IPS Academy College of Pharmacy, Rajendra Nagar, A.B. Road, Indore, Madhya Pradesh, India 452012
The global health burden of diabetes mellitus remains high, and fresh approaches are?required beyond traditional medical management. Artificial intelligence (AI) has recently become a groundbreaking catalyst with great potential for revolutionizing?all aspects of diabetes care, from forecasting and diagnosis to personalized therapy and risk prevention. This review discusses the use of machine learning, deep learning?and algorithms derived from data analysis for the development of diabetes prediction, screening and continuous glucose monitoring. AI-enhanced methods for early identification of high-risk patients, management of insulin dosage and nutritional planning based on an individual’s?dietary and physical activity patterns using adaptive digital platforms are also developed. Further, smart systems integrated with wearable biosensors and telemedicine applications have enabled patient-centric as well as remote and?continuous management. The article also points out AI’s?increasingly prominent application in automatic dietary monitoring, health education as well as early detection of diabetic complications including retinopathy and nephropathy. Although progress has been made in all of these areas, concerns including privacy, suboptimal-digital-literacy, algorithmic?bias and regulatory barriers are some of the obstacles to widespread clinical implementation. Looking forward AI will be integrated with the Internet of Medical?Things, generative and language models and precision-medicine frameworks to deliver safer, more equitable and effective diabetes care. Overall, AI represents a pivotal innovation that promises to shift diabetes management toward a predictive, preventive, and personalized healthcare paradigm.
1.1 Artificial Intelligence
People made machines already exist that can perform all type laborious work. However, for many reasons, both due to the pressures of needing more “production” and perhaps in some cases of interest, humans have been attempting to imbue machines with human like intelligence (which is the original motivation behind AI). Artificial Intelligence has been explored for over six decades, and both its theoretical advances and real-world applications show that the current momentum surrounding AI is durable and not disappearing anytime soon [1,2]. AI is applied in almost all aspects of life and is deemed as a fundamental competency in the future. The AI market will be worth $190 billion by 2025 and is expected to register an impressive CAGR (compound annual growth rate) of over 36% from 2018-2025 [3].
Artificial intelligence has been defined in many different ways. According to the turing test, a machine can be called intelligent if it can communicate with a person through electronic means without revealing that it is not human [4,5]. Marvin Minsky, a key pioneer in the field, described AI as creating machines that can perform tasks that would be considered intelligent if done by humans [6,7]. The symbolic approach to AI says that intelligence comes from processing symbols, with these symbols representing real-world objects. Although the explanations vary, AI mainly focuses on the ideas, methods, technologies, and real-world applications that help imitate, enhance, or expand human intelligence.
Today, AI is changing our lives in some of the most significant ways ever seen in history. Just as steam engines powered the industrial age, electricity transformed the modern world, and computers shaped the information Age, AI is becoming the next major technology driving our future. It is quickly becoming a core part of economies and daily life. The term “AI” is now used everywhere, turning into a buzzword across almost all areas of society.
We draw the semantic network graph through VOS Viewer software according to search results in Web of Science. It demonstrates the degree of impact and association of these keywords with AI. It can be observed from the link's colour that AI has been widely studied in literature. The idea is a gene of “system” science and algorithms like “neural network”, “classification”, “prediction” etc. are perspective. The research areas within the scope of AI include systems and engineering, brain science, psychology, cognitive science, mathematics and computer science.
The scenarios where AI plays a role are extensive, including speech recognition, image processing, natural language processing [8], smart robot [9], automatic vehicle [10], energy system [11], health care systems [12], and Fintech. In some ways, AI has actually exceeded human performance. The trend of "AI-beyond-humans" has caused a renewed interest and discussion on how AI might reshape human society [13]. While the vast majority of AI solutions are impressive, they have not scared us in the same way as The Terminator or The Matrix because capability is domain specific not all encompassing [14,15]. In this, we will see that this mainstream success has been contained to ANI (artificial narrow intelligence) and not AGI (Artificial General Intelligence). But it's not always true if you take a long-term historical or forward look [16,17]. Thus, at this juncture of important and unprecedented development in AI technologies, it is time to raise the past, present, and future tense in relation to both AI systems as well as tools based on AI [18].
1.1.1 Different Types of Artificial Intelligence
1.1.2 Applications of AI in Different Industries
1.2 Machine Learning (ML)- Machine learning is branch of AI that enables computers to learn from data and make decision and prediction. That is, machine learning is the development of algorithms that enable computers to learn from and make predictions based on data. The key word is automatic: machine learning is defined as the general approach to data sets that generates important results. Machine learning is based on the three concepts Data, Model, and Learning. The machine learning model can also be used in classification problems, often learning from past transactions to identify suspicious and fraudulent transactions, which are perceived as 'normal' and 'suspicious' transactions. Such suspicious transactions can then be filtered out for further processing and analysis through the use of machine-learning algorithms [22].
