Dr. Shivajirao Kadam College of Pharmacy, Kasabe Digraj, Sangli (MS), India. 416305.
This narrative review also emphasizes the need for pharmacists in mental health care through skills in medication management, provision of counselling, and encouraging patient’s adherence to strategies. Even though these roles seem to impact positively, most of the papers available nowadays have no controlled designs which diminish the value of the evidence. Therefore, future studies should use more rigorous methodologies to measure the impact of services delivered by the pharmacists in mental health directly. Early evidence suggests that pharmacists are actively involved in collaborative drug therapy management, taking part in multidisciplinary teams, and also working to reduce antipsychotic polypharmacy. Nonetheless, future studies should employ more rigorous designs, specific evaluation tools, and longer follow-up, to strengthen the evidence. Enhancing medication adherence may also be achieved through customizing pharmacist services to the specifications of individual patients and applying multi-component strategies. In addition, the widespread diffusion of such guidance for practice may also involve addressing mental illness stigma as a barrier to the deployment of evidence-based pharmacy services. Training programs that target stigma reduction and assist the pharmacists in their extended role need to be instituted to increase the effectiveness and reach of the pharmacist-led mental health care services. In this way, the pharmacists' contribution toward augmentation of mental health may be better optimized.
Mental health conditions, and patients’ personal experiences, Pharmacists are often on the frontline, helping to address concerns about side effects, adherence, and overall treatment outcomes. As mental health awareness grows, so does the responsibility for pharmacists to provide compassionate, informed care, making their role essential in helping patients navigate both their mental health journeys and their medication needs. Mental health disorders are rapidly involving primary healthcare providers of diagnosing, treating, and advocating, the therapeutic role of pharmacists is often underestimated and unknown. Some 450 million people suffer from mental, neurological, or substance use disorders, and the vast majority of them lack of adequate treatment. In communicating with patients, pharmacists are uniquely placed to improve mental health and reduce the overall impact of many mental disorders due to the fact that the majority of conditions are treated pharmaceutically. The objectives of this narrative review are: To examine the evidence for pharmacist-led services in mental health, the barriers and facilitators of implementing pharmacy services in mental health with focus on factors such as organisational culture and mental health, they contribute to ensuring appropriate use of medicines through medication reviews, adherence promoting strategies, antipsychotic polypharmacy management and shared decision making.
To determine the current best evidence regarding pharmacists’ roles in the mental health interventions, we performed a narrative review. While the review was not systematic and was limited to key field of pharmacy interventions in mental diseases, the sources used for the review included interviews with experts, as well as evaluations of references provided as well as electronic databases such as PubMed, Medline, Go ogle Scholar.
Figure 1: Reflections in the pharmacy: mental health and medication
2.1 Pharmacists assume an important place in the multidisciplinary health care teams
In recent times, both government bodies and international organizations have increasingly called for the inclusion of pharmacists in multidisciplinary healthcare teams [1]. This is even more evident when there are financial incentives offered by governments and other payers, where pharmacists are compensated for professional services that are offered collaboratively with other health professionals. Such programs include Australia’s Home Medicines Review, UK’s Medicines Use Review services, USA’s Medication Therapy Management, and medication review services in New Zealand [2-5].
Pharmacists, as pharmacotherapy specialists, possess distinctive knowledge, skill, and viewpoints which back and supplement the abilities of other health care professionals. Their position on a multidisciplinary team is very often diverse and includes the provision of medication therapy management services such as MTMPs (Medication Therapy Management Program) to manage, solve or prevent medication-related problems, assure safe and effective drug use, educate patients and providers on drugs, maintain patient compliance to drug therapy, and advocate for health promotion and lifestyle changes in the community.
