School of Pharmaceutical Sciences, Sandip University. Nashik
Diabetes presents as a persistent metabolic condition characterized by insufficient insulin levels in the body, resulting in the inability to regulate blood sugar effectively. Patients with diabetes typically rely on frequent insulin injections to manage their blood glucose levels within the normal range. Unfortunately, this method of administration is often uncomfortable for individuals. Individuals with advanced type 2 diabetes mellitus (T2DM) and all those with type 1 diabetes mellitus (T1DM) require insulin to maintain optimal blood sugar levels. The primary approach to deliver insulin is through subcutaneous injections. Various options exist for subcutaneous insulin delivery, including traditional vials and syringes, convenient insulin pens, and modern insulin pumps. Previously, inhaled insulin offered a non-invasive alternative, but it has since been removed from the market. In order to improve the adaptability of patients to use insulin and reduce the pain caused by injection, the development of oral insulin formulations is currently a topic.
Diabetes ranks among the top ten illnesses posing a threat to human health worldwide, and it stands as one of the most rapidly expanding global health emergencies in the 21st century.
Having a peptide hormone nature, insulin faces the risk of being destroyed by gastric acid when consumed orally. [1] The intradermal absorption method lacks reliability and fails to replicate natural insulin secretion. Additionally, intradermal, intramuscular, and intravenous modes of therapy are unsuitable for daily self-administration. [2] Hence, subcutaneous delivery remains the favoured choice due to its simplicity in self-administering.
The first research on oral insulin dates back several decades, with early studies exploring the feasibility of delivering insulin via the oral route as an alternative to injections [3] They investigated the possibility of administering insulin orally by encapsulating it in gelatine capsules. [4] Although this early attempt showed limited success due to the degradation of insulin by digestive enzymes and poor absorption in the gastrointestinal tract. [5]
The Physicochemical Properties of Insulin:
Molecular Weight: Insulin has a relatively small molecular weight compared to many other proteins, with approximately 5,800 Daltons (Da) for the human insulin molecule.
Structure: Comprised of two peptide chains, A and B, linked by disulphide bonds, insulin has a tertiary structure essential for its biological function. The A chain contains 21 amino acids, while the B chain consists of 30 amino acids.
Solubility: While insulin is soluble in water at acidic pH levels, it tends to aggregate and precipitate in neutral or alkaline conditions. This characteristic plays a crucial role in its stability and the process of formulating injectable preparations.
Stability: Insulin’s stability is influenced by temperature, pH, and agitation. Exposure to extreme temperatures or pH levels can lead to the degradation of insulin and subsequent loss of its biological function. Proper storage conditions are paramount for maintaining its stability. [6]
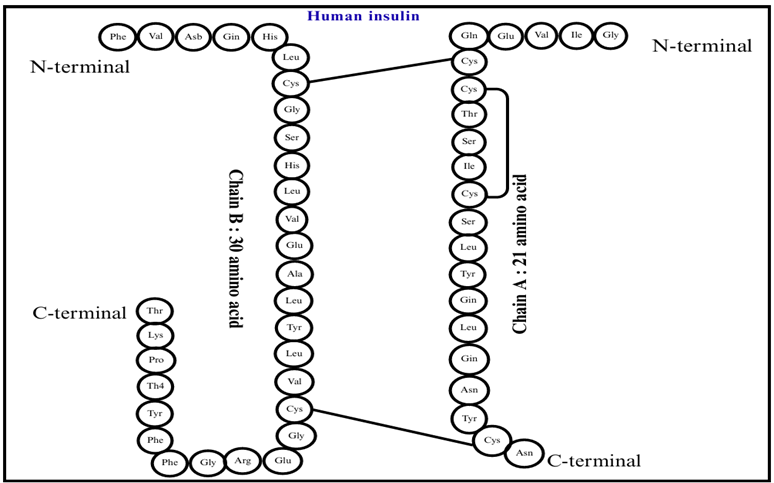
Figure 1: Structure of human insulin
The image shows the structure of human insulin.
It consists of two polypeptide chains, Chain A (21 amino acids) and Chain B (30 amino acids).
The two chains are linked by disulfide bonds, forming the active insulin molecule.
Common signs of Diabetes:
Feeling Thirsty (Polydipsia): A really persistent thirst is often one of the clues that might be present. People end up dinking a lot of water.
Going to bathroom a lot(polyuria): When there’s too much glucose in blood, the kidney to work harder. To cause it folks to urinate more frequently to get rid of that extra sugar
Feeling Very Hungry(polyphagia): Even if someone eats regularly, they might still feel overly hungry. This happens because the body can’t use glucose well.
Losing weight for no Reason: Especially in Type 1 diabetes, the body may start breaking down muscles & fats. This can lead to weight loss, even if a person eats normally or even more than the usual.
Feeling Tired: High blood sugar can make it tough for one’s body to get enough energy. This often leads to feeling sleepy and worn out.
