
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of Pharmacy, Sharda University, Knowledge Park –III, Greater Noida.
Uterine fibroids, also known as leiomyoma’s or myomas, are the most common benign tumour in women. They often lead to various clinical issues such as heavy menstrual bleeding, anaemia, painful menstruation (dysmenorrhea), chronic pelvic discomfort, difficulty in pregnancy, and urinary symptoms. The enhancement of these fibroids is influenced by a complex interaction of hormonal, genetic, and environmental factors. A key factor in their growth is the regulation of steroid hormones—particularly estrogen and progesterone. Estrogen is known to encourage the growth of fibroids, while progesterone has a more nuanced role, sometimes promoting or inhibiting fibroid growth depending on the uterine environment. Understanding how these hormones impact fibroid development is vital for creating effective treatments, as current therapies often aim to modulate hormone levels to alleviate symptoms and shrink the fibroids. The effects of steroid hormones on uterine fibroids primarily occur through their binding to steroid receptors in the uterine smooth muscle cells. Both estrogen and progesterone receptors are found in high concentrations in fibroid tissues, underscoring the importance of these hormones in fibroid growth. Estrogen promotes the proliferation of smooth muscle cells, enhances the production of extracellular matrix components, and increases angiogenesis (blood vessel formation) within fibroids. This hormone contributes to fibroid pathogenesis by triggering cellular activities that support tumor expansion. Additionally, research indicates that estrogen alters the interpretation of various growth factors and cytokines in fibroid tissue, further aiding the fibrotic process. Progesterone, through its receptor, also plays a role in fibroid development, though its effects are more context-dependent. Under typical conditions, progesterone may help balance fibroid growth and regression. However, when the hormonal balance is disrupted—such as during periods of excess estrogen or impaired progesterone function—fibroids can continue to grow. The interplay between estrogen and progesterone is crucial in determining whether fibroids expand or shrink. Disruptions in the balance of these hormones, as seen in conditions like obesity or menopause, may also contribute to the formation and progression of fibroids. Recent advances in the molecular understanding of uterine fibroids have highlighted the critical role of steroid hormone receptors and their signaling pathways in fibroid development. For instance, overexpression of the estrogen receptor alpha (ER?) has been identical with increased fibroid growth, while the two isoforms of the progesterone receptor (PR-A and PR-B) have distinct effects on how cells respond to progesterone. Moreover, steroid hormone receptors help regulate the expression of genes responsible for extracellular matrix remodelling and cell proliferation—two key factors in fibroid formation. The discovery of these molecular pathways has led to the development of targeted therapies that aim to modulate steroid hormone signalling in fibroid tissues. Steroid regulation is also influenced by various co-regulators and enzymes that alter local concentrations of estrogen and progesterone. Aromatase, an enzyme that converts androgens to estrogen, has been found at higher levels in fibroid tissues. This suggests that local estrogen production within the fibroid environment may be a contributing factor to its growth. Additionally, 17?-hydroxysteroid dehydrogenase (17?-HSD), which regulates the availability of active estrogen, is involved in fibroid development. These enzymes represent promising therapeutic targets for controlling the local steroid hormone levels within fibroid tissues, offering new avenues for managing fibroid growth and associated symptoms.
Historical Background
Uterine fibroids were originally called Uterine stones and then Scleromas in the second century AD. The term fibroid was introduced in 1860s. The first documented myomectomy was performed in 1845 by Dr. Washington Atlee in Pennsylvania. German pathologist Rudolf Virchow coined the term myomas to describe the smooth muscle origin of fibroids. It was originally thought that fibroids grew linearly during a woman’s reproductive years, but evidence suggests that they may grow and regress.
What is Fibroids?
Fibroids also known as leiomyomas, are non-cancerous growths that develop in or around the uterus. They are composed of smooth muscle cells and fibrous connective tissue. Uterine fibroids, also known as leiomyoma, are the most common benign tumors of the female reproductive system, affecting a substantial proportion of women, particularly those of reproductive age. Estimates suggest that up to 70-80% of women may develop fibroids at some point in their lives, with around 25% experiencing symptoms severe enough to necessitate medical intervention. The clinical manifestations of fibroids can include heavy menstrual bleeding, pelvic pain, pressure symptoms, and complications related to pregnancy and infertility. Given their prevalence and associated health burdens, understanding the pathophysiology of uterine fibroids is crucial for developing effective treatment strategies.
