
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
2,3 Rajarambapu College of Pharmacy, Kasegaon,Walwa, Sangli, Maharashtra, India.
1,4,5 Sahyadri College of Pharmacy, Methwade, Sangola, Solapur, Maharashtra, India.
6 Fabtech College of Pharmacy, Sangola, Solapur, Maharashtra, India.
The mechanism of action (MOA) and effectiveness of vonoprazan, a potassium-competitive acid blocker (P-CAB), are very different from those of conventional proton pump inhibitors (PPIs) such as omeprazole and esomeprazole.Unlike PPIs, which require activation in an acidic environment and irreversibly inhibit the H?/K?-ATPase enzyme, Vonoprazan directly and reversibly blocks this enzyme without requiring prior activation. As a result, gastric acid secretion can be suppressed more rapidly , potently , and sustainably . Studies have shown that Vonoprazan achieves higher gastric pH levels more quickly & maintains them for a longer duration compared to PPIs, making it particularly effective for patients with severe acid-related disorders. Additionally, it is more stable in acidic conditions, providing consistent efficacy even in cases where PPIs may be less effective, such as Helicobacter pylori eradication or refractory gastro-esophageal reflux disease (GERD).
A condition affecting the digestive system, peptic-ulcer (gastro-duodenal ulcer) disease is characterized by gastric acid production and mucous membrane damage caused by pepsin.
Aetiology of Peptic-ulcer –
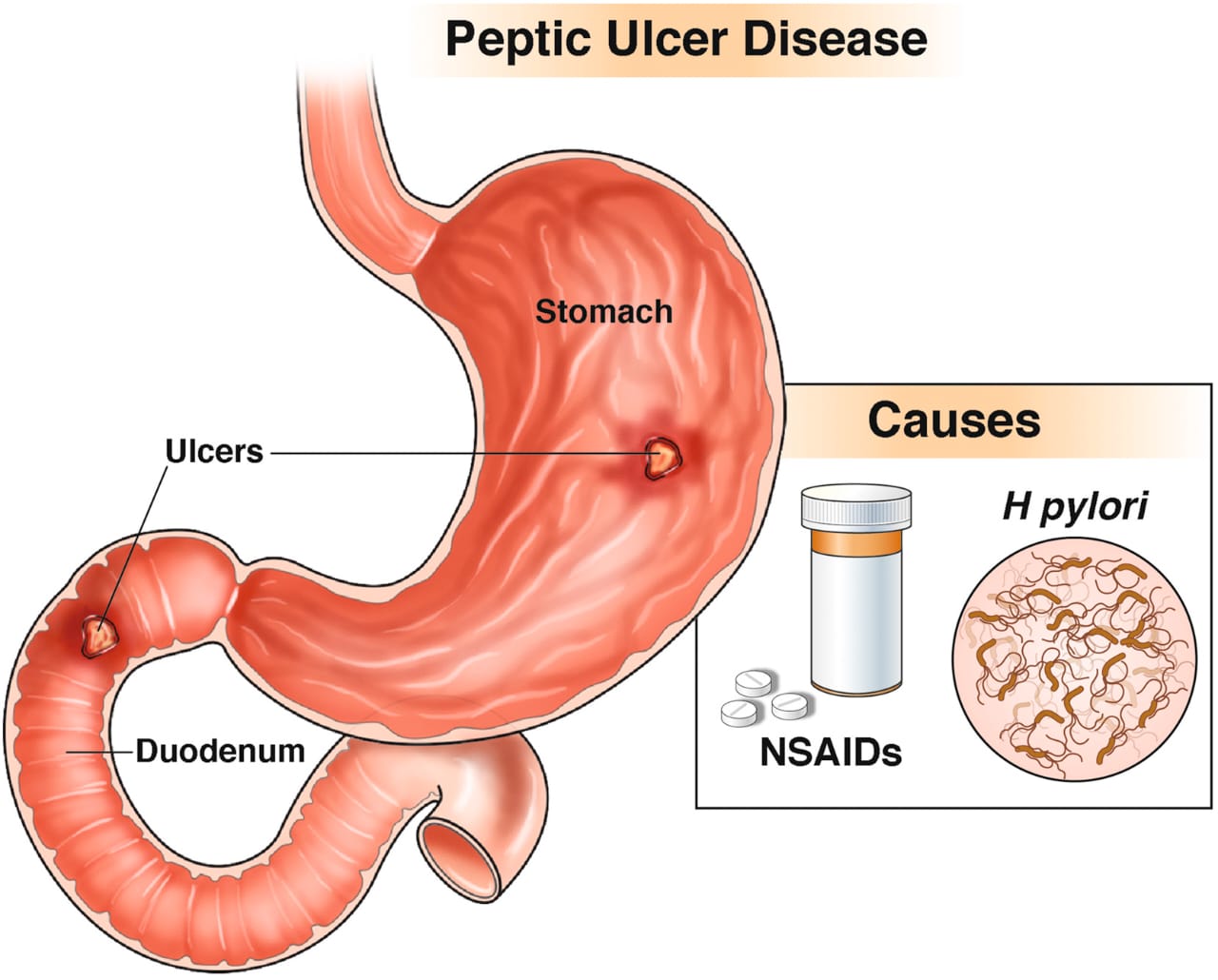
Fig. no. 1: Aetiology of Peptic-ulcer
Identification (diagnosis) of Peptic-ulcer Disease-
Symptoms and clinical features are usually considered , but individual signs and symptoms are not always reliable. A new selective and non-competitive Proton Pump Inhibitor (PPI’s) in the oxidative-reduction state, Vonoprazan is often referred to as a potassium-competitive acid blocker(P-CAB) [7].