1.2.1 Types of Machine Learning Techniques
Machine learning (ML) techniques can be broadly classified into four main categories-
1.2.2 Different Techniques Used in Machine Learning
1. Logistic Regression (LR)- Logistic regression is a statistical model that is very common in machine learning applications, being used as classifier when the partitioning data is utilized to process specific tasks. Because it depends on the logistic function to predict probabilities and performance on high-dimensional datasets is particularly good when a linear decision boundary can be discerned in them. This method has its limitations: by assuming that straight lines exist between the dependent and independent variables, for example. Logistic Regression may be applied to either a classification or a regression problem, but it is more commonly used in tasks linked with classification [24].
2. Support Vector Machine (SVM)- The Support Vector Machine is a basic building block of machine learning. It has been widely used since around 1990, and upon initial creation the support vector machine model has proven its ability to use groups of labelled training examples in different categories to make both classification and regression predictions.
3. Decision Tree (DT)- A decision tree is a tree-structured model that is used for classification. Its internal nodes each represent an attribute or variable and its leaf nodes give the terminal classification value. The root node (or head) is considered to be the topmost node. It is best for simplicity, ease of development, and not having complex model parameter adjustment but it is not suitable when high accuracy data is expected.
4. K-Nearest Neighbors (KNN)- The KNN is a popular classifier. It does so by measuring the distance between a sample with known class label (feature) and some point in space. The sample is then classified according to the class with maximum response (depending on the normalization) among nearest neighbors (those being also samples) [25].
2. DIABETES MELLITUS
Diabetes mellitus constitutes a wide spectrum of metabolic disorders, all sharing the common feature of longstanding hyperglycemia that results from impairment in insulin secretion, action or both. Long-term exposure to elevated blood glucose leads to sustained structural/functional damage in several organs, including the retina, kidneys, peripheral nerves, heart and the vasculature.
Diabetes mellitus develops as a continuum of pathogenetic mechanisms. These mechanisms vary widely, from autoimmune destruction of the β-cells in pancreas and absolute lack of insulin to abnormalities which leads to resistance of cells to insulin. Disorders of carb and lipid metabolism are associated with the failure of insulin to act on its target tissues. This dysfunction can result from less insulin being made by the cells, or a reduced response to the signal pathways laid out by insulin, or both. Deficient insulin secretion is commonly intermingled with reduced sensitivity to insulin in individuals, complicating discernment of the most influential cause for hyperglycaemia [26].
Polyuria, polydipsia, unexplained weight loss (with occasional polyphagia), and blurred vision are well described symptoms of marked hyperglycemia [27]. Prolonged excessive blood sugar can lead to altered growth and development, delayed wound healing, susceptibility to certain infections and cataracts. Without proper treatment, acute and life-threatening metabolic crises such as diabetic ketoacidosis or hyperosmolar hyperglycemia states can occur [28].
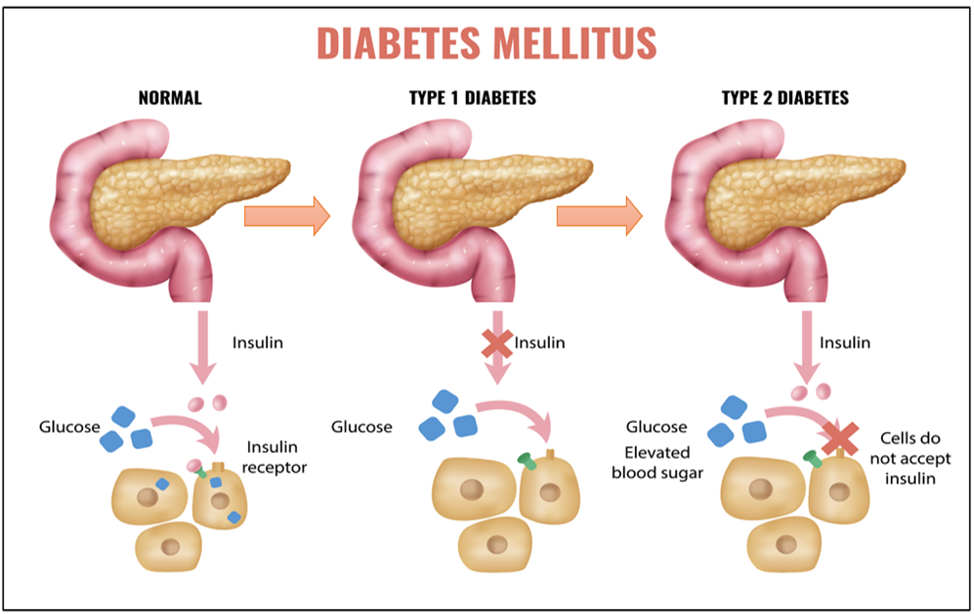
Fig. No. 1: Pathophysiology of Diabetes Mellitus illustrating Difference Between Normal Insulin Function, Type 1 Diabetes and Type 2 Diabetes
Diabetes chronicles complications involve many organs of the body. These complications, such as diabetic retinopathy with the risk of visual loss, nephropathy leading to end-stage renal disease and peripheral neuropathy that predisposes patients to foot ulcers, amputations and Charcot arthropathy. Autonomic neuropathy can present with changes in gastrointestinal, genitourinary and cardiovascular function and sexual dysfunction [29].
