
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Samarth College of Pharmacy, Belhe, Pune, Maharashtra, India, 412410
Pharmacogenomics testing has already demonstrated clinical success in predicting severe toxicities associated with drugs like abacavir, carbamazepine, warfarin, and irinotecan. However, challenges such as population-specific genetic diversity, ethical issues, cost, and lack of infrastructure limit widespread implementation. Future prospects involve integrating pharmacogenomics with artificial intelligence, polygenic risk scoring, and real-time clinical decision systems to establish precision medicine as a healthcare standard. This review explores the genetic basis of ADRs, key biomarkers, clinical applications, and future trends that position pharmacogenomics as an indispensable tool for improving drug safety and efficacy. Clinical effectiveness in anticipating serious toxicities linked to medications such as irinotecan, warfarin, carbamazepine, and abacavir has previously been shown by pharmacogenomics testing. Widespread adoption is, however, constrained by obstacles such population-specific genetic variability, moral dilemmas, expense, and infrastructural deficiencies. In order to make precision medicine the norm in healthcare, future prospects include combining pharmacogenomics with artificial intelligence, polygenic risk assessment, and real-time clinical decision systems. The genetic foundation of adverse drug reactions (ADRs), important biomarkers, clinical uses, and emerging trends are all examined in this study, which establishes pharmacogenomics as a crucial instrument for enhancing medication safety and effectiveness.
One of the most significant problems in contemporary healthcare is the occurrence of adverse drug reactions (ADRs), which are undesirable, unanticipated reactions to drugs given at therapeutic dosages1. ADRs account for between 5–10% of hospital admissions and 3–7% of hospital fatalities, making them one of the world's top causes of morbidity and mortality, according to the World Health Organization (WHO). In addition to endangering patient safety, these responses place a significant financial strain on healthcare systems since they necessitate longer hospital stays, more diagnostic procedures, and alternative therapies2-3.
Despite continual breakthroughs in medication research and development, interindividual heterogeneity in treatment response continues. When given the same dosage of a medicine, two people frequently show quite varied therapeutic results; one may achieve the intended efficacy, while the other may suffer from severe toxicity4. This heterogeneity derives from a mix of genetic, physiological, and environmental variables. Genetic variations are widely acknowledged as the most important drivers of medication response, even if age, nutrition, illness status, and drug interactions all contribute to variability. Understanding how a person's genetic composition affects drug metabolism, transport, and mechanism of action is the main goal of the new science of pharmacogenomics, which straddles the divide between genetics and pharmacology5.
A branch of pharmacogenetics called pharmacogenomics studies how changes in the genome impact pharmacokinetics (drug-target interactions) and pharmacokinetics (absorption, distribution, metabolism, and excretion). Clinicians can forecast whether a patient will react well to a certain medication or have harmful side effects by integrating pharmacogenomics data6-7. Genetic variations in cytochrome P450 (CYP450) enzymes, for example, have been widely connected to changes in the metabolism of medications that are often administered, including cardiovascular medicines, antidepressants, and antiepileptic’s. Similarly, intracellular drug concentrations can be greatly impacted by differences in genes producing solute carriers or drug transporters like ABCB18-9.
Pharmacogenomics has therapeutic significance that goes beyond effectiveness prediction; it is essential for averting adverse drug reactions. It is now recognized that a sizable percentage of Type B (idiosyncratic) ADRs, which are unexpected and unrelated to dosage, have hereditary roots10. For instance, those with the HLA-B15:02* allele are more likely to develop Stevens-Johnson syndrome while using carbamazepine, and those with the HLA-B57:01* allele are more likely to have hypersensitivity to the antiretroviral medication abacavir .Because of these findings, genetic testing is now required before starting treatment with these drugs, indicating the therapeutic potential of pharmacogenomics in improving medication safety11-12.
The significance of pharmacogenomics biomarkers has been acknowledged by regulatory bodies worldwide, including the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) 13. More than 300 medications with related genetic data that help with dosage or treatment selection are listed in the FDA's pharmacogenomics biomarker table (FDA, 2023). These include medications with known gene–drug interactions, such as irinotecan (UGT1A1), thiopurines (TPMT), and warfarin (CYP2C9, VKORC1)14-15.
