(1), 3–15.
Dubois, R. N., et al. (1998). Cyclooxygenase in biology and disease. FASEB J.
Derry, C. J., Derry, S., & Moore, R. A. (2015). Single dose oral ibuprofen for acute postoperative pain in adults. Cochrane Database of Systematic Reviews, (7), CD001548. https://doi.org/10.1002/14651858.CD001548.pub2
Moore, R. A., Derry, S., & McQuay, H. J. (2009). Adverse outcomes with long-term use of NSAIDs: a systematic review of observational studies. BMC Musculoskeletal Disorders, 10, 90. https://doi.org/10.1186/1471-2474-10-90
McGettigan, P., & Henry, D. (2011). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: An examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Med, 8 (2), e1000381. https://doi.org/10.1371/journal.pmed.1000381
Bally, M., et al. (2017). Myocardial infarction risks with NSAIDs. BMJ
McGettigan, P., & Henry, D. (2013). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Medicine, 10(2), e1001388. https://doi.org/10.1371/journal.pmed.1001388
Moore, R. A., Derry, S., McQuay, H. J., & Wiffen, P. J. (2008). Single dose oral analgesics for acute postoperative pain in adults – an overview of Cochrane reviews. Cochrane Database of Systematic Reviews, (1), CD008659. https://doi.org/10.1002/14651858.CD008659.pub2
Ong, C. K. S., Lirk, P., Tan, C. H., & Seymour, R. A. (2007). An evidence-based update on nonsteroidal anti-inflammatory drugs. Clinical Medicine & Research, 5(1), 19–34. https://doi.org/10.3121/cmr.2007.698
Vane, J. R., & Botting, R. M. (1998). Mechanism of action of anti-inflammatory drugs. The American Journal of Medicine, 104(3A), 2S–8S. https://doi.org/10.1016/S0002- 9343(98)00091-1
Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (Eds.). (2018). Goodman & Gilman's: The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill Education.
Kalgutkar, A. S., & Zhao, S. Z. (2001). Discovery and design of selective cyclooxygenase- 2 inhibitors as nonulcerogenic anti-inflammatory agents. Current Topics in Medicinal Chemistry, 1(5), 345–367.
Moore, N., Pollack, C., & Butkerait, P. (2015). Adverse drug reactions and drug–drug interactions with over-the-counter NSAIDs. Therapy, 12(1), 45–55..
Perrott, D. A., Piira, T., Goodenough, B., & Champion, G. D. (2004). Efficacy and safety of acetaminophen vs ibuprofen for treating children's pain or fever: A meta-analysis. Archives of Pediatrics & Adolescent Medicine, 158(6), 521–526. https://doi.org/10.1001/archpedi.158.6.521
Zahradnik, H. P., Hanjalic-Beck, A., & Groth, K. (2010). Nonsteroidal anti-inflammatory drugs and hormonal contraceptives for pain relief from dysmenorrhea: A review. Gynecological Endocrinology, 26(9), 673–676.
Whelton, A. (1999). Nephrotoxicity of nonsteroidal anti-inflammatory drugs: Physiologic foundations and clinical implications. The American Journal of Medicine, 106(5B), 13S– 24S.
Kanabar, D. J. (2017). A clinical and safety review of paracetamol and ibuprofen in children. Inflammopharmacology, 25, 1–9.
Purssell, E. (2011). Systematic review of studies comparing combined treatment with paracetamol and ibuprofen to either drug alone. Archives of Disease in Childhood, 96(12), 1175–1179.
Chou, R., et al. (2016). Management of Postoperative Pain: A Clinical Practice Guideline. The Journal of Pain, 17(2), 131–157.
Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th Ed. (2018).
Rainsford, K. D. (2009). Ibuprofen: pharmacology, efficacy and safety. Inflammopharmacology, 17(6), 275–342. https://doi.org/10.1007/s10787-009-0016-x
Deeks, J. J., Smith, L. A., & Derry, S. (2002). Paracetamol, ibuprofen, and their combination for pain relief after oral surgery: a quantitative systematic review. British Dental Journal, 193(6), 377–383. https://doi.org/10.1038/sj.bdj.4801558
Farkouh, M. E., Greenberg, J. D., & Jeger, R. V. (2007). Cardiovascular risk of NSAIDs: past, present and future. The American Journal of Cardiology, 99(6A), 12C–18C. https://doi.org/10.1016/j.amjcard.2006.12.002
McGettigan, P., & Henry, D. (2013). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLOS Medicine, 10(2), e1001388. https://doi.org/10.1371/journal.pmed.1001388
Rainsford, K. D. (2009). Ibuprofen: pharmacology, efficacy and safety. Inflammopharmacology, 17(6), 275–342. https://doi.org/10.1007/s10787-009-0016-x
Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (Eds.). (2017). Goodman & Gilman's: The pharmacological basis of therapeutics (13th ed.). McGraw-Hill Education.