Dyslipidaemia and hypertension often coexist, which influences the global cardiovascular risk. Diabetes can be divided into two main groups from the etiopathogenetic point of view. Type 1 diabetes results from an absolute deficiency of insulin secretion, typically secondary to autoimmune-mediated β-cell destruction. Individuals at risk can often be identified by serological markers of autoimmunity and specific genetic profiles. Type 2 diabetes, which accounts for the majority of cases, is characterized by a combination of peripheral insulin resistance and an inadequate compensatory insulin secretory response. In many cases, hyperglycemia develops insidiously and may remain asymptomatic for an extended period. During this latent phase, abnormalities in glucose regulation such as impaired fasting glucose or impaired glucose tolerance can be detected through biochemical testing before overt disease develops [30,31]
2.1 Classification of Diabetes Mellitus-
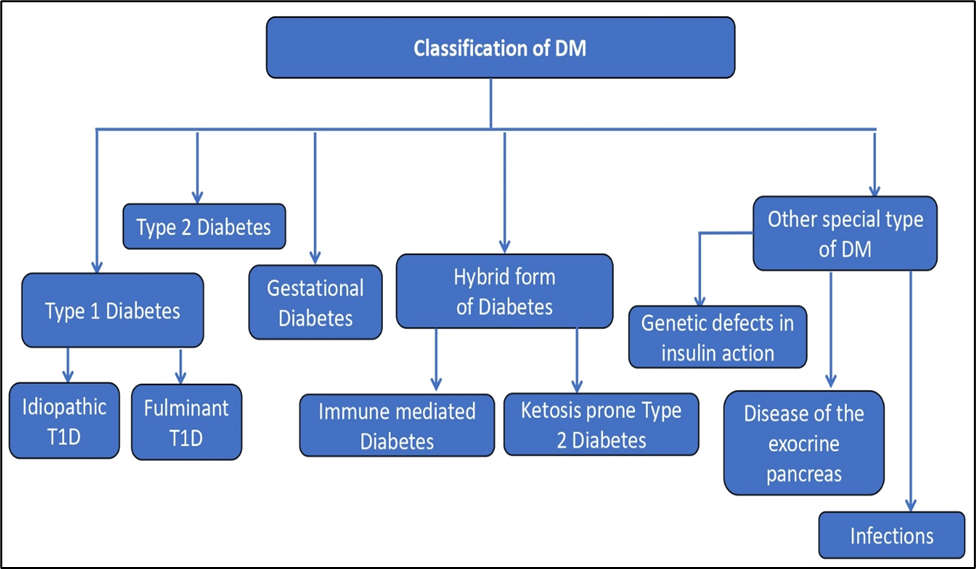
Fig. No. 2: Classification of Diabetes Mellitus (DM)
2.1.1 Type 1 Diabetes
Type 1 diabetes (T1D) can often be identified well before clinical symptoms appear, as insulin secretion starts to progressively decline at least two years prior to diagnosis During this early stage, pancreatic β-cells become less responsive to glucose. The second phase of insulin secretion is greater when the first phase diminishes. Following diagnosis, the decrease in insulin sensitivity progresses more rapidly. A biphasic pattern of insulin loss has been confirmed by studies in the first years after diagnosis, with a higher initial rate of decline and the subsequent period of lower volume reduction.
Insulin secretion declines further with the passage of time until it virtually ceases to be produced. Blood glucose may trend towards the high-end of normal, and variability in glucose is evident during T1D onset. Metabolic biomarkers, including dysglycemia, can predict the development of disease in predisposed populations. Changes of the glucose and C-peptide levels allow for better risk estimates and prediction models as well [32].
2.1.2 Idiopathic Type 1 Diabetes
A rare variant of T1D, idiopathic diabetes does not have an autoimmune basis and overall presents milder disease than the classical autoimmune disorder. Individuals with this variety might have occasional ketoacidosis and diminished insulin secretion. It is seen more commonly in those with African or Asian heritage [33].
2.1.3 Fulminant Type 1 Diabetes
Fulminant T1D is a distinct and aggressive form of the disease first recognized in 2000. Like idiopathic T1D, it is not immune-mediated [34]. Ketoacidosis develops shortly after the onset of hyperglycemia, and C-peptide levels become undetectable despite extremely high blood glucose concentrations (around 288 mg/dL). Approximately 20% of Japanese patients with acute-onset T1D (roughly 5,000–7,000 cases) are affected by this variant, which is primarily documented in East Asian populations.
It is characterized by rapid and near-total destruction of β-cells, resulting in almost no endogenous insulin secretion. The condition is thought to arise from a combination of genetic and environmental triggers. An intense antiviral immune response, without the typical production of pancreatic autoantibodies, may be responsible for the β-cell loss. Fulminant T1D has also been reported in association with pregnancy [35].