Symptoms-
Risk Factors -
Category Of Uterine Fibroids-
1. Intramural Fibroids-
- Location: Within the uterine wall
- Characteristics: Most common type, can grow large, may cause heavy bleeding and pressure
- Symptoms: Pelvic pain, heavy bleeding, pressure on bladder/bowels.
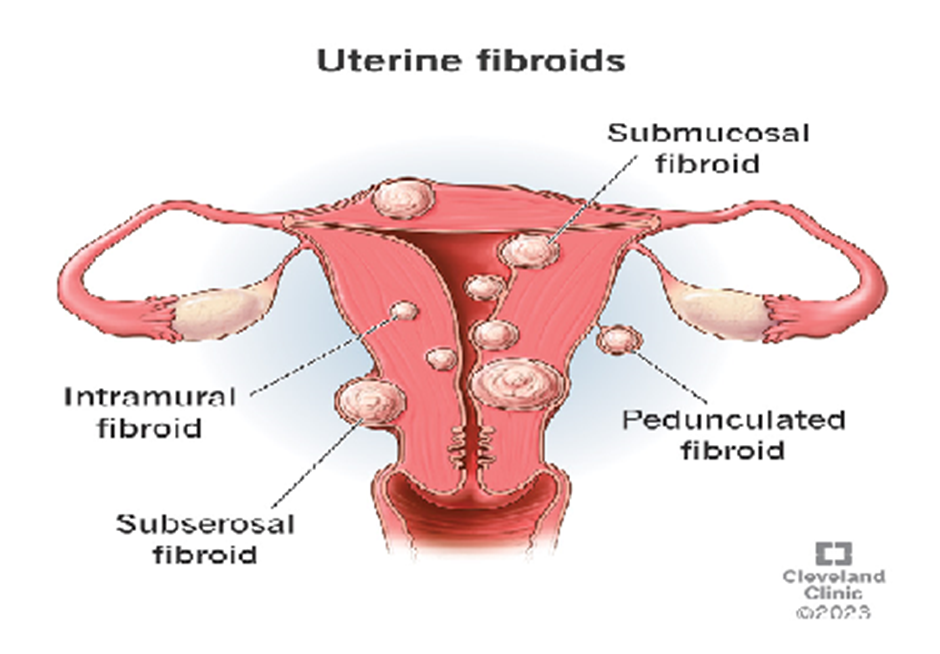
https://my.clevelandclinic.org/health/diseases/9130-uterine-fibroids
2. Submucosal Fibroids-
- Location: Under the uterine lining (endometrium)
- Characteristics: Grow into the uterine cavity, can cause heavy bleeding and infertility
- Symptoms: Heavy bleeding, prolonged periods, infertility, miscarriage
3. Subserosal Fibroids-
- Location: On the exterior surface of the uterus
- Characteristics: Can grow large, may cause pressure on surrounding organs
- Symptoms: Pelvic pressure, bladder/bowel pressure, back pain
4. Pedunculated Fibroids-
- Location: Attached to the uterus by a stalk (peduncle)
- Characteristics: Can grow inside or outside the uterus
- Symptoms: Pelvic pain, heavy bleeding, pressure on surrounding organs
Other Types:
1. Cervical Fibroids: Grow in the cervix
2. Parasitic Fibroids: Grow outside the uterus, attached to nearby organs
3. Intraligamentous Fibroids: Raise within the ligaments supporting the uterus
4. Adenomyotic Fibroids: Raise within the uterine muscle, often with endometriosis
Classification by Size:
1. Small Fibroids: <2 cm
2. Medium Fibroids: 2-5 cm
3. Large Fibroids: >5 cm
Mechanism:
•The precise molecular mechanism behind the formation of fibroids remains unclear. However, it is believed that local hypoxia and hormonal influences are key factors that initiate the transformation of myometrial cells or their stem progenitors into fibroid cells. The concentration of these hormones fluctuates significantly across different phases of the estrous cycle.
•It is well-established that the development and growth of fibroids are influenced by sex steroids such as estrogen and progesterone, along with pituitary hormones, including gonadotropins, follicle-stimulating hormone (FSH), luteinizing hormone (LH), anti-Müllerian hormone, and prolactin.
•Additionally, the individual genetic makeup of the patient (hereditary factors), ethnic background, and a high body mass index (BMI) also play significant roles in the occurrence of fibroids.
•Steroid hormones bind to their respective receptors, activating signalling pathways that promote the proliferation of fibroid cells.