Pharmacists are working at the primary level, extent community pharmacies, or general practices, and also at the secondary level, which comprises other specialized healthcare establishments. In a hospital or a residential aged care facility, a considerable number of practitioners have access to views of the patient’s clinical notes and have the potential for direct communication with other health care workers, which promotes the employment of pharmacists in the management of patients with mental illnesses in these areas [6-10]. There is however, literature on involving pharmacists within multidisciplinary teams with mental health focus, which has reported good results. One research looked at the perceptions of both health care professionals and patients with regard to the pharmacist's role when they are a member of the mental healthcare team. Healthcare professionals and patients viewed the pharmacists as some of the mental healthcare team members needed in pharmacotherapy management after medical evaluation and diagnosis smoke as chiro prescribers [11].
Pharmacists in primary care are usually not in direct contact with clinical data of the patients or other health workers. This however is not the case in the community pharmacies where patients do not require appointments to be attended to. This means that patients have the option of seeking help on self-limiting diseases, preventative services and issues of greater concern even before they visit the GP, and at times when it would be more appropriate than visiting the GP [12]. This makes pharmacists capable of acting as the very first person who consumes a contact within the healthcare system in order to serve as a point of triage or as a connector to other healthcare professionals including physicians. A study by Wang et al. in the US shows how a psychiatric pharmacist facilitated patient access to mental health, psychotherapeutic and social services at a community health centre with limited psychiatry resources [13]. Pharmacists’ collaboration with other health professionals presented favourable results to the forensic circumstances as well. Regular interactions of a psychiatrist and a pharmacist within the framework of benzodiazepine guidelines and their adjustment in addition to routine tasks dramatically decreased this particular drug’s prescription rates in the course of imprisonment [14].
Another type of integrated care is Collaborative Drug Therapy Management (CDTM), where an agreement that is in place between pharmacists and physicians facilitates pharmacists in performing various roles like assessment of patients, alterations of medications and evaluation of patient’s response to pharmacotherapy [15]. This model has demonstrated an ability to identify and solve inappropriate medication use when practised in primary care and mental health care settings among homeless patients [16]. In mental health clinics, common interventions used under CDTM have included patient counselling, dose changes, discontinuation of drugs, or commencement of other therapies.
Collaborative care has enabled the incorporation of case conference interventions in many healthcare systems. Specifically, in such interventions, a case conference is a term used to refer to a meeting that involves two or more healthcare workers from various professional disciplines willing to collaboratively assist a patient[2].In cases of medication management review services, case conferences have their unique benefit of enabling in person interaction between the physician who requests the case conference and the pharmacist conducting medication review[17].Such situations enable both disciplines to communicate about a patient’s particular medications’ needs and issues as they arise. All of these factors can help facilitate the clarification of treatment goals, the resolution of unmet expectations, and the overall management of a patient’s healthcare [17].

Figure 2: Pharmacist’s multifaceted role in healthcare
2.2 Pharmacist’s role in screening and risk assessment in mental illness
As the third leading global cause of disease burden worldwide, depression is acknowledged all over the world; however, very few people seek help due to their symptoms [18-20]. Mental health stigma creates barriers in seeking help for these individuals. This encompasses treatment stigma, which is the stigma connected to the act of trying to look for or receiving mental health treatment, and internalized stigma which can be defined as personal level of shame or embarrassment associated with the act of trying to seek help [21]. A considerable number of people also have never heard about the existing mental health care options or may not see the signs of depression and correlate its symptoms with a depressive disorder. It is usually the case that a person suffering from a mental disorder report to a medical practitioner for a physical ailment first. There is a study by Fernandez et al that shows area in which GPs made greater chances of diagnosing depression emanating from a patient’s complaint that was emotional or mental. This is an era where it is imperative that individuals know the distinctive features of depression and how to diagnose it [22].
Research on the screening of depression reveals that screening is the most effective way of improving the early detection of depression and anxiety disorders [23]. The controversy surrounding routine depression screening for asymptomatic individuals is largely due to the lack of clinical evidence [24]. It is worth noting, however, that pharmacists can assist in conducting opportunistic screening in the community. Pharmacists are in a very favourable position because they do not need appointments to be accessed, and the public has a high level of trust in them [25]. Evidence from studies suggests that trained pharmacists may be able to assist in the identification and management of depressed patients [8,26]. Identification of depression and the determination of the risk may assist in the early identification of symptoms, thus facilitating rapid referral to appropriate health care services. However, the effectiveness of depression screening partition relies on the effectiveness of the screening tool, which should also be dependable. The patient’s health questionnaire and the WHO-5 Well-being index are among the screening tools that have been found to be reliable and valid for primary care [27-29].