2.1.4 Type 2 Diabetes
In type 2 diabetes (T2D), impaired insulin secretion plays a central role in disease progression. Normally, insulin secretion adjusts according to insulin sensitivity to keep glucose levels stable. The relationship between these two factors is represented by the “disposition index,” which follows a curvilinear pattern. People with T2D have a reduced disposition index, indicating their inability to increase insulin production sufficiently to overcome insulin resistance.
Even though insulin levels in insulin-resistant, obese individuals with T2D are often higher than those in insulin-sensitive lean individuals, these levels are still inadequate relative to the degree of resistance. The first-phase insulin response to glucose is greatly reduced or absent, and the proinsulin to insulin (or C-peptide) ratio is elevated. Additionally, the maximal capacity to produce insulin and the ability of hyperglycemia to enhance insulin responses to non-glucose stimuli are markedly reduced. With time, hyperglycemia progresses and is more difficult to control because of the gradual decline in β-cell function an essential feature of T2D pathogenesis [36].
2.1.5 Gestational Diabetes
Gestational hyperglycemia is associated with poor outcomes in both the mother and child. These risks exist irrespective of whether the increased blood glucose level is or acts like type 2 diabetes diagnosed before pregnancy or develops during it. There's also the higher risk of developing diabetes later in life for babies born to mothers with gestational diabetes [37].
High maternal glucose is a significant contributor to pregnancy-related complications, such as preterm and large-for-gestational age births, macrosomia (birth weight>4.5 kg), higher rates of cesarean section deliveries, and preeclampsia. Most of these problems arise from an overgrowth of the baby due to the high levels of maternal glucose.
There are a number of factors that may increase the risk of developing gestational diabetes, including family history of diabetes, maternal obesity, advanced maternal age and certain conditions such as polycystic ovary syndrome (PCOS), not being physically active and exposure to environmental toxins [38]. Diagnosis is established by the consensus definition of specific clinical criteria, including evaluation of fasting plasma glucose levels, 75 g oral glucose tolerance test, and other pertinent diagnostic parameters [39].
2.2 Diabetes Technology
Diabetes technology are tools, including hardware, software, and devices for monitoring as well as managing blood glucose levels; to aid in the prevention of complications from Diabetes mellitus; more recently development of new Diabetic related technologies endeavouring to ease also the management of diabetes has developed. Of these, “smart” tools such as blood glucose meters, blood pressure monitors, activity trackers and wireless scales are some of the most popular connected devices used in diabetes care.
New products also continue to appear, such as smart socks that measure foot temperature to help prevent inflammation and ulcers, or miniaturised wearable electrocardiograph monitoring (ECG) telehealth sensors for better heart care. The widening spectrum and accessibility of such tools are likely to change the face of diabetes care. Furthermore, the use of smart techniques in diabetes care is a developing area which can revolutionize the lives of those living with diabetes [40].
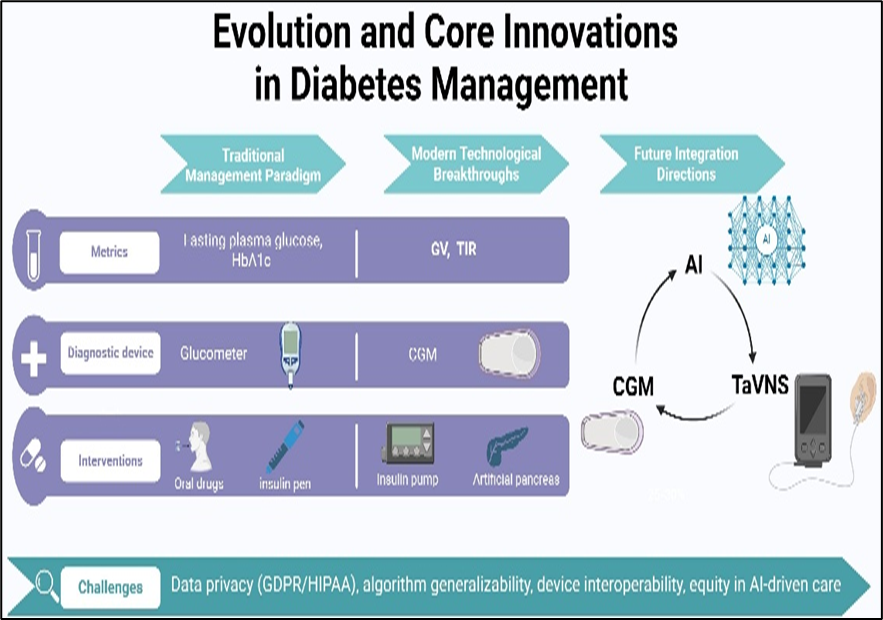
Fig. No. 3: Evolution and Core Innovations in Diabetes Management [41]
3.1 Diabetes Onset Prediction- Prediction of the diabetes onset is an important part of a preventive care in that it aims at recognizing individual high-risk probability for developing the disease prior to expressing clinical symptoms. Early diagnosis allows for prevention of the development of diabetes, ultimately reducing the prevalence.