Vision Problem: High sugar levels can cause swelling in the lens of the eye. This can lead to blurry or unclear vision.
Slow healing cuts or frequent infections: High glucose make it hard for the body to heal and fight infection. So wounds heal slowly and there might me more infection, especially on skin and gums.
Tingling or numbness in hands or feet: Known as neuropathy, this tingling sensation happens because of nerves damage from having high blood sugar for a long time.
Dark skin patches: some folk might notice dark patches that feel velvety often found in neck fold and underarms. This condition is called acanthosis Nigerians and might indicate insulin resistance.
Feeling grumpy and mood swing: changes in the blood sugar can really affect how a person feels leading to irritability or different mood swings. [7]
Sign Specific to Type 1 Diabetes:
Quick development: The symptoms of Type 1 diabetes often appear suddenly and can be pretty serious.
Ketoacidosis: Sometimes people develop a dangerous condition called diabetic ketoacidosis. Symptoms may include nausea vomiting tommy pain rapid breathing and confusion.
Signs specific to Type 2 Diabetes:
Slow development: For type 2 diabetes symptoms may slowly appear over time sometime going unnoticed for year. [8]
Insulin and Blood Sugar
Our body do not support to high blood sugar level for longer period of time. So to resolve this issue we have developed a mechanism to deal with that [9]. The maximum amount of insulin produced is proportional to the magnitude of the rise in blood sugar level. But the problem arises when this insulin mechanism is overworked. For the most of the time that human have been around, we could not get sugar and starch in small amount. It was at certain time of year we found them, now we have got that sugar and starch available all year long. There are also tone or refined sugar and starch in things like breakfast, cereal, cake, chocolates, fruit, juices, sodas. [10]
Because of this change of body reacts differently to insulin. When blood sugar levels stay high all the time, the cells that need to lower those level start to ignore insulin message bit. This is how insulin resistance begins. When insulin hangs around too long, it changes how we make energy. Our body use both glucose and fats for energy. The fat turn into ketone body. But if insulin level is always high, it slows down how many ketones we make us rely more on sugar or glucose for energy instead. Ketone body is super important for our brain health and growth. So when insulin is too high all the time, it limits the ketone we have. That can lead to issues for our brain. when blood sugar stays high, glucose stick to protein in the process called creating AGE (Advanced Glycation End product). These strange molecules can cause the body to react in way that aren’t good triggering autoimmune responses. Over time this can hurt body response and cause other autoimmune issue. So eating lot of sugar and starch cause a lot of chronic illness. [11]
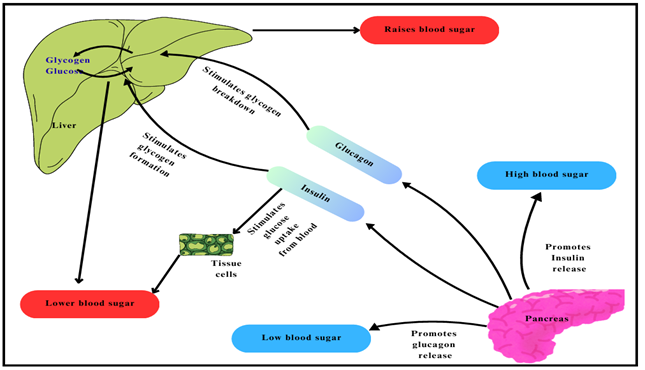
Figure 2: Regulation Of Blood Glucose
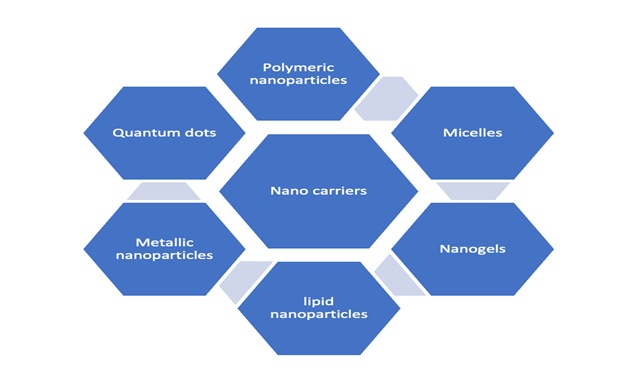
Figure 3: Rate of insulin resistance [12]
This figure shows various factors influencing insulin resistance, including diet, sleep, exercise, stress, genes, and gut bacteria. Lifestyle and genetic factors together determine the body’s response to insulin. Proper management of these factors can help reduce insulin resistance.
Blood sugar enters the blood, signalling the pancreas to secrete Insulin.