•Genes regulated by these hormones control key procedures such as cell proliferation, distinct, and survival within fibroids.
•Inflammation and oxidative stress contribute to the development and progression of fibroids.
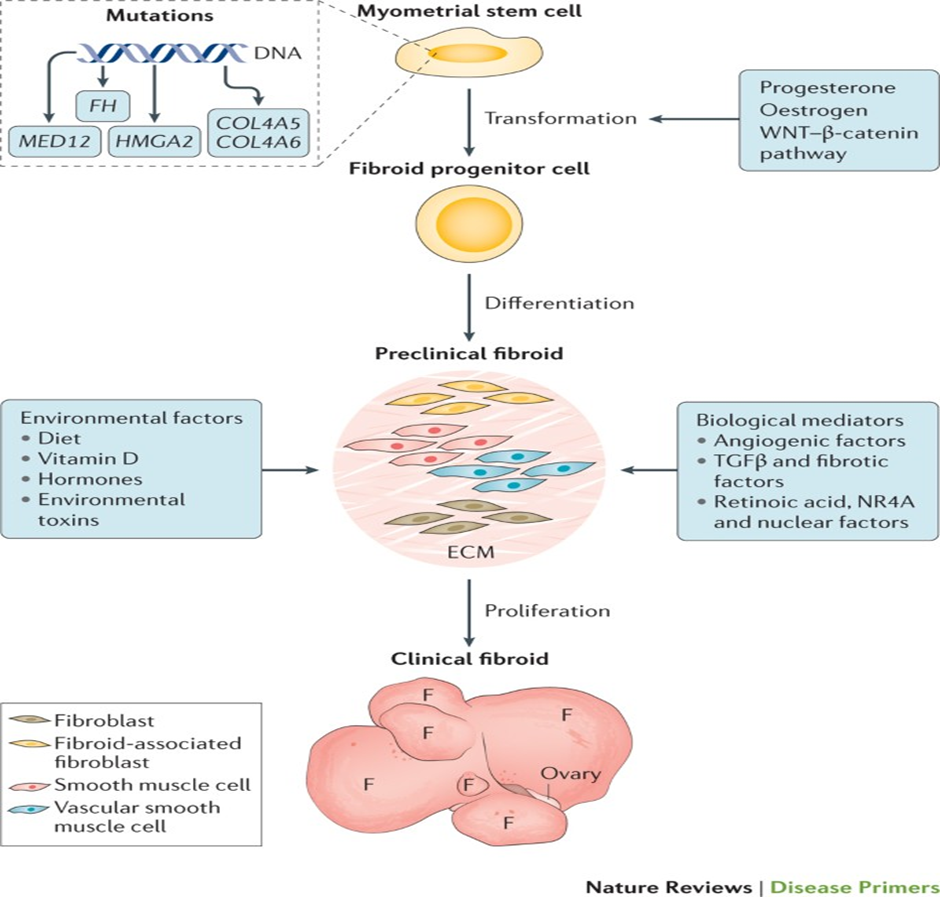
https://www.nature.com/articles/nrdp201643
Mechanism of Uterine Fibroid Formation:
Receptors Involved:
Pathways Involved:
Phases of Fibroid Growth:
Factors Affecting Fibroid Development:
METHODOLOGY:
To understand the portrayal of steroid hormones in the enhancement of uterine fibroids, a multidisciplinary approach that combines clinical observations, molecular biology research, and pharmacological studies is essential. This methodology outlines a systematic approach for examining the effects of steroid hormones, primarily estrogen and progesterone, on the growth and regulation of uterine fibroids.
Study Design:
To address the research questions regarding the influence of steroids on fibroid development, a combination of observational studies, in-vitro experiments, and animal models will be used. This triangulated approach ensures a well-rounded understanding of the mechanisms driving fibroid growth.
A comprehensive review of existing literature will be conducted to compile the current knowledge about the relation between steroid hormones and uterine fibroids. This will include:
This literature review will establish a solid foundation for evaluating new findings and help identify gaps in existing knowledge.
Sample Selection:
Data Collection:
Symptom Assessment:
Statistical Analysis:
To explore the cellular mechanisms by which steroids influence fibroid development, well-established human leiomyoma cell lines will be used.
Cell Culture:
Outcome Measures:
In vivo studies will use an ovariectomized mouse model to simulate the hormonal regulation of fibroids.