Predictive models were available before machine learning (ML) became popular, including classical statistical methods such as logistic regression, Cox proportional hazards models and Weibull distribution analysis. For example, Abbasi et al. showed that they could predict the risk of incident diabetes in individuals without diabetes over 5-10 years, with a concordance index ranging 0.74-0.94.
With the development of AI, ML has become an excellent tool to improve predictive accuracy beyond traditional methods. Choi et al. found that ML logistic regression models had an AUC of 0.78 in predicting the occurrence of new diabetes cases in hospitalized patients within 5 years. Similarly, Ravaut et al. employed an administrative health database to build a model with AUC 0.80 for 5 years diabetes prediction. Nomura et al. used a Gradient-Boosting Decision Tree algorithm for early prediction of diabetes. More recently, Zhang et al. developed a DL model of that integrated retinal imaging and clinical risk factors in order to predict and classify the risk of new-onset T2DM [42].
3.2 Management of Modifiable Risk Factors for Diabetes- Artificial intelligence can assist in determining the risk factors that are responsible for the development of diabetes since human evaluation may be hindered or biased when dealing with large and complex datasets. In identifying these modifiable risks, AI facilitates the creation of appropriate and personalized preventative strategies. Previous studies had revealed many genetic, clinical, anthropometric, demographic and behavioral factors associated with the trans its ion from NGH to diabetes.
AI-enabled predictors have identified multiple targetable risk factors that contribute to the risk for diabetes, including high blood pressure, high cholesterol, smoking, physical inactivity, poor dietary quality and overweight or obesity [43].
3.3 Uses of AI in the Screening and Classification of Diabetes
3.3.1 Screening of Diabetes- The most classical diagnostic methods of diabetes lean on the invasive clinical measurements, influenced by ethnicity and habits. Due to the fact that early onset of T2D is usually asymptomatic, a significant number of cases remain unidentified for years. Such a late diagnosis leads often to comorbidities and shortened life span.
To solve this issue, researchers are focussing on generating more accurate, cheap, and non-invasive diagnosis method that use for receiving all data. These requirements have driven the adoption of AI solutions able to analyze large and complex data sets (including those arising from wearable sensors and continuous monitoring devices) capable of very accurate classification and making screening more accessible. AI-based approaches with personalized screening strategies on high-risk populations could be a promising way to promote the public participation in early diabetes detection [44].
AI applications in diabetes diagnosis predominantly focus on two major aspects. The first one is finding the hidden or unknown predictors of the disease. For example, Tapak et al. applied several AI algorithms, such as artificial neural network (ANN), support vector machine (SVM), fuzzy c-means, random forest model, logistic regression and linear discriminant analysis to the information of 6,500 participants in Iran and did not depend on blood glucose measure. Their results indicated that the AUC value for SVM model was higher than those calculated from logistic regression and linear discriminant analysis [45]. Similarly, Maniruzzaman et al. compared different GP approaches with di?erent kernels (linear, polynomial and radial basis) against classical classifiers including linear, quadratic discriminant analysis and naïve Bayes. The radial kernel Gaussian process performed optimally [46].
The second line of research involves advanced sensing technologies and innovative new forms of data. Shu et al. studied the facial texture features for diabetes detection with 8 separate texture extraction methods. Their SVM model led to an impressive accuracy (99.02%), whereas sensitivity and specificity were estimated to be 99.64% and 98.26% respectively. Li et al. constructed a non-invasive risk prediction model via integration of tongue feature fusion and ML algorithms to achieve an accuracy of 0.821, AUROC (area under the receiver operating characteristic curve) of 0.924 in pre-diabetes/diabetes prediction. Additionally, Zhang et al. demonstrated that deep learning models could accurately identify T2D based on retinal fundus images alone, or in conjunction with clinical data, yielding AUROCs between 0.85 to 0.93 [47].
3.3.2 Technology in Diabetes Prediction- Artificial intelligence techniques such as data mining, machine learning (ML), and deep learning (DL) are increasingly being applied to predict the onset of diabetes by analyzing statistical and historical data. These methods rely on identifying common early signs of diabetes, including metabolic irregularities and hyperglycemia, which pose significant risks to vital organs such as the eyes, kidneys, and nervous system. Data related to these indicators are collected and then modelled by incorporating variables like age and gender to improve prediction accuracy.
One notable algorithm used in this context is OPTICS (Ordering Points to Identify the Clustering Structure), an enhanced version of the DBSCAN (Density-Based Spatial Clustering of Applications with Noise) algorithm. OPTICS overcomes DBSCAN’s limitations by using a clustering approach based on the BIRCH (Balanced Iterative Reducing and Clustering using Hierarchies) algorithm, allowing for more effective grouping of data and the selection of the most relevant information for subsequent predictive analysis [48].