Insulin helps blood sugar enter the body’s cells so it can be used as an energy source. Insulin also signals the liver to store blood sugar for later use. Blood sugar enters cells and blood levels decrease, signalling that insulin is also decreasing. Lower insulin levels alert the liver to release stored blood sugar so energy is always available, even if you haven’t eaten in a while. This is when everything works fine. But this finely tuned system can quickly malfunction, as follows: Large amounts of blood sugar enter the bloodstream [13]. The pancreas pumps more insulin to get blood sugar into cells. Over time, the cells stop responding to all that insulin: they become insulin resistant. The pancreas continues to produce more insulin to try to make the cells respond. Eventually, the pancreas can no longer keep up and blood sugar levels continue to rise. Large amounts of sugar in the blood are very harmful to the body and must be delivered to the cells as quickly as possible. [14] There is also a lot of insulin, which protects the liver and muscles from storing blood sugar. When they are full, the liver sends excess sugar in the blood to fat cells to be stored as body fat. Yes, weight gain. And what is more serious is that the stage of prediabetes and Type 2 diabetes has been established. [15]
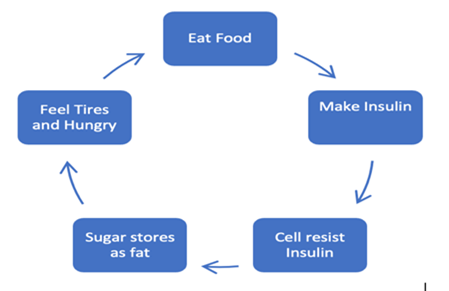
Figure 4: Relationship between Insulin and Blood Sugar
This diagram explains how food intake stimulates insulin secretion.
Insulin regulates blood glucose by promoting cellular uptake and storage of sugar as fat.
Insulin resistance disrupts this cycle, leading to hunger and fatigue.
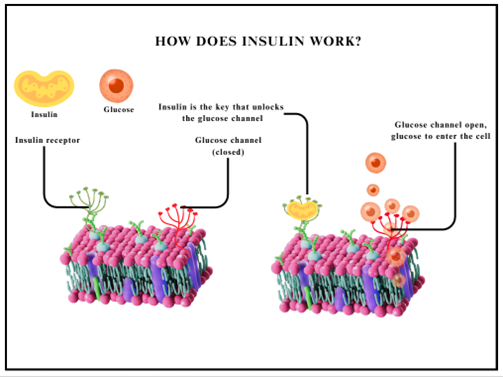
Figure 5: Working of Insulin in human body
The image explains how insulin works at the cellular level.
Insulin binds to its receptor on the cell membrane and opens glucose channels.
This allows glucose to enter the cell and be used for energy.
On the left side cell:
The insulin receptor is present on the cell on which the insulin going to bind The glucose channel is present next to the insulin receptor through which the glucose will pass The glucose channel is temporary closed
On the right side cell: The insulin binds to the receptor, which on further unlocks the glucose channel. Once the channel is unlocked, the glucose starts to enter into the cell [16]
Mechanism of release of insulin
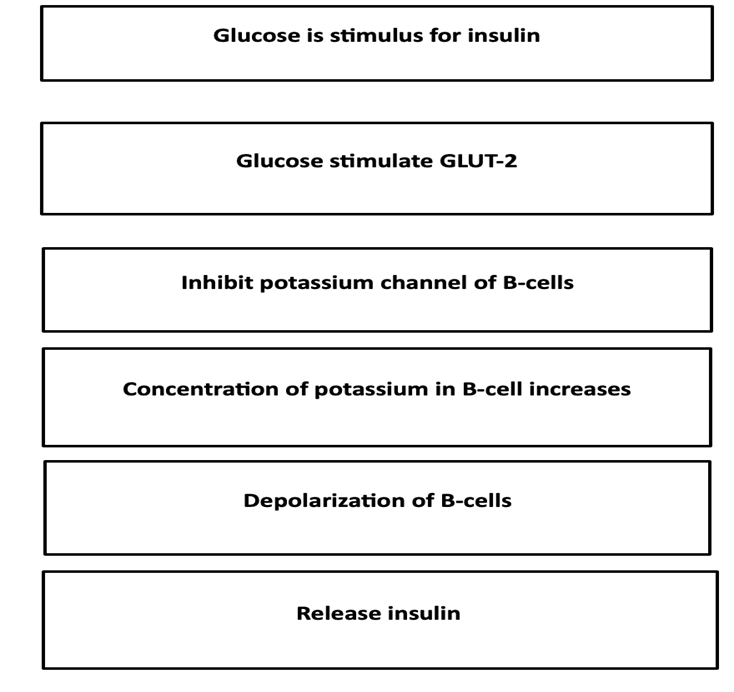
Figure 6 Mechanism of release of insulin [17]
This figure describes how increased blood glucose acts as a stimulus for insulin secretion from pancreatic β-cells. Glucose uptake through GLUT-2 inhibits potassium channels, leading to depolarization of β-cells. This depolarization ultimately triggers the release of insulin.