Experimental Design:
Histological Analysis:
Body of the Review: The Role of Steroids in the Development of Uterine Fibroids
Uterine fibroids, also known as leiomyoma, are non-cancerous tumor that enhance from the smooth muscle layer of the uterus. They are highly prevalent and clinically significant, affecting a large portion of women during their reproductive years. The development of fibroids involves intricate interactions among genetic, environmental, and hormonal factors, with steroid hormones—especially estrogen and progesterone—playing a key aspect in their growth and regulation.
Estrogen’s Impact on Fibroid Development
Estrogen significantly influences the growth and formation of uterine fibroids. Multiple studies have shown that fibroids have elevated levels of estrogen receptors compared to normal myometrial tissues, indicating that estrogen levels are directly associated with fibroid growth. In premenopausal women, the fluctuations of estrogen during the menstrual cycle can worsen fibroid symptoms, as fibroids are predominantly estrogen-dependent. Estrogen stimulates cell proliferation and the production of extracellular matrix components, which creates a favorable environment for fibroid expansion. Research further supports the notion that fibroid tissues react to estrogen by promoting cellular proliferation and angiogenesis. For example, estrogen boosts the interpretation of growth factors like insulin-like growth factor-1 (IGF-1), which is essential for stimulating the mitogenic activity in myometrial cells. This creates assessment loop in which fibroids contribute to local estrogen production, thereby accelerating their own growth.
The Role of Progesterone
Progesterone also opera crucial role in the enhancement of fibroids, particularly through its receptors found within fibroid tissues. Studies show that progesterone can trigger the expression of genes linked to cell proliferation and encourage fibroblast activity in the myometrium. The interaction between estrogen and progesterone is synergistic; while estrogen initiates fibroid growth, progesterone supports their structural development and further expansion. Selective progesterone receptor modulators (SPRMs), like ulipristal acetate, have proven effective in treating uterine fibroids by reducing progesterone's effects, which edge to a contraction in fibroid size and alleviation of ailment. This highlights progesterone's dual function as both a growth-promoting factor and a viable therapeutic target.
Interactions with Other Steroid Hormones
Although estrogen and progesterone are the main hormones involved in fibroid regulation, other steroid hormones such as androgens and glucocorticoids may also affect fibroid development. Androgens can be converted to estrogen in adipose tissue, thereby influencing local estrogen levels and impacting the fibroid environment. Likewise, glucocorticoids are believed to influence the inflammatory response in the uterus, which could indirectly affect fibroid progression. Importantly, research has shown that steroid hormones interact with various molecular passageways, such as the Wnt/β-catenin and RhoA signalling pathways, which can significantly influence fibroid biology. Abnormal activation of these pathways has been linked to increased cell proliferation and extracellular matrix production, further promoting fibroid development.
Epigenetic and Molecular Mechanisms
Emerging research suggests that steroid hormones may also contribute to epigenetic modifications, complicating the understanding of fibroid development. Adjustment in DNA methylation and histone alteration patterns in response to steroid hormones could alter gene expression profiles in myometrial tissues. These epigenetic alterations likely opera a role in the long-term aftermath of steroid hormones on fibroid growth and behaviour. In conclusion, the formation of uterine fibroids is closely associated with the regulation of steroid hormones, especially estrogen and progesterone. Their influence on cell proliferation, gene expression, and interactions with growth factors creates a complex environment that supports fibroid development. Ongoing research into these hormonal pathways is crucial for identifying new therapeutic strategies that target steroid regulation, offering potential for better management of uterine fibroids and enhanced quality of life for affected women. As our understanding of these biological mechanisms continues to evolve, it is clear that effective treatments must consider the intricate interplay of hormonal influences in fibroid pathophysiology.
Discussion: Uterine fibroids, or leiomyoma, are a common health condition that affects a significant proportion of women, particularly during their reproductive years. A comprehensive understanding of the role that steroid hormones—especially estrogen and progesterone—play in the enhancement of these fibroids is essential for advancing treatment strategies and improving patient outcomes.