3.4 Uses of AI in the Comprehensive Management of Diabetes
Artificial intelligence (AI) has emerged as a transformative technology in enhancing the diagnosis and management of diabetes mellitus (DM) by improving diagnostic accuracy, facilitating early detection, and optimizing patient care. AI-based algorithms have the remarkable ability to analyze and interpret large and complex datasets, such as electronic health records (EHRs), laboratory results, genetic profiles, lifestyle data, and continuous glucose monitoring (CGM) readings. By identifying hidden patterns, correlations, and predictive biomarkers that may not be evident through traditional diagnostic methods, AI enables clinicians to detect diabetes onset at an earlier stage with higher precision. Machine learning and deep learning models continuously refine their performance through data training, improving their capacity to predict the risk of developing diabetes and its related complications. This data-driven approach supports personalized risk assessment, enabling tailored preventive and therapeutic strategies for individual patients. Moreover, AI assists in monitoring disease progression, optimizing treatment regimens, and ensuring timely medical interventions. By integrating AI into clinical practice, healthcare professionals can make more informed, accurate, and efficient decisions. Overall, the application of AI in diabetes diagnosis represents a significant advancement toward predictive, preventive, and precision medicine, ultimately leading to improved patient outcomes and reduced disease burden.
Table 1: Summary of AI Uses in Diabetes Management
|
Sr. No. |
Uses Area |
Specific Task |
AI/ML Techniques Used |
Key Finding |
|
1. |
Prediction and prevention |
Predict future onset of diabetes |
Logistic Regression, Decision Trees, Deep Learning (DL) |
Models can predict diabetes 5 years in advance. |
|
2. |
Screening and Diagnosis |
Non-invasive screening for T2D |
Support Vector Machines (SVM), Deep Learning, Gaussian Process. |
DL models using retinal fundus images achieved high accuracy for detecting T2D. |
|
3. |
Glycemic Control |
Predict blood glucose (BG) fluctuations |
Recurrent Neural Networks, Artificial Neural Networks. |
ML algorithms for predicting hypoglycemia showed high pooled sensitivity and specificity. |
|
4. |
Complication Management |
Automated screening for diabetic retinopathy |
Automated retinal imaging analysis |
AI systems can anticipate complications like retinopathy, nephropathy, and cardiovascular disorders. |
Moreover, AI systems can anticipate the development of diabetes-related complications such as diabetic nephropathy, retinopathy, and cardiovascular disorders through the analysis of comprehensive patient datasets. These predictive insights enable early diagnosis and preventive interventions for secondary complications. AI-driven platforms also enhance remote monitoring and telemedicine services by enabling continuous patient assessment and real-time diagnostic adjustments. By integrating data from multiple sources and presenting a comprehensive view of the patient’s health status, AI supports more informed and accurate diagnostic decisions. Collectively, these technological advances have strengthened the efficiency, precision, and timeliness of diabetes diagnosis, thereby improved patient care outcomes and alleviating the burden on healthcare systems.
3.4.1 Health education
Health education involves more than giving information to patients; it sets the foundation for the self-management of diabetes. Alotaibi et al. designed the intelligent mobile diabetes management system, whose pilot study showed it could reduce HbA1c levels and improve participants’ basic diabetes knowledge [49]. Hamon and Gagnayre used natural language processing techniques on web forms to uncover patients’ knowledge gaps and propose personalized educational plans. Most recently, Chen et al. used intelligent mobile health technology for diabetes education to assess its impact on glucose control with patients with T2D, who were starting pre-mixed insulin. The combination of the 12-week education and the insulin initiation helped in the management of T2D by causing a significant reduction in the patients HbA1c levels [50].
3.4.2 Automatic Diet Monitoring
Inaccurate self-reporting of food intake is a huge obstacle in dietary management of patients with diabetes [51]. This highlights the need for automated solutions in dietary monitoring. Based on level of automation, a monitor system can be classified as semi-automatic or fully-automatic. For semi-automatic systems, users have to indicate the position of food on a plate, 'marking' the food. For fully-automatic dietary systems, users upload food pictures to a central system which estimates dietary composition. This means that photo analysis systems need to address image segmentation, food recognition and classification, volume estimation, and conversion of estimated volume to calorie [52].
Recent advances in technology indicate an improvement in estimating energy intake from images of food. For instance, in the work of Vasiloglou et al., the smartphone system GoCARB, specially designed for T1D patients, can estimate the carbohydrate content of a patient’s meal [53]. The estimations by GoCARB system did not differ from those of dietitians for any meal size. Zhang et al. designed a system that automatically identifies food, records the calories and nutrients, and requires no user input [54]. When tested for 15 different food items, the system's accuracy exceeded 85%. Fang et al. expanded on the concept of “food energy distribution” to capture the four characteristics of food energy spatial arrangement in an eating scene [55]. A four-layer generative adversarial network was implemented where the user inputs a food image and the network predicts an energy distribution image. The user can then estimate the energy from the food image based on the predicted energy distribution image. The average of the estimated energies was 209 kcal per eating occasion, suggesting more work is needed for accurate estimations.