Action of insulin
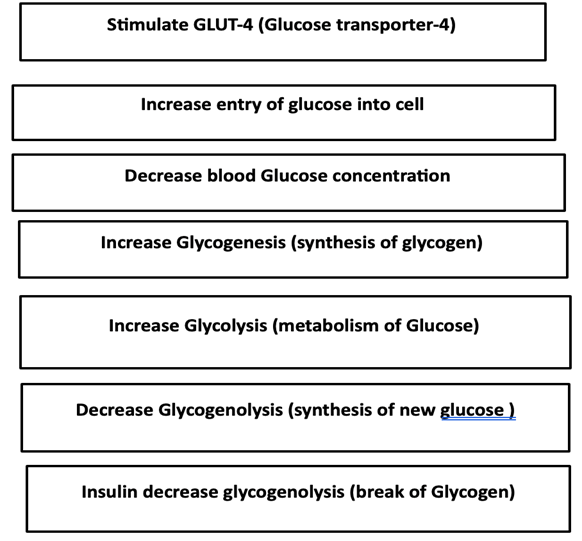
Figure 7: Action of insulin [18]
This diagram explains the role of insulin in regulating blood glucose levels. Insulin stimulates GLUT-4 transporters, increasing glucose uptake by cells and lowering blood glucose concentration. It promotes glycogenesis and glycolysis while inhibiting glucose production and breakdown of glycogen.
Barriers of oral insulin delivery system
GIT causes a series of obstacles to oral insulin absorption, mainly enzymatic, physical, and chemical. Oral medications pass through the GIT. Sticks to the mucus layer, passes through the intestinal epithelium and then enters the blood. However, due to its instability in the gastrointestinal tract and limited epithelial penetration, insulin has very low oral bioavailability (less than 1%). [19]
Pepsin in the stomach, pancreatic in the small intestine (including trypsin, chymotrypsin and elastase) aminopeptidase in the cytosol are the main enzymes involved in protein breakdown in the GIT. [20]
Additionally, if insulin is resistant to the above-mentioned protease, it will most likely be degraded by liver enzymes. [21]
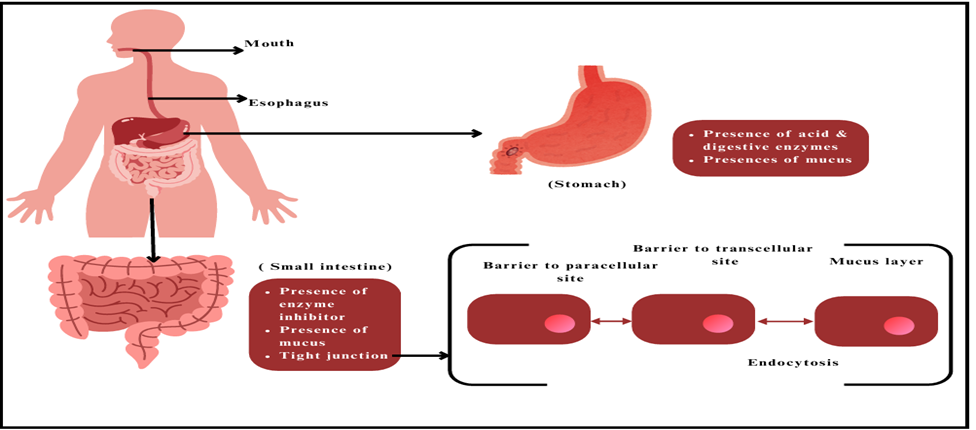
Figure 8: Barriers related to oral insulin
The image shows the digestive tract from mouth to stomach and small intestine.
It highlights the stomach’s acidic environment and the protective mucus layer.
The small intestine is shown as the main site of absorption with barriers and endocytosis.
Barrier is divided into 3 types
Physical barrier: Oral insulin has a tough journey ahead. There are many physical barriers within the digestive system that make delivering insulin through mouth quite challenging. Let's down the main barriers:
A. Mucus layer
The mucus layer acts as a diffusion and enzyme barrier. [22] Polypeptide is encountered due to the continuous secretion of mucus, possibly due to its negative charge. [23] This creates a positively charged drug and protein filter through electrostatic interactions. [24].