Pharmacists in the community have become familiar with conducting screening and risk evaluation for chronic diseases and other health related conditions such as diabetes, hypertension and respiratory diseases [30]. Patients are not screened for depression in these cases. There is some indication that community pharmacists are able to screen for depression and refer patients to healthcare providers further back in the depression. It was also found that community patients or members with higher risk of depression who would otherwise be missed can be screened by pharmacists at the community level [31]. They are able to perform depression screening and refer patients to other health care providers as appropriate. Some of the patients who have been identified in the community using pharmacy services have been patients with active suicidal ideation. Since depression is a common disorder, there is a need emphasised for pharmacists to undertake appropriate form of training in mental health first aid. There have been changes especially among pharmacy students who undergo training in mental health first aid and barrier B where the students reported improvement in their performance particularly in managing mental health. Furthermore, patients should never be left without needed psychiatric assistance, for this to work there is a need for closer ties between surgery and pharmacy practice [32-34].
A number of barriers and facilitators have been identified in enhancing the extent of depression care services in the pharmacy setting [33]. Consistent to other findings, stigma, and self-stigma or stigma from other areas of the healthcare’s team members have population put some hindrances on its effective prevalence. Other barriers are addressed limitations of time, lack of privacy, and poor remuneration of professional roles of a pharmacist. A major facilitator that was provided by pharmacists is the endorsement of the pharmacy as a nice place to speak about mental health issues through specific advertising [33]. This endorses an earlier Australian study which said that when the patients trust the pharmacist, they feel that it is safe to discuss the mental health matters at the community pharmacy. Therefore, this illustrates the roles of an inviting culture and the relationships with practitioners in the provision of mental health services [35].
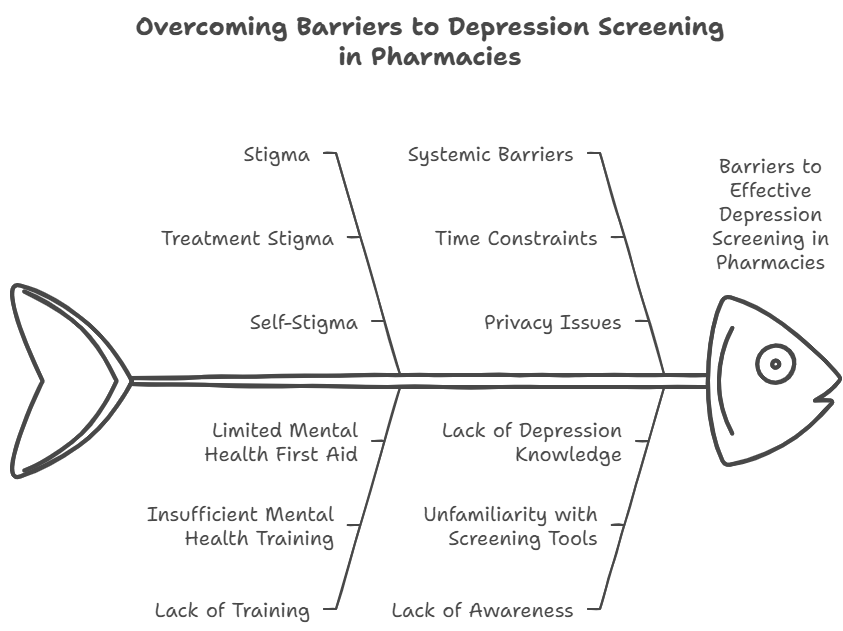
Figure 3: Overcoming barriers to depression screening in pharmacies
The biomedical model of mental disorder is a theory that supports the use of medication to treat mental illness. It posits that mental disorder are brain diseases and that pharmacological treatment is the best way to target biological abnormalities.