3.4.3 AI-Driven Dietary Recommendations- Maintaining healthy blood glucose levels through an appropriate diet is crucial for managing diabetes and alleviating stress on pancreatic islet β cells [56]. A well-planned, individualized diet can help regulate both blood sugar and lipid levels while ensuring adequate intake of proteins and essential nutrients [57]. Effective dietary recommendation systems for diabetic patients should be grounded in medical nutrition principles, take into account individual eating habits, and support the development of sustainable healthy behaviors.
Various AI-powered dietary recommendation systems have been designed with performance levels comparable to professional dietitians. For instance, Chen et al. developed a system that uses expert knowledge to deliver precise and convenient dietary guidance for individuals with chronic conditions, achieving 100% verification accuracy compared to dietitians’ assessments. Similarly, Zeevi et al. observed significant differences in postprandial glucose responses among individuals consuming the same meals. By applying machine learning models that incorporate factors such as eating patterns, physical activity, and gut microbiota, they demonstrated that personalized dietary plans can effectively reduce post-meal glucose spikes and improve long-term metabolic outcomes.
3.4.4 Physical Therapy
Physical activity serves as a scientifically validated, personalized, and quantitatively measurable therapeutic tool that holds great potential in diabetes management. Despite its proven efficacy, its implementation in clinical practice remains suboptimal. This shortfall is often linked to clinicians limited expertise in exercise prescription and patient’s poor adherence to exercise regimens. Several exercise programs fail because they do not account for individual motivation, exercise enjoyment, or the complexities of patient’s physical conditions.
To address these challenges, intelligent and personalized exercise prescription systems are gaining attention. Everett et al. proposed a digital coaching application that adapts physical activity recommendations based on real-time contextual data for instance, suggesting specific outdoor exercises when the patient’s location data indicates they are in a park [58]. Likewise, Sun et al. conducted a long-term intervention using a cloud-based intelligent exercise prescription platform designed for Chinese middle-aged and older adults [59]. Their findings demonstrated that such personalized digital interventions could significantly improve health outcomes, including cardiovascular function and body composition, among community-dwelling populations.
3.4.5 Blood Glucose (BG) Monitoring and Prediction
In diabetes management, daily fluctuations in blood glucose are common due to varying carbohydrate intake, insulin activity, and other physiological factors. Accurately predicting these BG changes can provide early warnings of potential glycemic excursions, allowing patients and healthcare providers to act proactively.
With advancements in continuous glucose monitoring (CGM) technology, it is now possible to collect real-time glucose data to forecast future BG levels over timeframes ranging from a few minutes to several hours. Although CGM devices typically exhibit a mean absolute relative difference of about 9%, they remain integral to predictive research. Most studies focus on short-term predictions within 60 minutes, which have proven critical for timely diabetes management.
Among the machine learning (ML) techniques applied, artificial neural networks (ANNs) are the most widely used, followed by random forest and support vector machine (SVM) models. In a meta-analysis, Kodama et al. evaluated ML algorithms for predicting hypoglycemia and reported pooled estimates of 0.80 for sensitivity and 0.92 for specificity, showing strong diagnostic potential [60].
AI-based prediction systems have proven especially beneficial during challenging contexts, such as fasting periods. For instance, Elhadd et al. developed a machine learning algorithm that integrates clinical and demographic variables, physical activity patterns, and glucose variability to predict hyperglycemic and hypoglycemic events in patients with type 2 diabetes (T2D) undergoing fasting during Ramadan.
The model achieved impressive accuracy correctly identifying normal glucose levels in 95.2% of instances, hyperglycemic events in 82.6%, though it was less effective in detecting hypoglycemia events at 27.9%. Such studies highlight the growing potential of AI-driven tools and intelligent, context-aware systems in improving diabetes care through more precise exercise prescriptions and predictive monitoring. The continuous blood glucose monitoring helps to monitor the patient blood glucose level for easily managing any problem occur when blood glucose level is immediately increased, in that condition AI driven device controlling blood glucose, the device show their response by sensors which is available in device that helps to managing glucose level.
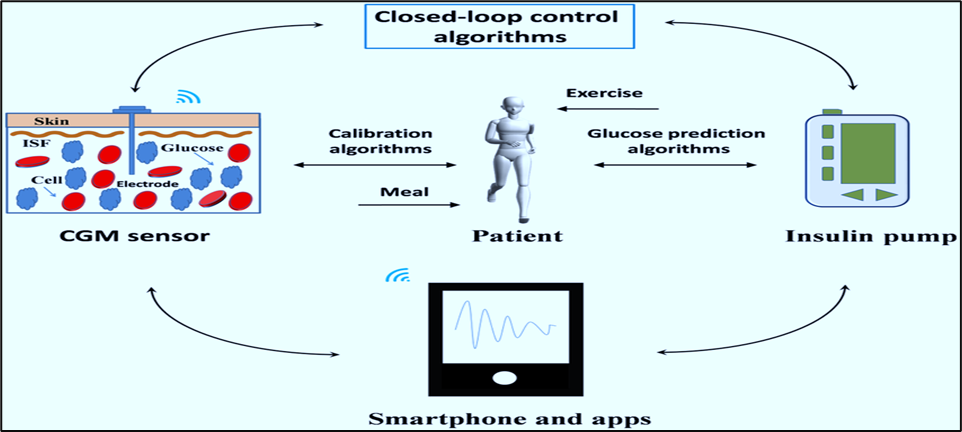
Fig. No. 4: A Schematic of an AI-Driven Closed Loop System for Automated Diabetes Management
4. LIMITATIONS
While there is great potential for the use of Artificial Intelligence in Diabetes Research and Care, there are also many limitations that must be taken into account. The performance of many AI Systems is dependent on the quality, completeness, and consistency of the data that they were trained on. This means that if the AI System was trained on a dataset that contained many gaps or inconsistencies, then the accuracy of the AI System's predictions may differ significantly from the actual situation. In addition, Models developed using AI Systems trained on data from a certain Population Group may perform differently than Models developed with data from other Population Groups and therefore might not be equally applicable across the full spectrum of Clinical and Geographic Options available within the healthcare delivery system.