Chemical structure of Vanoprazan -
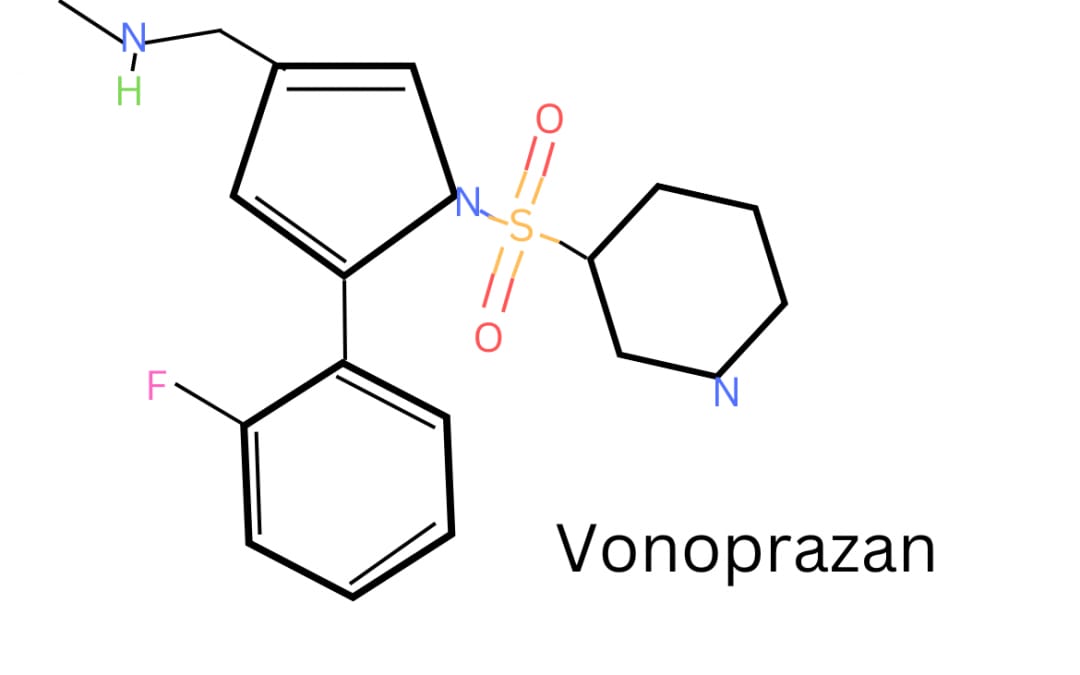
The cytochrome P450 (CYP) 3A4 is primarily responsible for the metabolism of Vonoprazan, with CYP2B6, CYP2C19, CYP2D6, &SULT2A1, which causes inactive metabolites to develop [8]. Vonoprazan offers a quicker onset of action, a longer duration of effect , a more
potent acid-suppressing capability compared to traditional proton pump inhibitors [9, 10]. Vonoprazan inhibits stomach acid in a dose-dependent manner and does so quickly, strongly, and persistently. The way PPI’s operate is by permanently blocking the stomach lining's proton pump (H+/K+-ATPase). Vonoprazan is likewise PPIs, however it works in a reversible way. PPI’s work by blocking this enzyme, which is in charge of the last stage of gastric acid production, so reducing the amount of acid secreted into the stomach. Unlike PPI’s, it binds to a different location on the proton pump to inhibit it.The time it takes for the body to replenish the deactivated proton pumps influences how long the suppression of acid with PPIs lasts. Because of its reversible inhibition, Vonoprazan may offer a longer and more sustained suppression of stomach acid compared to traditional PPIs, although this process might take several days. The recommended oral