Depressive disorder, a bipolar disorder, and schizophrenia are all closely associated Depressive with taking medication as the first step in their treatment. That is, pharmacists can help in the treatment of these disorders through performing medication reviews towards safe and effective use of medicines. Community and hospital studies review have also pointed out this important clinical practice for pharmacists [36,37]. Bell et al. reviewed community and other healthcare professionals’ pharmacy services for patients with handicap, more specifically, patients with psychological complications where community pharmacy programs were reviewed in 22 research studies providing for professional services to the patients n= 10 and other healthcare givers n =12[37]. The results pointed out that, especially, pharmacists are primarily involved in assisting with the review of medications for medicine optimization to lessen the chances of inappropriate medications. It has also been demonstrated that filling out prescriptions together with monitoring them helps improve compliance to antidepressants. However, studies employing a more robust design are required in order to assess the effects of the provided services in regard to pharmacy on the mental health of patients in the community.
A more recent review by Richardson et al. explored 18 hospital studies based within hospitals’ departments of pharmacy, looking into the provision of health interventions designed for patients, such as reviewing a medication chart, assessing lab results including prescribing medications, or even counselling to either the patient or the provider [36]. This review, however, reported that more than a single service was rendered to the in patients with mental disorders and the pharmacist had an important role in mental healthcare in improvement with some activities. But there is relatively little evidence that would support such a conclusion. When ranked according to Australian guidelines for evidence hierarchies provided by the National Health and Medical Research Council (NHMRC), there is no study met with level I evidence (which is reviews of randomised control trials) and there is only November whose type of study was of level II (which is an RCT). The rest were based on much weaker uncontrolled designs.
3.1 Review of medication
In residential aged care homes, the psychotropic drugs including antipsychotics, sedative and hypnotic drugs, are often over used in elderly residents [38]. These medications which –if not adequately controlled- can have harmful effects when overused. In light of possible dangers, Alldred et al., and others carried out a Cochrane review aimed at evaluating such approaches focused on medication reviews as a means of promoting rational prescribing. Eight randomized controlled trials were part of this review which focused on the enabling role of reviews in venting out and correcting medications that are misused. The results from this Cochrane review which has been aimed at centring on drug related problems as performance objectives should acknowledge that the medication reviews have and performed the centrical sets of activities demonstrating outcomes that were actually anticipated.
Namely, the rate of adverse drug events, the rate of hospital admission, and the rate of mortality did not show an effect. Neither was the secondary measured outcome [39], quality of life, improved suggesting that these reviews would be effective in the adjustment of the medications but would not impact the overall health status of the residents or other broader health measures.
3.2 Medication adherence
The issue of adherence to psychotropic medication, particularly in the case of the mental health sector of care, remains a common issue and a general concern [40-43]. Speaking of the various types of psychotropic medications, the problem of adherence is particularly acute in the case of antidepressants. However, the nonadherence rates for those who take these medications are the highest, and this represents a significant obstacle to effective treatment. It is critical that individuals who take antidepressant drugs in such circumstances remain compliant with this aspect of their therapy, as it helps in the attainment of several critical targets which are the reduction of symptoms, restoration of an individual’s functioning to the pre-depression levels, and prevention of any relapses into depression. Further, compliancy to medical treatment, in this case antidepressant therapy, prevents increased health care expenditure and cost related to mental illness treatment by decreasing the possibilities of the relapse and need for further intervention. There has not been a shortage of literature on different methods and interventions directed towards enhancement of adherence to antidepressants. However, most of the studies used in these trials have been based on complicated strategies targeting several impediments to adherence simultaneously. Case management and collaborative care approach were the common elements within these interventions. In a case management approach, patients are offered support and follow-ups by a given practitioner within the health care setting integrative collaborative care [44-46].