1. Viscous Gel: The mucus layer is made up of special proteins called mucins. They create a thick, gel-like substance that covers the cells in the GI tract. This layer is like a protective shield, trapping and blocking larger molecules, including drugs like insulin and even harmful pathogens. [25]
2. Selective Permeability: Size and Charge Barrier: Mucus has a unique way of letting things through. It allows tiny, water-repelling molecules in while keeping out larger, water-attracting ones like insulin. Since insulin is a big protein, it finds it really hard to get through this tight network of mucins. [26]
3. Mucocilliary Clearance: Constant Renewal: The mucus layer is always on the move! It’s produced continuously and shed regularly to clear away trapped particles. This means that insulin can be swept away before it gets the chance to be absorbed by the epithelial surface. [27]
4. Trapping and Degradation: Enzymatic Activity: Sometimes, mucus holds onto insulin for too long. This gives proteolytic enzymes in the GI tract time to break it down, making it even less likely for insulin to pass through the epithelial barrier. [28]
5. Diffusion Barrier Slow Diffusion: The thick, sticky quality of mucus slows down how quickly insulin can diffuse through it. Because of this delay, there’s less concentration of insulin reaching the intestinal wall. [29]
Ways to Tackle the Mucus Barrier
Researchers are working hard to find ways around these mucus hurdles for oral insulin delivery:
1. Mucus-Penetrating Nanoparticles: They’re looking into wrapping insulin in tiny particles specially designed to get past the mucus layer. [30]
2. Mucoadhesive Systems: Other scientists are creating formulas that stick to the mucus and gradually release insulin in targeted spots, improving chances for absorption. [31]
3. Chemical Modifications: There’s also exploration into changing how insulin works or adding ingredients that either break down mucus or help it become more permeable. Even with all these clever strategies, that mucus layer remains a strong barrier in creating effective oral insulin treatments. But hope isn’t lost; scientists keep pushing forward. [32] [33]
B. Intestinal epithelium
It is made up of a single layer of columnar epithelial cells. The difficulty in passive diffusion of lipophilic drugs is < 700 Da in molecular weight and the molecular weight of insulin is 5800 Da. This makes it difficult to pass through the cell by passive diffusion of insulin. An essential physical barrier to the efficient oral administration of insulin is the intestinal epithelium. The main function of this barrier is to control how well drugs enter the bloodstream from the gut. This is how oral insulin administration is affected by it. [34]
1. Selective Permeability: Tight Junctions Between Epithelial Cells Tight junctions, which bind the intestinal epithelial cells together tightly, stop big chemicals like insulin from traveling through the Paracellular pathway and entering individual cells. The absorption of bigger molecules like insulin is severely restricted by these tight junctions, which only permit the passage of water, ions, and tiny molecules. [35]
2. Transcellular Route: Transcellular Transport Challenges Insulin must travel through the cells in order to be absorbed (transcellular pathway). Nevertheless, due to its size and hydrophilicity, insulin finds it difficult to pass through the lipid-rich cell membranes. Because big proteins like insulin typically lack particular transport mechanisms or carriers, it becomes difficult for insulin to be absorbed via this pathway. [36]
3. Efflux Transporters: P-glycoprotein and Other Systems of Efflux: Efflux transporters, such as P-glycoprotein, are found in the intestinal epithelium and actively pump foreign molecules, including some medications, back into the intestinal lumen from the epithelial cells. This reduces the amount of foreign substances that can be absorbed into the circulation. This significantly reduces insulin's oral bioavailability. [37]
4. Enzymatic Barrier:
Degradation within cells: Insulin may be broken down by intracellular enzymes prior to being released into the bloodstream, even if it does manage to penetrate the epithelial cells. Insulin absorption through the mouth is further complicated by this cellular deterioration. [38]
5. Minimum Absorption Sites:
Low Permeability: The intestines surface area is largely used for absorbing nutrients and smaller molecules; hence it is not very large for the absorption of macromolecules like insulin. Insulin's bulk and hydrophilicity, two of its physical and chemical characteristics, cause minimal permeability across the intestinal epithelium. [39]
C. Tight Junction
This is a tight junction between adjacent epithelial cells, effectively sealing the intercellular space between cells and preventing the previous passage of molecules. [40] It plays an important role in regulating the permeability of the epithelial barrier and controlling the transport of ions, water and solutes across the epithelium. In the context of oral insulin delivery, tight junctions greatly hinder the absorption of molecular insulin from the gastrointestinal tract. The size and charge of insulin molecules normally prevent them from passing through tight junctions via the paracellular pathway. Therefore, strategies to overcome tight junctions often involve transcellular insulin permeability, for example using absorption enhancers or transport systems that can facilitate the Epithelial cells absorb insulin. When taken orally, insulin is physically prevented from being absorbed by the intestinal epithelium's tight junctions. This is the precise way that tight connections prevent insulin from being delivered. [41]
1. Tight Junction Structure:
Barrier Function: In the intestine, the distance between neighbouring epithelial cells is sealed by intricate protein structures called tight junctions. They establish a selective barrier that regulates substances' passage across the paracellular space, or the area in between cells. [42]
Selectivity: Due to their extreme selectivity, these junctions mainly permit the passage of very small molecules, water, and tiny ions. Bigger molecules can't fit through the tight connections; one example of this is insulin, a huge protein with a molecular weight of about 5,800 Da. [43]
2. Participation in Paracellular Transport:
Restricted Entry for Big Molecules: The gap between cells that allows chemicals to travel through is known as the paracellular pathway. In order to preserve the integrity and selectivity of the epithelial barrier, tight junctions regulate this area to stop bigger molecules from passing through uncontrollably. [44]
Improving Insulin Absorption Prevention: The tight connections make it difficult for insulin to pass between cells and enter the circulation, which greatly lowers insulin's oral bioavailability. [45]
3. Evolutionary Control:
Dynamic tight junctions can be controlled by a range of physiological and pathological variables. To preserve their barrier role, they are, nevertheless, strictly regulated in normal circumstances. [46]
Avoidance of Pathogen Ingress: Tight junctions serve as the body's first line of defence against the entry of infections and big, potentially dangerous chemicals, such as insulin, which are not normally intended to be absorbed straight from the stomach [47].