dosage of Vonoprazan is 20 milligrams once daily for treating gastro-duodenal ulcers, 20 milligrams once daily for reflux esophagitis, and 10 milligrams once daily for prevention. Additionally, it is prescribed at 10 milligrams once daily to prevent peptic ulcers caused by low doses of aspirin or non-steroidal anti-inflammatory drugs and 20 milligrams twice daily, when used in combination with Amoxicillin & Clarithromycin to eradicate H. pylori [11]. The stomach proton pump enzyme H+/K+-ATPase in parietal cells of the stomach is the target of the powerful acid-inhibitory medication Vonoprazan. Its slower dissociation kinetics give it a longer half-life than PPIs, and it doesn't need to be activated by stomach acid [12, 13]. The use of traditional PPIs has frequently been associated with acute-kidney injury (AKI) [14]. Chronic PPI use may result in nephrotoxicity [15]. Acute interstitial nephritis (AIN) is the key feature of PPI-induced acute kidney injury (AKI) [16]. Recent studies have shown that the treatment rates for gastro-esophageal reflux disease treatment and H. Pylori eradication are higher with Vonoprazan (VPZ) compared to traditional PPI therapy [17].
Mechanism of Action
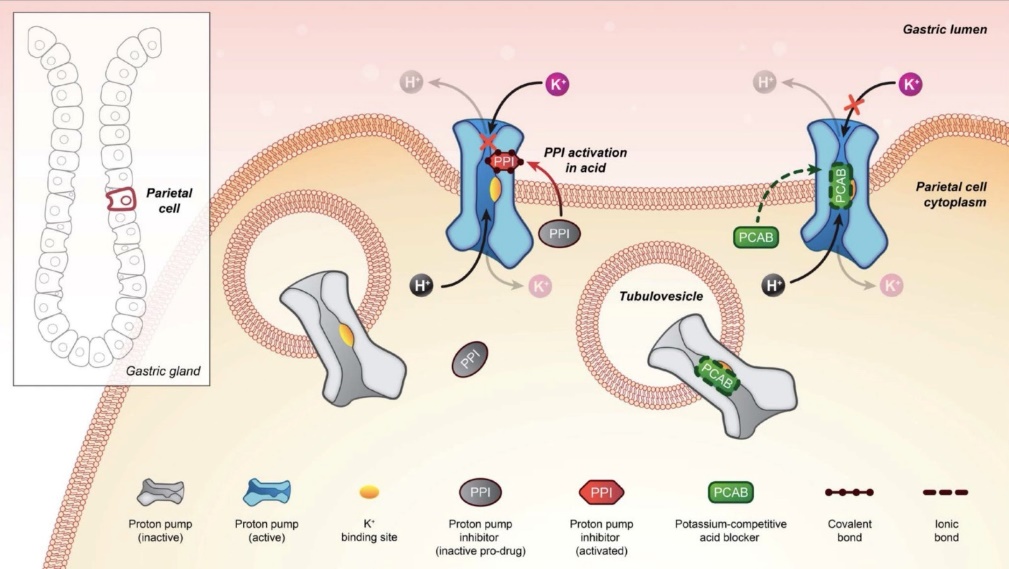
Fig.no. 3: Comparison in MOA of PPI and Vonoprazan.