Various efforts have been put in place to improve adherence to psychotropic medications which includes the use of antipsychotics for psychosis management. Nevertheless, such studies on interventions designed to enhance adherence to antipsychotic medication are very few. The absence of these studies in the literature might be explained by certain factors. One apparent factor is the stigma towards the patients of the severe mental illnesses’ some pharmacists may carry with them, which would help to explain their level of active patient engagement. Evidence further suggests that there are also other situations where, due to the nature of severe mental illnesses and their common intra- and inter-derivation, pharmacists may feel more comfortable bothering with patients’ care requiring physical health management rather than doing so with patients’ care involving mental health. One study of interest was a pharmacy-based intervention aimed at addressing the low levels of adherence to antipsychotic medication among patients suffering from serious mental illness. Results of this intervention were positive as measuring medication adherence revealed significant improvements among patients who participated. The intervention incorporated some essential strategies that aimed at simplifying adherence to treatment among patients. One of these strategies was the use of unit-of-use packaging [47-50].
3.3 Using multiple antipsychotic medications together
In medications, other than antipsychotics, such as mood stabilizers and or antidepressants, are very likely to be prescribed for clozapine patients. Chronic use of clozapine not only increases the likelihood of interaction with other medications but also raises the chances of more negative effects. Among them: medications prescribed for anxiety that cause sedation might reduce the efficiency of clozapine and increase negative side effects when used in combination [52]. Clozapine is a lasting antipsychotic and is considered as drug of choice for many patients. Of note however would be Cochrane review that pointed out that use of patients' self-reports is associated with high internal bias. This phenomenon is known as ‘reporting bias’. It causes further issues with documentation, as patients tend to forget what medications they are taking when they are combined with supplementation. For some patients, long-term clozapine treatment raises concerns or causes adverse effects, whilst several studies have shown its high efficacy. A small group of Clozapine patients correlating with 24 history of poultry farm specific therapies study patient representation in the community tended to overuse clozapine, which is quite common practice. Most prescriptions of clozapine usually arise from other clozapine patients’ YouTube channels which has some degree of charm. Unfortunately, this validity is questionable and leads to those patients with self-reported combining clozapine with multiple other medications or combining it with non-prescribed supplements [53-54].
Clozapine raises worries as even a single tablet can interact with other non-antipsychotic drugs increasing their toxicity and levels of side effects further, chronic use. These tablets containing clozapine have metabolites that can affect both systems leading to more toxicity. Clozapine has long been targeted as an antipsychotic treatment; much has changed over the last 50 years making it difficult for elderly patients to combine treatment with clozapine with multiple other tablets. New guidelines raised in the past decade made clozapine the go to for many branded drug companies. However, due to over prescriptions and such an influx of clozapine patients in the healthcare system, potential overuse was imagined leading to ketamine being promoted as an alternative [55].
3.4 Making healthcare decision together
The biomedical perspective that has been the norm in management across the globe is continuously being replaced by a patient-oriented model that is more effective with numerous initiatives being put in place to support it. In patient-centred care, patients, family members, and representatives from the healthcare team work in collaboration to address the requirements, expectations, and the views of the patient with particular attention to mental health where behavioural and emotional factors are important. It has become commonplace for patients to be engaged in various aspects of their care including decision making. Like other health care professionals, pharmacists are an important part of this transition and appreciate the need for patient-centred care. Research indicates that patients’ health outcomes, satisfaction, and trust are improved when pharmacists engage in professional and patient-centred communication. Nevertheless, there is evidence that a good number of pharmacists have retained the traditional focus on medications frequently adopting a biomedical framework with minimal psychosocial interventions or considerations during consultations even in mental health cases [56-59].
Evaluation of such programs suggested improvement in patients’ psychosocial context amongst healthcare providers, pharmacists in particular while addressing patients’ communication issues. Programs aimed at enhancing educational outcomes boost pharmacists’ self-assurance and listening in mental-illness focused scenarios, however, there are still gaps.