Davies, N. M. (1998). Clinical pharmacokinetics of ibuprofen. The first 30 years. Clinical Pharmacokinetics, 34(2), 101–154. https://doi.org/10.2165/00003088-199834020-00002
U.S. Food and Drug Administration (FDA). (2018). Ibuprofen Drug Label Information. Retrieved from https://www.accessdata.fda.gov
National Center for Biotechnology Information. (2024). PubChem Compound Summary for CID 3672, Ibuprofen. PubChem, U.S. National Library of Medicine. Retrieved from https://pubchem.ncbi.nlm.nih.gov/compound/Ibuprofen
Silverman, R. B., & Holladay, M. W. (2014). The Organic Chemistry of Drug Design and Drug Action (3rd ed.). Academic Press.
Nahata, M. C., & Powell, D. A. (2000). Safety and efficacy of ibuprofen in children. Clinical Pediatrics, 39(8), 427–434. https://doi.org/10.1177/000992280003900801
Warden, S. J. (2010). Prophylactic use of NSAIDs by athletes: A risk/benefit assessment. The Physician and Sportsmedicine,38 (1), 132–138. https://doi.org/10.3810/psm.2010.04.1768
Marjoribanks, J., Ayeleke, R. O., Farquhar, C., & Proctor, M. (2015). Nonsteroidal anti- inflammatory drugs for dysmenorrhoea. Cochrane Database of Systematic Reviews, (7), CD001751. https://doi.org/10.1002/14651858.CD001751.pub3
Singla, N., Rock, A., & Pavliv, L. (2010). A review of the clinical efficacy and safety of intravenous ibuprofen for pain in adults. Clinical Therapeutics, 32(11), 2027–2052. https://doi.org/10.1016/j.clinthera.2010.11.013
Watkins, P. B., Kaplowitz, N., Slattery, J. T., Colonese, C. R., Colucci, S. V., Stewart, P. W., & Harris, S. C. (2006). Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: A randomized controlled trial. JAMA, 296(1), 87–93. https://doi.org/10.1001/jama.296.1.87.
Reference
Rainsford, K. D. (2011). Ibuprofen: Discovery, development and therapeutics. Inflammopharmacology, 19(3), 105–113. https://doi.org/10.1007/s10787-010-0062-z
Sneader, W. (2005). Drug Discovery: A History. Wiley. (for historical development of ibuprofen)
Vane, J. R., & Botting, R. M. (1998). Mechanism of action of anti-inflammatory drugs. International Journal of Tissue Reactions, 20(1), 3–15.
Dubois, R. N., et al. (1998). Cyclooxygenase in biology and disease. FASEB J.
Derry, C. J., Derry, S., & Moore, R. A. (2015). Single dose oral ibuprofen for acute postoperative pain in adults. Cochrane Database of Systematic Reviews, (7), CD001548. https://doi.org/10.1002/14651858.CD001548.pub2
Moore, R. A., Derry, S., & McQuay, H. J. (2009). Adverse outcomes with long-term use of NSAIDs: a systematic review of observational studies. BMC Musculoskeletal Disorders, 10, 90. https://doi.org/10.1186/1471-2474-10-90
McGettigan, P., & Henry, D. (2011). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: An examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Med, 8 (2), e1000381. https://doi.org/10.1371/journal.pmed.1000381
Bally, M., et al. (2017). Myocardial infarction risks with NSAIDs. BMJ
McGettigan, P., & Henry, D. (2013). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Medicine, 10(2), e1001388. https://doi.org/10.1371/journal.pmed.1001388
Moore, R. A., Derry, S., McQuay, H. J., & Wiffen, P. J. (2008). Single dose oral analgesics for acute postoperative pain in adults – an overview of Cochrane reviews. Cochrane Database of Systematic Reviews, (1), CD008659. https://doi.org/10.1002/14651858.CD008659.pub2
Ong, C. K. S., Lirk, P., Tan, C. H., & Seymour, R. A. (2007). An evidence-based update on nonsteroidal anti-inflammatory drugs. Clinical Medicine & Research, 5(1), 19–34. https://doi.org/10.3121/cmr.2007.698
Vane, J. R., & Botting, R. M. (1998). Mechanism of action of anti-inflammatory drugs. The American Journal of Medicine, 104(3A), 2S–8S. https://doi.org/10.1016/S0002- 9343(98)00091-1
Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (Eds.). (2018). Goodman & Gilman's: The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill Education.
Kalgutkar, A. S., & Zhao, S. Z. (2001). Discovery and design of selective cyclooxygenase- 2 inhibitors as nonulcerogenic anti-inflammatory agents. Current Topics in Medicinal Chemistry, 1(5), 345–367.
Moore, N., Pollack, C., & Butkerait, P. (2015). Adverse drug reactions and drug–drug interactions with over-the-counter NSAIDs. Therapy, 12(1), 45–55..