When treating gastro-esophageal reflux disease, proton pump inhibitors (PPIs) can be used instead of potassium-competitive acid blockers (P-CABs), a special type of acid-suppressing drugs. PPIs may be used as an alternative to P-CABs in the treatment of GERD. Both PPIs and P-CABs are drug classes intended to reduce the production of stomach acid, and their use may be influenced by tolerability, patient preferences, or certain clinical concerns. In contrast to PPIs, P-CABs are a “distinct category of acid-suppressing medications" that work in a different way. P-CABs, like Vonoprazan, offer an alternate method of treating acid reflux by competitively blocking the proton pump's potassium channel suppression as opposed to PPI’s irreversible inhibition. P-CABs are acid-stable, non-covalent inhibitors of H+/K+-ATPase, in contrast to PPIs. Vonoprazan act as a potassium-competitive acid blocker (P-CAB), which inhibits the H+/K+-ATPase enzyme systems. The parietal cells of the stomach secrete acid both basal and stimulated and Vonoprazan inhibits both processes. The action's mechanism is shown in Fig. no.3. Although both medication classes block the H+/K+-ATPase, P-CABs operate differently than proton-pump inhibitors (PPIs). Although both drug groups block the H+/K+-ATPase, PCABs work differently than proton-pump PPIs, or inhibitors [18]. Lansoprazole (a conventional proton pump inhibitor) & Vonoprazan (potassium-competitive acid blocker) were compared in terms of their mechanisms of action. In the active phase of the secretory canaliculus, which follows a meal, H+/K+-ATPases can be seen on the apical membrane of the cells .They are observed in quiescent phage tubulovesicles. Lansoprazole dissolves rapidly, but in the secretory canaliculus ;it changes into its active form. The active form of lansoprazole forms covalent bond with the proton pump enzyme H+/ K+-ATPase. As shown in Fig. no.3 Vonoprazan can accumulate slowly in the acidic secretory canaliculus & effectively blocking newly exposed H+/K+-ATPase for an extended period. It binds to H+/K+-ATPase non-covalently & with slow dissociation rate [19].
Pharmacokinetic
Vonoprazan has time-independent pharmacokinetics. Vonoprazan is quickly absorbed after oral treatment, reaching peak plasma concentrations 1-3 hours after dosage. Clinical studies using once-daily dosage in healthy participants indicate that By days 3 and 4, vonoprazan exposure reaches steady-state values and is roughly dose proportional throughout dose range between 10 to 40 milligrams [20]. Food has no clinically significant impact on Vonoprazan pharmacokinetics & the medication can be taken as prescribed [21]. When Vonoprazan 20 milligrams is taken twice daily, the mean steady-state plasma exposure is nearly 1.8 times greater than on day 1. When taken twice a day at steady state, vonoprazan produces an apparent oral volume of distribution of 782.7 liters. Vonoprazan's plasma protein binding ranges between 85 and 88%. There is no pharmacologic activity in the metabolites that come from the extensive metabolism of Vonoprazan. According to in vitro research, CYP3A4 is the primary mediator of Vonoprazan metabolism, with sulfo- and glucuronosyl-transferases, CYP2B6, CYP2C9, CYP2C19, and CYP2D6 also playing a role [22]. The elimination half-life of Vonoprazan is around seven hours. When taking twice-daily doses, the apparent oral clearance at steady state is 81.3 L/h. About 67% and 31% of a radiolabeled dosage of Vonoprazan, respectively, were recovered in faeces and urine after oral delivery, primarily as metabolites. The pharmacokinetics of Vonoprazan did not differ clinically significantly by sex, age (less than 65 years versus more than 65 years), race (Asian versus non-Asian) or CYP2C19 metabolizer status [23].
Pharmacodynamics
The intragastric pH rises when Vonoprazan is used. With repeated daily dose, vonoprazan's inhibitory effect on acid secretion rises. Even while Vonoprazan's antisecretory action lessens after the medication is stopped, the intragastric pH stays high for 24 to 48 hours. QT prolongation is not clinically significantly affected by Vonoprazan. Vonoprazan has more significant point-positive charge ( pKa of 9.06 ) than other potassium-competitive acid blockers (PCABs). Because of this, Vonoprazan can build up at greater quantities in the stomach parietal cells canalicular region, where it binds H+/ K+-ATPase in a reversible & K+-competitive way. Vonoprazan exhibits more H+/K+-ATPase inhibitory activity than other PCABs like SCH28080 or proton-pump inhibitors like lansoprazole [24].
Drug-drug interaction
Clinical studies used combination regimens of Vonoprazan, clarithromycin, and amoxicillin to evaluate possible drug interactions. Exposure of results When clarithromycin and amoxicillin were given together, the amount of Vonoprazan eliminated rose by 1.8 times [25]. The PKs of amoxicillin remained same, while the exposure to the medication dose increased by 1.5 times when clarithromycin was administered using analytical methodologies with clinical trials & potential 290 triple therapy. Owing to possible safety issues with likely nitrosamine contaminants in clinical supply for rifampin, a Clinical studies investigating the impact of the potent CYP3A inducer rifampin on exposure to Vonoprazan were discontinued [26].
Adverse drug reaction
ADRs such rash, soft stools, nausea, diarrhea, and dysgeusia were frequently noted.
Drug-related immune system issues anaphylactic shock, urticaria, and eruptions.