Overview of Steroid Hormone Regulation: Steroid hormones such as estrogen and progesterone are vital regulators of the menstrual cycle, reproductive health, and metabolism. Their production and biological effects are carefully controlled, and any fluctuations can lead to various physiological changes. In the case of uterine fibroids, both estrogen and progesterone have been shown to stimulate cell growth and extracellular matrix (ECM) production in the uterus, creating a favorable environment for fibroid development. Fibroids are particularly known for their estrogen dependence. Estrogen promotes the growth of smooth muscle cells in the myometrium and stimulates the production of various growth factors. The increased expression of estrogen receptors in fibroid tissues offers insight into why these tumor’s are often sensitive to hormonal fluctuations that ensue all along the menstrual cycle. For many women, symptoms related to fibroids become more pronounced all along the follicular and luteal phases of the cycle, when estrogen and progesterone levels are higher.
The Synergistic Effect of Estrogen and Progesterone- The relationship between estrogen and progesterone in fibroid development is complex and highly interactive. While estrogen acts as the main trigger for cell division, progesterone further enhances the growth-promoting effects initiated by estrogen. This interaction has therapeutic implications. For example, scrupulous progesterone receptor modulators (SPRMs), like ulipristal acetate, have shown effectiveness in reducing fibroid size by blocking the actions of progesterone. This highlights the importance of hormonal balance and suggests that targeting these pathways may offer potential treatment strategies. Moreover, the timing of hormone exposure plays a critical role. Research has demonstrated that prolonged exposure to elevated levels of estrogen or progesterone increases the risk of fibroid development. This is particularly evident in cases of obesity, where increased adipose tissue results in higher estrogen levels due to the transformation of androgens to estrogens. Recognizing these interrelations emphasizes the need to appraise a woman’s overall hormonal profile when determining fibroid risk.
Contributions of Additional Steroid Hormones-While estrogen and progesterone are the primary hormones convoluted in fibroid growth, other steroid hormones also play significant roles. Androgens, although less influential than estrogen, may affect fibroid development by being converted into estrogen in adipose tissue. Additionally, glucocorticoids deserve attention for their role in modulating the inflammatory response, which could indirectly influence fibroid growth. The interaction between various steroid hormones points to a more systemic involvement in fibroid pathogenesis, underscoring the need for a multifaceted approach to treatment.
Molecular and Epigenetic Mechanisms: Recent research has focused on the molecular and epigenetic mechanisms by which steroid hormones regulate fibroid development. Specific signalling pathways, such as Wnt/β-catenin, have been linked to increased cell proliferation and differentiation within fibroids. Furthermore, steroid hormone vulnerability can urge epigenetic changes, such as DNA methylation and histone modifications, which can amend gene expression patterns and potentially increase the risk of fibroid formation. This intersection of hormonal signalling and epigenetics presents a promising area for further research and could reveal new targets for therapeutic intervention.
Clinical Implications and Future Directions
The Considerate of steroid hormone coordination in the development of uterine fibroids carries several important clinical implications. The success of SPRMs has sparked increased interest in developing treatments that target hormonal pathways more precisely, while minimizing the after effects commonly associated amidst systemic hormone remedies. Moreover, advancing our understanding of how hormones interact with one another could lead to more personalized treatment plans tailored to the unique hormonal profiles of women with fibroids. Looking ahead, future research should not only focus on the hormonal mechanisms underlying fibroid development but also consider the environmental factors that interact with these biological systems. Lifestyle factors such as diet, physical activity, and stress may also influence hormonal levels, thereby contributing to fibroid growth. Exploring these factors further could offer new insights into preventing and treating uterine fibroids more effectively.
Future Directions
Looking ahead, gaining a deeper understanding of steroid hormone signaling in relation to uterine fibroid development is crucial. Future research should prioritize longitudinal studies to clarify the interactions between hormonal pathways, growth factors, and environmental influences on fibroid development and progression. Incorporating genetic and epigenetic data will offer further insights into the biology of myomas, potentially enabling more personalized treatment approaches entrenched the patient's hormonal portrait and the specific characteristics of their fibroids. In conclusion, the complex mechanisms involved in the pathogenesis of uterine fibroids require a holistic approach, with hormonal regulation being a central factor. Ongoing research into the delicate balance of steroid hormones and their interactions with other molecular pathways is essential for advancing clinical management and improving therapeutic outcomes for women affected by this widespread condition. By addressing the role of steroid hormones in fibroid development, we can enhance our understanding of this common gynaecological issue, potentially leading to more effective and less invasive treatment options in the future.