Perrott, D. A., Piira, T., Goodenough, B., & Champion, G. D. (2004). Efficacy and safety of acetaminophen vs ibuprofen for treating children's pain or fever: A meta-analysis. Archives of Pediatrics & Adolescent Medicine, 158(6), 521–526. https://doi.org/10.1001/archpedi.158.6.521
Zahradnik, H. P., Hanjalic-Beck, A., & Groth, K. (2010). Nonsteroidal anti-inflammatory drugs and hormonal contraceptives for pain relief from dysmenorrhea: A review. Gynecological Endocrinology, 26(9), 673–676.
Whelton, A. (1999). Nephrotoxicity of nonsteroidal anti-inflammatory drugs: Physiologic foundations and clinical implications. The American Journal of Medicine, 106(5B), 13S– 24S.
Kanabar, D. J. (2017). A clinical and safety review of paracetamol and ibuprofen in children. Inflammopharmacology, 25, 1–9.
Purssell, E. (2011). Systematic review of studies comparing combined treatment with paracetamol and ibuprofen to either drug alone. Archives of Disease in Childhood, 96(12), 1175–1179.
Chou, R., et al. (2016). Management of Postoperative Pain: A Clinical Practice Guideline. The Journal of Pain, 17(2), 131–157.
Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th Ed. (2018).
Rainsford, K. D. (2009). Ibuprofen: pharmacology, efficacy and safety. Inflammopharmacology, 17(6), 275–342. https://doi.org/10.1007/s10787-009-0016-x
Deeks, J. J., Smith, L. A., & Derry, S. (2002). Paracetamol, ibuprofen, and their combination for pain relief after oral surgery: a quantitative systematic review. British Dental Journal, 193(6), 377–383. https://doi.org/10.1038/sj.bdj.4801558
Farkouh, M. E., Greenberg, J. D., & Jeger, R. V. (2007). Cardiovascular risk of NSAIDs: past, present and future. The American Journal of Cardiology, 99(6A), 12C–18C. https://doi.org/10.1016/j.amjcard.2006.12.002
McGettigan, P., & Henry, D. (2013). Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLOS Medicine, 10(2), e1001388. https://doi.org/10.1371/journal.pmed.1001388
Rainsford, K. D. (2009). Ibuprofen: pharmacology, efficacy and safety. Inflammopharmacology, 17(6), 275–342. https://doi.org/10.1007/s10787-009-0016-x
Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (Eds.). (2017). Goodman & Gilman's: The pharmacological basis of therapeutics (13th ed.). McGraw-Hill Education.
Davies, N. M. (1998). Clinical pharmacokinetics of ibuprofen. The first 30 years. Clinical Pharmacokinetics, 34(2), 101–154. https://doi.org/10.2165/00003088-199834020-00002
U.S. Food and Drug Administration (FDA). (2018). Ibuprofen Drug Label Information. Retrieved from https://www.accessdata.fda.gov
National Center for Biotechnology Information. (2024). PubChem Compound Summary for CID 3672, Ibuprofen. PubChem, U.S. National Library of Medicine. Retrieved from https://pubchem.ncbi.nlm.nih.gov/compound/Ibuprofen
Silverman, R. B., & Holladay, M. W. (2014). The Organic Chemistry of Drug Design and Drug Action (3rd ed.). Academic Press.
Nahata, M. C., & Powell, D. A. (2000). Safety and efficacy of ibuprofen in children. Clinical Pediatrics, 39(8), 427–434. https://doi.org/10.1177/000992280003900801
Warden, S. J. (2010). Prophylactic use of NSAIDs by athletes: A risk/benefit assessment. The Physician and Sportsmedicine,38 (1), 132–138. https://doi.org/10.3810/psm.2010.04.1768
Marjoribanks, J., Ayeleke, R. O., Farquhar, C., & Proctor, M. (2015). Nonsteroidal anti- inflammatory drugs for dysmenorrhoea. Cochrane Database of Systematic Reviews, (7), CD001751. https://doi.org/10.1002/14651858.CD001751.pub3
Singla, N., Rock, A., & Pavliv, L. (2010). A review of the clinical efficacy and safety of intravenous ibuprofen for pain in adults. Clinical Therapeutics, 32(11), 2027–2052. https://doi.org/10.1016/j.clinthera.2010.11.013
Watkins, P. B., Kaplowitz, N., Slattery, J. T., Colonese, C. R., Colucci, S. V., Stewart, P. W., & Harris, S. C. (2006). Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: A randomized controlled trial. JAMA, 296(1), 87–93. https://doi.org/10.1001/jama.296.1.87.
J. B. Shinde
Corresponding author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
J. B. Shinde
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
U. A. Shaikh
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
M. K. Khan
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
S. B. Gaikwad
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
A. P. Ingole
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
S. D. Giram
Co-author
Department of Pharmaceutical Chemistry, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
J. B. Shinde*, Dr. R. D. Ingole, U. A. Shaikh, M. K. Khan, S. D. Giram, S. B. Gaikwad, A. P. Ingole, Review On: Comparative Efficacy of Ibuprofen over Other NSAIDs, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 3571-3579. https://doi.org/10.5281/zenodo.15720048




 10.5281/zenodo.15720048
10.5281/zenodo.15720048