Hepatobiliary diseases include jaundice, liver failure, and hepatic injury. The VOQUEZNA TRIPLE PAK, which includes[Vonoprazan pills + Amoxicillin capsules + Clarithromycin tablets] has typical side effects of vulvovaginal discomfort, altered taste sense (dysgeusia), and gastrointestinal problems like diarrhea [27].
Indication
Contraindication
The use of Vonoprazan is contraindicated in patients who are hypersensitive to it or its components . It should be used with caution in individuals with severe liver disease due to its hepatic metabolism. Pregnant and lactating women should avoid its use unless absolutely necessary, as safety data is limited. Long-term use may pose risks in patients prone to osteoporosis or infections like Clostridium difficile.
|
Contraindication |
Description |
|
Hypersensitivity |
Allergy to Vanoprazan or any of it’s components. |
|
Pregnancy and Lactation |
Not recommended due to lack of sufficient safety data. |
|
Severse Hepatic Impairment |
Patients with significant liver dysfuction may experience altered drug metabolism. |
|
Clostridium difficile Infection |
May increase the risk of bacterial overgrowth and diarrhea. |
|
Gastrointestinal Malignancy |
Can mask symptoms of stomach cancer, delaying diagnosis. |
Result
|
Feature |
Description |
|
Drug Name |
Vanoprazan |
|
Brand Name |
Lupivon, Voltapraz. |
|
Class |
Potassium-competitive acid blockers (PCAB) |
|
Mechanism of Action |
Vonoprazan is a potassium-competitive acid blocker (P-CAB) that inhibits H?/K?-ATPase in gastric parietal cells by competitively blocking K? binding. During the final step of gastric acid production , this prevents acid secretion. It provides potent, reversible, and long-lasting acid suppression, acting faster and more effectively than proton pump inhibitors (PPIs). |
|
Indication |
In adults suffering from erosive esophagitis & heartburn, this medication can help heal the condition. |
|
Administration |
Oral |
|
Approval Date |
November 2023 (USA) |
|
Manufacturer |
Sainor Laboratories. |
|
Adverse Effects |
Common: Diarrhea, constipation, nausea, abdominal pain, headache. Less Common: Elevated liver enzymes, rash, dizziness. Rare: Hypomagnesemia, increased risk of infections (e.g., Clostridium difficile), osteoporosis-related fractures (long-term use). |
|
Contraindications |
Hypersensitivity to vanoprazan or its components; severe liver disease; caution in pregnancy/lactation due to limited data. |
|
Pharmacokinetics
|
Absorption-Rapid Tmax-~2 hours Bioavailability: High Metabolism: Primarily hepatic (CYP3A4) Elimination Half-life: ~7 hours Excretion-Mainly fecal (~50%), some renal |
|
Pharmacodyanamics |
Provides longer-lasting and stronger acid suppression than PPIs; effective in both fasting and postprandial states. |
|
Drug Interactions |
May alter absorption of pH-dependent drugs (e.g. ketoconazole, atazanavir); interacts with CYP3A4 substrates (e.g., midazolam, tacrolimus). |
CONCLUSION
Vonoprazan, a next-generation potassium-competitive acid blocker (P-CAB), signifies a paradigm shift in the therapeutic approach to acid-related pathologies, including peptic ulcer disease and gastro-esophageal reflux disorder (GERD). In contrast to conventional proton pump inhibitors (PPIs), which necessitate prior activation and exert irreversible inhibition on gastric H?/K?-ATPase, Vonoprazan functions through direct, reversible, and more potent suppression of gastric acid secretion. Comparative investigations have elucidated its superior pharmaco-dynamic profile, demonstrating enhanced acid suppression kinetics, prolonged elevation of intragastric pH, and greater efficacy in refractory GERD and Helicobacter pylori eradication regimens. Moreover, its intrinsic stability under acidic conditions mitigates interindividual variability in therapeutic outcomes, a limitation frequently associated with PPIs. Although PPIs maintain their prominence due to extensive clinical validation and long-term safety data, Vonoprazan emerges as a formidable alternative, particularly for patients necessitating sustained and robust acid inhibition. Nonetheless, further longitudinal studies are warranted to comprehensively ascertain its long-term safety and optimize its clinical utility in acid-related disorders
REFERENCES





Shantanu Bele, Shaunak Bele, Aarati Sawanji, Vaibhav Khadul*, Mayur Pawar, Akshay Khatal, Review on: Comparative study of Proton pump inhibitors & Vonoprazan with respect to Anti-ulcer activity, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1134-1141. https://doi.org/10.5281/zenodo.15185106
 10.5281/zenodo.15185106
10.5281/zenodo.15185106