4. Effect on Medication Administration:
Difficulty in Absorbing Macromolecules: Tight junctions pose a serious obstacle to macromolecules like insulin because they prevent these molecules from entering the paracellular pathway without external help. [48]
Methods for Breaking Through the Tight Junction Barrier: Scholars are investigating many approaches to surmount the obstacle presented by tightly spaced intersections:
Impression Boosters: These substances have the ability to momentarily damage tight junctions, hence enhancing paracellular permeability and permitting insulin to flow through. The trick is to accomplish this without permanently harming the intestinal barrier. liposomes, nanoparticles, or other delivery methods that work around tight junctions to get insulin beyond the intestinal barrier by using alternate routes. [49]
Chemical Modifications: Changing the structure of insulin to improve its capacity to pass past the intestinal epithelium or permeate it, possibly by receptor-mediated endocytosis or other means. Even though these approaches have potential, tight junctions continue to be one of the biggest barriers to the efficient oral delivery of insulin [50]
Biochemical Barrier
Biochemical barriers to oral insulin administration refer to factors and physiological processes that can interfere with the absorption and bioavailability of orally administered insulin. Although oral insulin delivery is a promising treatment option for diabetes, there are a number of obstacles to overcome, mostly because of the body's innate biochemical barriers. Enzymatic degradation and the harsh environment of the gastrointestinal (GI) tract are the primary obstacles. [51]
The main components of the biochemical barrier include:
1. Enzymatic degradation: Enzymes present in the digestive tract, such as proteases and nucleases, can degrade insulin molecules before absorption. Protection of insulin against enzymatic degradation is important to maintain its biological activity and improve its absorption. Proteolytic Enzymes: A number of proteolytic enzymes, including trypsin, chymotrypsin, and carboxypeptidase in the small intestine and pepsin in the stomach, break down proteins, including insulin, into smaller peptides and amino acids inside the GI tract. These enzymes cause insulin to break down by attacking its peptide bonds. [52]
Barrier to Absorption: The GI tract's epithelial lining acts as an additional barrier to absorption, even in cases where some insulin evades enzymatic breakdown. Since insulin is a big, hydrophilic molecule, it has a hard time getting past enterocytes' lipophilic membrane, which lines the inside of the intestines. [53]
Strategies:
I. Self-Emulsifying Systems and Micro emulsions
Micro emulsions: Insulin can be added to micro emulsions, which are mixes that are thermodynamically stable and shield the hormone from enzymatic breakdown. Additionally, these systems can improve insulin's capacity to pass through intestinal mucosa. In the watery environment of the GI tract, these systems spontaneously produce emulsions that encapsulate insulin and shield it from enzymes. [54]
2. Inhibition of particular enzyme: The development of inhibitors that selectively target enzymes known to decompose insulin, such as DPP-IV or certain proteases in the small intestine, can shield insulin against degradation while minimising off-target effects. This approach is known as Targeted Inhibition. [55]
3. Layer-by-Layer (LbL) - Using this technique, alternating layers of polyelectrolytes are applied to the molecules or particles of insulin. At the site of absorption, each layer permits the controlled release of insulin and can offer extra defence against enzymatic degradation. [56]
II. Gastrointestinal pH
Insulin bioavailability and breakdown affect the acidic environment of the stomach. As we know, insulin is very sensitive to acidic pH and this can lead to denaturation in the stomach, controlling its absorption. Insulin can be protected from acid degradation by coatings or pH regulators 3. Gastrointestinal Environment: Before insulin enters the bloodstream, its acidic pH (between 1.5 and 3.5) in the stomach might denature it and make it inactive. The slightly alkaline (pH 6 to 7.4) environment of the small intestine also plays a role in the instability and subsequent breakdown of insulin. [57] [58]
Strategies of Gastro-intestine
1) Coatings with pH sensitivity: Insulin can be encapsulated as enteric-coated capsules or tablets, which only dissolve in the more neutral to slightly alkaline environment of the small intestine and resist the acidic environment of the stomach. This method releases insulin where absorption is most likely and shields it from being broken down by stomach acid (pH 1.5 to 3.5). [59]
2) pH-Responsive Polymers: These polymers envelop and shield insulin from acidic environments, releasing the insulin only in response to an elevation in pH, usually in the intestine. [60]