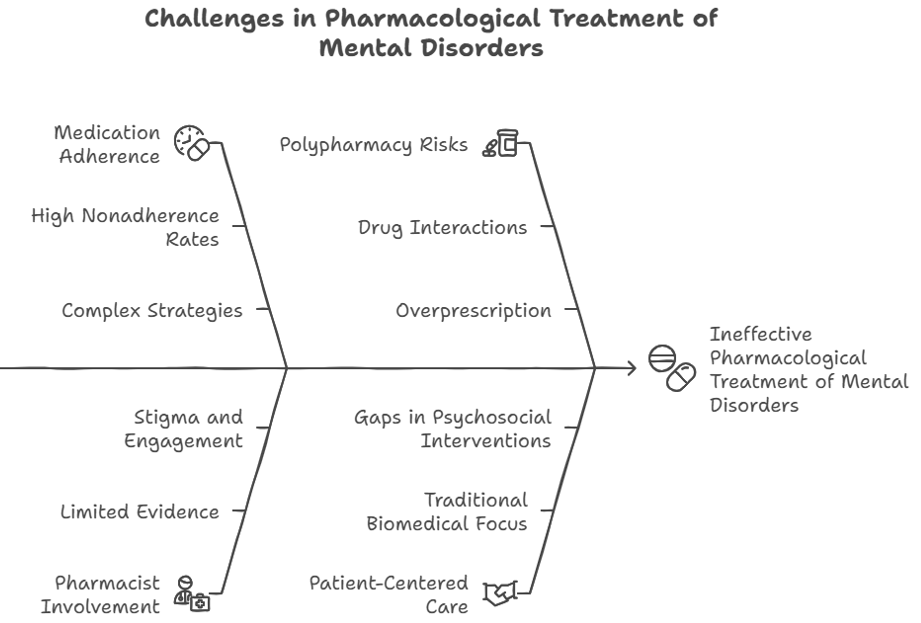
Figure 4: Challenges in pharmacological treatments of mental disorders
4. EVALUATING THE FACILITATORS AND BARRIERS TO THE DEVELOPEMENT ON MENTAL HEALTH INTRGRATED SERVICES WITHIN PHARMACY PRACTICE
Any time a pharmacy puts into effect a new service, there will be difficulties, and providing services to mental health patients has its own distinct drawbacks. Ensuring that the particular barriers are dealt with and thus the pharmacist’s involvement in mental health care is improved will set successful service implementation.
4.1 systematic culture
However, the progress from simply preparing and dispensing medications to offering complete pharmaceutical care services has its challenges. In particular mention has been made in the previous literature on the development of the services of the specific challenge such as pharmacist’s attitude and stigma and skill related variables in regard to mental health care of customers [61]. The culture of the workplace is also influenced by the attitudes, belief and value of its workers and in this case individual pharmacists may impede the delivery of these services [60-63]. Although increased access to these types of service is very important; organizational culture in pharmacy has not been clearly researched [64], more specifically how it affects the use of pharmacy focused services for people with mental illness. Recently, studies examined the impact of organization culture which existed on non-medics adopting mental health care roles within primary and social care services. The organization culture was found to be able to predict extent of participation on mental health promotional evaluation and educational roles at system level. Among others it includes working together with other services in delivering health promotion on social emotional wellbeing issues [65].
The literature review of the organizational culture of community pharmacy practice focused on the conflict that exists between the commercial and the professional perspectives of the pharmacists which in this case, is not uncommon in this field [64]. This is because the business of running a pharmacy entail making money from selling medicines and this sometimes runs counter to the other services carried out by the pharmacy which are focused at enhancing and optimizing patient’s care. This new dynamic condition seems to increase the tension between the business side of the pharmacist and the professional side of the pharmacist’s functions. Some countries have, however, shifted their pay systems to enable the delivery of these services, particularly pharmaceutical care services but this is not the norm and is just an additive to the pharmacist’s earnings. Other structural changes required for effective provision of these services include density of pharmacy outlets with incorporation of a private booth for consultations, management of pharmacy outlets to include more interaction with the technological devise, and strong linkages with other relevant specialists in the health care system [60].