Medication-
Some medications commonly used to treat uterine fibroids:
Hormonal Therapies:
1. Gonadotropin-releasing hormone (GnRH) agonists:
- Leuprolide (Lupron)
- Nafarelin (Synarel)
- Goserelin (Zoladex)
2. Selective estrogen receptor modulators (SERMs):
- Raloxifene (Evista)
- Tamoxifen (Nolvadex)
3. Progesterone receptor modulators:
- Ulipristal acetate (Ella)
- Mifepristone (Mifeprex)
Non-Hormonal Therapies:
1. Pain relievers:
- Ibuprofen (Advil, Motrin)
- Naproxen (Aleve)
2. Anti-inflammatory medications:
- Celecoxib (Celebrex)
3. Tranquilizers:
- Clonidine (Catapres)
Uterine Fibroid-Specific Medications:
1. Tranexamic acid (Lysteda): reduces heavy bleeding
2. Levonorgestrel-releasing intrauterine system (Mirena): reduces bleeding and shrink’s fibroids
3. Elagolix (Orilissa): reduces heavy bleeding and shrink’s fibroids
Emerging Therapies:
1. Aromatase inhibitors: reduce estrogen production
2. Anti-vascular endothelial growth factor (VEGF) therapies: reduce fibroid growth
3. Selective progesterone receptor antagonists: shrink fibroids
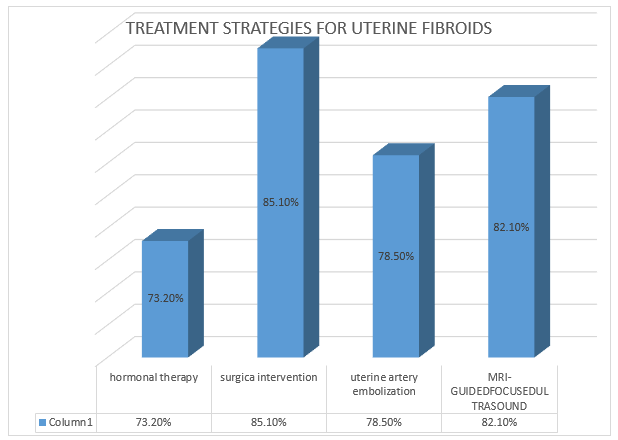
Surgical and Minimally Invasive Options:
1. Myomectomy (fibroid removal)
2. Hysterectomy (uterus removal)
3. Endometrial ablation
4. Uterine artery embolization (UAE)
5. Magnetic resonance-guided focused ultrasound surgery (MRgFUS)
Diagnosis
Management-
Yearly Medication Outcomes and Adverse Events
|
Reporting Year |
Therapeutic Agent |
% of people affected |
% of treated people successfully |
Medication related adverse events |
|
2019 |
Ulipristal Acetate |
15-20% |
50-75% |
Effective for reducing symptoms pre- surgery , but some related liver ADRs. |
|
2020 |
Leuprolide Acetate (GnRH Agonist) |
20-30% |
30-60% |
Reduces fibroid size significantly: Common ADRs include hot flashes and bone density loss. |
|
2021 |
Mifepristone |
10-20% |
50% |
Used for symptom relief: GIT issues reported in some patients. |
|
2022 |
Tranexamic acid |
25-30% |
40% |
Helps reduce heavy menstrual bleeding but not focussed on fibroid size reduction. |
|
2023 |
Aromatase Inhibitors |
10-20% |
30-50% |
Emergency treatment: some data on effectiveness, but still under research. |
Adverse Drug Reaction (ADRs) Surveillance Report –
|
Reporting Year |
Therapeutic Agent |
ADRs incidence |
% of people affected |
|
1994 |
RU486 (Mifepristone) |
Nausea, Headache, Fatigue, Uterine bleeding |
8-10% |
|
2004 |
Mifepristone |
Headache, nausea, Uterine cramping |
10-15% |
|
2006 |
Low-Dose Mifepristone |
Amenorrhea, Nausea, Fatigue |
20-22% |
|
2009 |
Leuprolide acetate (GnRH agonist) |
Hot flashes, Bone density loss, Mood swings |
20-30% |
|
2012 |
Ulipristal acetate |
Menstrual irregularities, Headache |
15-20% |
|
2016 |
Mifepristone |
GIT Issues, Dizziness |
14-16% |
Prevalence of Uterine Fibroids Due To Steroid Regulation & Treatment Success Rate (Last 10 Years)

CONCLUSION AND SUMMARY-
In conclusion, uterine fibroids are the result of a complex interaction of various factors, with steroid hormones, primarily estrogen and progesterone, playing a key aspect in their development. These hormones stimulate cell proliferation and affect the uterine extracellular environment, driving fibroid growth. Gaining a deeper understanding of the delicate balance and interaction between these hormones provides critical insights into the underlying pathophysiology of uterine fibroids. The synergistic effect between estrogen and progesterone offers significant therapeutic opportunities, as demonstrated by the success of scrupulous progesterone receptor modulators (SPRM) in treating fibroids. The exploration of additional steroid hormones, along with emerging discoveries related to molecular and epigenetic mechanisms, holds promise for advancing fibroid research. This area of study is crucial for the advancement of new remedial approach that not only target hormonal pathways but also address the multifaceted nature of fibroid development. Ongoing research efforts remain crucial for furthering our understanding of how steroid hormones regulate uterine fibroid formation, ultimately leading to innovative treatments that can enhance the quality of life for women afflicted by this widespread condition. A focus on personalized medicine, along with consideration of lifestyle factors in conjunction with hormonal therapies, offers promising prospects for better managing uterine fibroids and enhancing reproductive health.