3) Gut microbiota: It consists of a large number of microorganisms that inhibit the gastrointestinal tract from contact with orally administered insulin [61] and cause problems with absorption and metabolism. Regulating it can affect absorption and metabolism. In addition to being essential for nutrient digestion and absorption, the gut microbiota may operate as a biochemical barrier to the administration of insulin orally. The interactions between oral insulin and gut microbiota add another layer of complexity to the already challenging task of delivering insulin orally. [62]
1. Degradation by Microbial Enzymes:
Microbial Enzymatic Activity: The gut microbiota secretes a range of enzymes, such as proteases, which can further break down insulin in the gastrointestinal system. It's possible that these microbiological enzymes will break down insulin into inert pieces before the bloodstream can absorb it, decreasing its potency. [63]
Competition for Nutrients: Any insulin or insulin-like peptides that are present in the gut lumen may be in competition with the microbiota for nutrients by the host. As a result, there may be less insulin available for absorption. [64]
Immune Modulation: Interaction with Immune Cells: The host's immune system is significantly influenced by the gut microbiota. Immune responses that either degrade. [65]
Strategies
Prebiotics and Probiotics: Modifying the gut microbiota composition with prebiotics or probiotics may help minimise the enzymatic breakdown of insulin or boost its absorption. [66]
Microbiota-Targeted Drug Delivery: Creation of oral insulin formulations that release insulin in areas of the gut with lower microbial activity or that circumvent areas of the gut where microbial degradation is highest. [67]
Combination Therapies: Insulin's bioavailability may be increased by taking it orally in conjunction with medications that alter the bacteria in the gut or shield it from microbial deterioration. [68]
Regulating it can affect absorption and metabolism. [70]
Table 1
|
Biochemical barrier |
Constituents |
To Overcome |
|
Enzymatic Degradation |
Carboxypeptidase, Trypsin, Chymotrypsin, Pepsin |
Hydrophobic effect |
|
Gastrointestinal pH |
pH 1.0-2.0 |
pH responsiveness |
|
Gut Microbiota |
Bacteria, virus, parasites |
Decrease bacteria in gut |
This table outlines major biochemical barriers affecting drug absorption and metabolism in the gastrointestinal tract. It lists key factors such as enzymatic degradation, acidic pH, and gut microbiota along with their constituents. Possible strategies to overcome these barriers, including hydrophobic protection and pH-responsive systems, are also highlighted.
Formulation barriers:
Fabrication methods for oral insulin formulations typically involve techniques such as nanoparticles, encapsulation, microencapsulation, polymer matrix systems, and mucoadhesive formulations. [71]
These methods aim to protect insulin from enzymatic degradation in the gastrointestinal tract, enhance absorption across the intestinal epithelium, and achieve controlled release kinetics to mimic the physiological characteristics of insulin secretion. [72]
For example, one manufacturing technique includes emulsification\solvent evaporation, nanoprecipitation, spray drying, and electrospinning. [73] [74]
Various nanocarriers have been explored for oral insulin delivery.
A. Polymer nanoparticles: They are typically made from biodegradable polymers such as poly (lactic-co-glycolic acid) (PLGA) or chitosan. They protect insulin from enzymatic degradation and facilitate its absorption. [75]
Chitosan: A common choice for insulin-loaded nanoparticles, chitosan is recognised for its mucoadhesive qualities and capacity to open tight connections. The biocompatible and biodegradable polymer known as poly (lactic-co-glycolic acid) (PLGA) is widely employed because of its capacity to efficiently encapsulate insulin and offer prolonged release. [76]
Alginate: Frequently utilised for its capacity to create hydrogels, alginate has the potential to shield insulin from the hostile GI environment and release it gradually. [77]
Benefits of Polymer Nanoparticles for Oral Insulin:
Protection from Degradation: Insulin is shielded from severe stomach conditions and enzymatic breakdown in the intestines by being encapsulated within polymer nanoparticles. [78]
Improved Bioavailability: By helping insulin pass through the intestinal epithelium, polymer nanoparticles can improve the absorption of the drug in the intestines. [79]
B. Lipid-based nanoparticles: Liposomes, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs) are examples. Lipid carrier provides a lipid environment that protects insulin and improves its absorption. [80]
Benefits of LNPs for Oral Insulin
Non-Invasive Administration: Patients are more likely to comply with oral delivery because it is more convenient and less unpleasant than injections.
Improved Stability and Bioavailability: LNPs increase insulin's stability and may improve the GI tract's capacity to absorb it.