4.2 Stigma surrounding mental health
The mental illness stigma occurs when a negative attitude is associated with one or more signs of mental illness due to ignorance and its misconceptions [66]. Stigma presents itself in three forms: knowledge deficit (ignorance), unfavourable attitudes (prejudice), and discriminatory social action (behaviour) [67]. It is increasingly evident that practitioners of mental health, too, can hold stigmatizing views and behave in a prejudiced manner. A form of stigma is diagnostic overshadowing. It is where patients are treated differently by their care givers once their underlying mental illness is known to them. More importantly, research works suggest that consumers view mental health staff as some of the most conspicuous stigmatisers. The effects of stigma are probably the most severe, leading to social exclusion, delay in help-seeking, inadequate treatment, barriers to care, and lack of compliance with the prescribed treatment. Further, people suffering from mental illness are expected to have poor health conditions and a life span that is 15-20 years shorter than that of the general population [68].
Even with the ability to identify some mental illnesses and offer treatment, health professionals share most of the negative attitudes the general population holds toward people with mental illness [69-71]. To this effect, health professionals as well as pharmacists in particular, can be stated as one of the few health-related professions who can also carry stigma or help to alleviate it. Some researches on the other hand do find that pharmacists exhibit general positive attitude towards patients with depressive and other mental disorders, but they do show more stigmatizing attitude for patients suffering from schizophrenia. This is consistent with other studies done on pharmacy students globally which find quite on the contrary towards patients with schizophrenia and depression among students. Importantly, pharmacists are more at ease talking about treatment of depression than treatment of schizophrenia. A lot of people are uncomfortable in exploring issues relating to mental health, and in such cases, they are less likely to see patients suffering from the mental health conditions as compared to those with mental health problems related to the cardiovascular systems. Strikingly also, the prevalence of schizophrenia among patients and their pharmacy stigma is found to be inversely related [71-73].
4.3 Education and training for pharmacists to lessen stigma around mental health
The presence of suboptimal views surrounding mental illness as well as the lack of pharmacists’ professionalism themselves when providing services to patients with mental illness indicates an urgent need for change in teaching strategies in the sphere of mental health. Studies emphasize the necessity of extending the primary syllabus that mainly contains the pharmacological and therapeutic aspects of psychotropic agents to include practical strategies for the reduction of stigma related to mental illness and the improvement of pharmacists’ efficacy in the provision of mental health services. different kinds of anti-stigma campaigns have proven their effectiveness. One of the most effective in combating stigma are contact-based interventions – techniques which facilitate contact between people and those suffering from mental disorders [72-74].
Educational interventions based on contacts are influenced by Allport’s theory which emphasizes that mere bringing people together does not improve intergroup relations; there must be some prerequisites in terms of stigma reduction. As per the Allport’s intergroup contact theory: equal status of participants, common goals, intergroup collaboration, and endorsement of authorities or the social context are some prerequisites of decreasing prejudice. Many of these conditions can be integrated into the training of pharmacists and pharmacy students, such as establishing equal status. By including consumers of mental health in training programs as educators, they will be seen as academies instead of patients and sense of equality is achieved. It has been reported that contact-based interventions in pharmacy, nursing and medical education, where mental health consumers and students engage for the purpose of interaction are on the same level, work well. It has been successful to reduce stigma in students by creating chances for students to manage contact in safe low-stakes situations [72,75-78]. This in turn raises the likelihood of the students performing these services in future upon qualifying as pharmacists. To promote the effective engagement of pharmacists in mental health care, it is crucial to target stigma barriers through more complex educational programs that include active participation with psychiatric patients. There is ample evidence supporting this method among pharmacy and medical students, however, there is insufficient management knowledge to help practice changing stigma in active healthcare staff [79]. The applicability of the results of such studies to healthcare professionals practicing in the community is also questionable. Furthermore, addressing the issue of mitigating stigma, more studies are needed to evaluate training programs set out for pharmacists concerning mental health interventions at different levels in their career development.