Understanding the Hormonal Influence on Fibroid Development
Steroid hormones, particularly estrogen and progesterone, play essential roles in the growth, formation, and persistence of uterine fibroids. Studies have shown that fibroids exhibit a high density of estrogen and progesterone receptors, making them highly responsive to these hormones. Estrogen, primarily produced by ovarian follicles and adipose tissue, stimulates the proliferation of smooth muscle cells, the dominant cell type in fibroids. Estrogen acts through two main receptors, ERα and ERβ, which regulate gene expression and promote cell growth. This hormonal activity not only leads to the hyperplasia of myometrial cells but also alters the extracellular matrix (ECM) composition, contributing to the fibrotic characteristics of fibroids. Progesterone plays a complementary role by regulating apoptosis in uterine smooth muscle cells and influencing ECM dynamics through various growth factors. The interaction between estrogen and progesterone creates a delicate hormonal balance: while estrogen promotes the proliferation and growth of fibroids, progesterone may either enhance or inhibit growth depending on hormonal levels and receptor interactions. This complex relationship highlights the central role of steroid hormones in the pathophysiology of uterine fibroids.
Aspects of Other Factors in Hormonal Regulation
While steroid hormones are crucial, other factors also influence fibroid regulation. Advancement component, such as transforming growth factor-beta (TGF-β) and insulin-like growth factors (IGFs), serve as mediators of hormone action and play roles in fibroid development. Additionally, increased interpretation of vascular endothelial growth factor (VEGF) in fibroid tissue underscores the importance of angiogenesis in fibroid growth. Angiogenic factors, in combination with steroid hormones, contribute not only to fibroid development but may also represent new targets for treatment. Furthermore, the role of other regulatory molecules, such as microRNAs and cytokines, in fibroid pathology is gaining attention. Disruptions in these regulatory components can either amplify or reduce the effects of steroid hormones on fibroid development. For example, dysregulation of angiogenic pathways or an increase in inflammatory mediators may lead to more aggressive fibroid growth.
Clinical Implications and Therapeutic Targets
A deeper understanding of steroid hormone regulation in fibroid development offers new possibilities for treatment. Current therapies aim to alleviate symptoms and reduce fibroid size, with a primary focus on medical treatments such as gonadotropin-releasing hormone agonists, which temporarily shrivel fibroids inducing a hypo estrogenic state, are the primary treatments. However, the long-term use of these drugs is often limited by their side effects, highlighting the need for alternative treatments. Recent research has suggested that scrupulous estrogen receptor modulators (SERMs) and scrupulous progesterone receptor modulators (SPERMs) may offer more targeted hormonal therapy for uterine fibroids, providing symptom relief with fewer adverse effects. Additionally, vitamin D has shown potential as a treatment option, due to its role in regulating cellular proliferation and apoptosis, which may offer protective benefits against fibroid development. Exploring innovative therapies, such as focused ultrasound surgery and magnetic resonance-guided focused ultrasound, could also improve treatment outcomes. These non-invasive procedures target fibroids precisely while preserving surrounding healthy tissue, thus reducing the need for more invasive surgeries like hysterectomy or myomectomy.
REFERENCES

Dr. Gunjan*, Muskan Kumari, Dr. Preeti Singh, Role of Steroids Regulation In Development of Uterine Fibroids, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 76-93 https://doi.org/10.5281/zenodo.15118846
 10.5281/zenodo.15118846
10.5281/zenodo.15118846