Potential for Targeted Delivery: LNPs can be designed to release insulin in particular GI tract regions or in response to particular triggers. [81]
C. Polymer micelles: They are formed from amphiphilic block copolymers and can encapsulate insulin within their hydrophobic core, thereby improving its stability and solubility. The use of polymer micelles for oral insulin has the following benefits [82]
Improved Stability: Insulin is shielded from enzymatic breakdown and acidic GI tract conditions by being encapsulated in polymer micelles. [83]
Enhanced Bioavailability: Polymer micelles may potentially improve the bioavailability of insulin taken orally by encouraging improved absorption of insulin via the intestinal lining. [84]
Controlled and Targeted Release: Polymer micelles can be designed to release insulin in specific areas of the GI tract or in reaction to environmental cues (pH shifts, for example), improving the efficiency with which insulin enters the bloodstream. [85]
Non-Invasive Delivery: By utilising polymer micelles to administer insulin orally, injections may not be necessary, leading to increased patient comfort and compliance. [86]
D. Dendrimer: These are highly branched polymers with a well-defined structure. They can trap insulin molecules and protect them from degradation [87]
Following benefits of dendrimer:
High Encapsulation Efficiency: Dendrimers have the ability to encapsulate a significant amount of insulin, shielding it from degradation in the acidic stomach environment due to their branching structure and interior cavities. [88]
Controlled Release: The dendrimer structure allows for the regulation of insulin release, resulting in a prolonged release that resembles the body's normal secretion of the hormone. [89]
Targeted and Site-Specific Delivery: Insulin can be more effectively absorbed and released when dendrimers are designed to release it just in the small intestine. [90]
Versatility: Making the delivery system to individual therapeutic requirements is made possible by the capacity to alter the surface properties of dendrimers. [91]
E. Inorganic Nanoparticles: These are made from materials such as silica or gold have been investigated in oral insulin delivery because of their biocompatibility and controlled release. [92]
Benefits of Inorganic Nanoparticles for Oral Insulin:
High Stability: Under a variety of circumstances, inorganic nanoparticles—especially those based on silica and metals—are extremely stable, offering superior insulin protection. [93]
Surface Functionalisation: To enhance the stability, targeting, and release profile of insulin, the surface of inorganic nanoparticles can be readily changed with different ligands, targeting moieties, or polymers. [94]
Multifunctionality: Inorganic nanoparticles can be made to contain imaging agents in addition to insulin, enabling the monitoring of insulin administration and therapeutic response at the same time. [95]
Figure 9: Various nanoparticles of oral delivery insulin [96]
This figure illustrates different nanocarriers such as polymeric, lipid, metallic nanoparticles, micelles, nanogels, and quantum dots used for oral insulin delivery.
These systems protect insulin from degradation in the gastrointestinal tract. They also enhance insulin absorption and bioavailability.
Some clinical trials involving oral insulin
Many oral insulins have not entered clinical trials. One of the main reasons for this is that it is difficult to make measurements in the laboratory. [97]
However, some factors that will lead to success include optimizing the process, choosing the right equipment, creating a good design and sustainability of the product. [98]
In the Phase 1 trial, they will investigate the safety of oral insulin and strictly monitor the occurrence of hypoglycaemia in healthy and type 1 diabetic patients. After Phase 1, we will know if it is safe in humans and how it can be used instead of a vaccine in people with type 2 diabetes. New drugs can be prepared for clinical use. [99]
There are some pharmaceutical companies which are working on oral insulin delivery system are as follows: - [100]
Table 2
|
Company |
Name |
Product |
Action |
Clinical trials phase |
|
Nieldfree technologies (Hyderabad ) |
Oral insulin spray Ozulin |
Spraying insulin in mouth |
_ |
_ |
|
Biocon (a biotechnology company) Bangalore |
Oral insulin ‘IN-105’ |
Delivered in tablet form at room temperature |
_ |
I |
|
Jordanian Pharmaceutical Manufacturing Co PLC |
JPM Oral Insulin |
Liquid delivery system with insulin chitosan nanoparticles |
|
I |
|
Novo Nordisk A/S |
NN1952 OI338GT (NN1953) OI362GT (NN1954) OI287GT (NN1956) |
Insulin analogue with oral delivery system GIPET® |
Short |
I |
|
Oramed, Inc |
ORMD-0801 |
Insulin with protein oral delivery system POD™ |
Short |
II |
|
NOD Pharmaceuticals |
Nodlin |
Insulin with bio adhesive Nano encapsulation (NOD Tech) |
Intermediate
|
II |
This table summarizes oral insulin delivery technologies being developed by different pharmaceutical companies. It highlights the company name, product, delivery method/action, and the current clinical trial phase.
Overall, it shows ongoing efforts to replace injectable insulin with oral or spray-based formulations under early clinical evaluation.
FUTURE OUTLOOK
Further studies are needed to better understand the mechanisms involved in intestinal insulin absorption to improve oral efficacy.
CONCLUSION
Oral insulin delivery has great potential due to the need for a non-invasive route to improve compliance and pricing. Although there have been many efforts to develop oral insulin delivery systems, none have yet reached the market because they have not shown a clear advantage over conventional delivery and some are still in development.
REFERENCES


Apurva Chavan, MD Nawab, Review on Challenges and Innovations in Oral Insulin Administration, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1729-1756. https://doi.org/10.5281/zenodo.18280525
 10.5281/zenodo.18280525
10.5281/zenodo.18280525