User engagement with Digital Health Tools is often not sustained over time, which may impact long-term outcomes. Also, many AI Algorithms hide their internal decision-making processes, making them difficult to transparency and thus limiting their clinical acceptance. Many challenges still exist regarding the protection of patient data, ethical standards, and regulatory requirements. These different frameworks exist in different parts of the world.
Furthermore, Successful utilisation of AI in Routine Healthcare Practices requires the availability of the necessary Supportive Infrastructure, A Technical Support System, and adequate Training on how to use AI. Availability of all three Support Elements is not guaranteed in every setting.
Table 2: Key Challenges Obstructing Clinical Translation of AI
|
Sr. No. |
Challenge Category |
Specific Issue |
Impact on Adoption & Implementation |
|
1. |
User Acceptance & Adoption |
Complicated user interfaces, Lack of perceived relevance |
High dropout rates (15-20%). Discourages participation, especially from older adults. |
|
2. |
Data Security & Privacy |
Patient concerns over sensitive health data, Insufficient regulatory policies |
Patient hesitancy; nearly 60% of participants expressed apprehension about the safety of AI health apps. |
|
3. |
Digital Literacy & Equity |
Disparities in technology competence among patients |
Patients with limited digital literacy struggle to use apps effectively, which risks deepening existing healthcare disparities. |
|
4. |
Technical & Regulatory |
Algorithmic bias, Lack of interoperability between systems, Regulatory complexities for medical AI |
These barriers collectively impede large-scale clinical translation and foster a lack of trust. |
The future of artificial intelligence (AI) in clinical diabetes management is evolving rapidly with the advent of generative models, which foster the development of inclusive and comprehensive medical AI systems. These generalist models could improve diabetes care through continuous monitoring of risk factors, early detection, optimization of medication dosages, and prediction of complications. The integration of wearable devices and the Internet of Medical Things (IoMT) enable smooth data sharing with enhanced interoperability, cybersecurity, and reliable transmission capabilities further strengthened by advanced 5G network infrastructure. Large language models (LLMs) represent a major technological milestone, capable of engaging in natural, interactive communication and offering meaningful support to healthcare professionals. Building upon this, LLM-based autonomous agents with attributes such as responsiveness, initiative, and social intelligence have been introduced, allowing them to interpret complex medical data and perform multifaceted tasks beneficial for diabetes management.
These developments signal progress toward more universal AI systems, including artificial general intelligence, that can augment traditional clinical workflows by improving efficiency in data handling and decision-making. To ensure the effective and sustainable integration of AI in diabetes care, close collaboration among healthcare providers, data scientists, and AI developers will remain essential for ongoing innovation and refinement.
AI's contribution to diabetes care is increasing through improved risk prediction, increased accuracy of screening, and the ability to manage diabetes on an individualized basis. For example, artificial intelligence applications including machine learning and deep learning, wearable devices, and digital health platforms have been shown to improve glucose monitoring, lifestyle changes, and detection of complications. Artificial intelligence also creates new possibilities for improving diabetes care via more proactive, individualized, and data-driven methods. While artificial intelligence has potential to become integrated into routine diabetes care practices, the factors that continue to influence the widespread adoption of this technology include data quality, the ability to understand and interpret AI-generated data, privacy and security issues, infrastructure and resource availability, and patient and clinician engagement with AI. To facilitate long-term acceptance and integration of AI technologies in diabetes care, it will be necessary to overcome these barriers by using appropriate validation, ethical oversight, and clinical integration. This technology should be viewed as an adjunct rather than replacement for the clinical decision-making process, and further research and collaboration are needed to ensure the safe, effective, and equitable utilization of AI in diabetes prevention and management.
REFERENCES

Bhupendra Mourya, Dr. Akash Yadav, Dr. Dinesh Kumar Jain, Role of Artificial Intelligence in Diabetes Care: Present Uses, Limitations, and Future Directions, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1993-2011. https://doi.org/10.5281/zenodo.18317870
 10.5281/zenodo.18317870
10.5281/zenodo.18317870