4.4 Elements influencing collaboration between pharmacist and physicians
The inclusion of pharmacists into these teams is however a work in progress and a key area of interest in research in pharmacy practice [80-83]. Models have been designed in order to explain the interactions in multidisciplinary health care, however the focus on specific functions of pharmacists in these structures is poor. Among such are the Bradley and McDonough [84] models which provide for progressive stages of pharmacist physician collaboration and treat them as a continuum from complete isolation to full collaboration [85]. The above models explain the stages of collaborative advancement in regard to several participants’ characteristics including their context and exchange. Further studies have also analysed the introduction of other pharmacy care services such as qualitative studies that sought to understand factors that inhibited or motivated collaboration from new angles that were pharmacists and doctors. The barriers embracing the collaboration included the perceived worth of the collaboration, the trust and understanding between the two parties, the confusion of the roles played, the interests of the pharmacists and the professional domain of the physicians. Interprofessional care models as mentioned above, integrate these factors as barriers and drivers and serve.
Focusing on the pharmacists’ and physicians’ intent to collaborate the following analysis of the obstacles is according to Ajzen’s theory of planned behaviour, which predicts behavioural intentions. These include perception on the behaviour, attitude towards the behaviour, perceived behavioural control as well as perceived norms. In the array of studies focusing on physician-pharmacist collaboration, willingness of those professions to engage in collaborative partnership depends on their beliefs toward such forms of collaboration and was found to be influenced by the perceived value of the collaboration, degree of trust between the two professions [81,86-87].
Such negative or neutral assessments about working together with other professional groups from the health system can act as a barrier to participation for practitioners [87]. More likely you will find people who are resistant to the idea, especially in teams that have not had experience working this way. Hence, joint interprofessional continuing education and meetings in person at collective practice levels are indispensable. These kinds of initiatives can generate a positive experience with interprofessional collaboration for pharmacists and physicians overall, reducing conflict, driving better understanding across disciplinary roles toward shared goals; improved communication based on ongoing dialogue rather than information transfer alone; and trust that will be valuable in times when members feel they are working at cross purposes. Collaboration is also driven by a variety of other external factors. [80-81,83,86,88] For example: co-location of pharmacists and physicians; support from professional or governmental bodies; legislative mandates for shared access to patient records; financial incentives for provision of professional services all help create the pre-conditions in which collaboration can thrive. Consideration of these factors represents an important part in the design of novel care models to better incorporate pharmacists as members of multidisciplinary teams providing more consolidated mental health services [89].

Figure 5: Facilitators and barriers in pharmacy mental health services
The current review has demonstrated that pharmacists have several necessary competencies that are required in mental healthcare practice. This entails task such as, medication therapy management, providing prescribing physicians with information on available medications, educating patients on how to use their medicines, and encouraging the use of the appropriate medications. Nevertheless, a lot of the studies assessing these roles are uncontrolled, undermining the quality of evidence provided. For this reason, future evaluations should use study designs that are able to measure the impact of such services in a more direct fashion. Pharmacists’ roles in collaborative drug therapy management within a multidisciplinary team and avoiding polypharmacy in the use of multiple antipsychotics is also quite encouraging as preliminary evidence supports the same. More studies should, however, have well defined study designs, better evaluation techniques and longer durations of follow up. Further, developing and evaluating specific multifaceted pharmacist services for individual patients may provide more evidence on promoting medication adherence.
Lastly, evidence-based pharmacy service adoption could be enhanced by implementing strategies and training methods that target individual barriers, such as those around addressing psychological aspects of mental health.
REFERENCES










Sanika Latpate*, Naziya Munawar, Sneha Mane, Moksha Patil, Simra Momin, Ashiya Mulla, Pranali Patil, Neha Patil, Prajkta Mendgule, Namrata Mardane, The Psychopharmacist’s Paradigm: Navigating Treatment, Adherence, And Stigma in Mental Health Care Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2607-2625 https://doi.org/10.5281/zenodo.17639058
 10.5281/zenodo.17639058
10.5281/zenodo.17639058