Furthermore, the idea of personalised medicine, which involves adjusting treatment to each patient's unique genetic profile, is becoming more and more popular. Physicians can enhance treatment results, lower the frequency of adverse drug reactions, and optimize therapy selection by integrating pharmacogenomics data into clinical decision-making16. With the goal of replacing the conventional "one-size-fits-all" method with a more focused and evidence-based approach, the move towards customised therapy marks a revolutionary movement in healthcare. However, there are obstacles to integrating pharmacogenomics into standard practice, such as exorbitant testing expenses, a lack of knowledge among physicians, and moral worries over the privacy of genetic data17. However, the detection of gene–drug interactions has been hastened by technology improvements, especially genome-wide association studies (GWAS) and next- generation sequencing (NGS), making pharmacogenomics testing more practical and inexpensive18.
GENETIC BASIS OF ADVERSE DRUG REACTIONS:
Variations in genes related to drug metabolism, transport, and immune responses constitute the genetic foundation of adverse drug reactions (ADRs). These differences, which are frequently single nucleotide polymorphisms (SNPs), affect pharmacokinetic and pharmacodynamic mechanisms, changing the toxicity and effectiveness profiles of drugs19.
A key player in drug metabolism is the cytochrome P450 (CYP) superfamily. Individual variations in medication clearance are caused by genetic variations in CYP2D6, CYP2C9, and CYP2C19. Standard amounts of codeine, for instance, may be harmful to CYP2D6 weak metabolizers, whereas ultra-rapid metabolizers turn excessive codeine into morphine, which causes respiratory depression. Likewise, CYP2C9 variations (CYP2C92* and CYP2C93*) affect the metabolism of warfarin and put individuals at risk for bleeding20.
Drug distribution and elimination are influenced by transporter genes like SLCO1B1 and ABCB1 (P-glycoprotein). SLCO1B1 polymorphisms are linked to a higher incidence of myopathy brought on by statins, especially simvastatin21.
Changes in drug targets may result in changes to therapeutic sensitivity or resistance. For example, VKORC1 polymorphisms alter warfarin sensitivity, requiring genotype-based dosage modifications.
One important factor influencing immune-mediated ADRs is the human leukocyte antigen (HLA) system. Hypersensitivity responses to abacavir, carbamazepine, and allopurinol are closely associated with alleles such as HLA-B57:01*, HLA-B15:02*, and HLA-A31:01*22.
PHARMACOGENOMICS BIOMARKERS IN ADR PREDICTION:
Pharmacogenomic biomarkers are quantifiable genetic markers that forecast a person's propensity to adverse medication reactions and therapeutic response. More than 300 gene-drug combinations with proven clinical significance are on the FDA-approved pharmacogenomic biomarker list (FDA, 2023).
These indicators make it easier to customise therapy and optimize dosage. Safe and efficient medication prescription is made possible by clinical implementation through standards such as the Clinical Pharmacogenetics Implementation Consortium (CPIC) 23-24.
TECHNIQUES USED IN PHARMACOGENOMICS STUDIES:
Pharmacogenomic research uses a variety of molecular and computational techniques to find and confirm the genetic causes of adverse drug reactions.
Genotyping Techniques:
Real-time PCR, restriction fragment length polymorphism (RFLP), and polymerase chain reaction (PCR) allow for the identification of known SNPs. Because they make it possible to identify precise genetic variations—in particular, single nucleotide polymorphisms (SNPs)—that affect medication response and metabolism, genotyping techniques are essential to pharmacogenomics. Polymerase chain reaction (PCR), restriction fragment length polymorphism (RFLP) analysis, and real-time PCR (quantitative PCR) are frequently employed genotyping techniques. Small DNA segments containing target SNPs can be amplified very well using PCR-based techniques, and the results can be examined to ascertain a person's genotype. In RFLP, DNA is digested using certain restriction enzymes that cut at known polymorphic locations, resulting in fragments of different lengths that can be sorted and visualized using gel electrophoresis. In contrast, real-time PCR produces faster and more precise findings by using fluorescent probes to identify and measure certain alleles as amplification proceeds30-31.
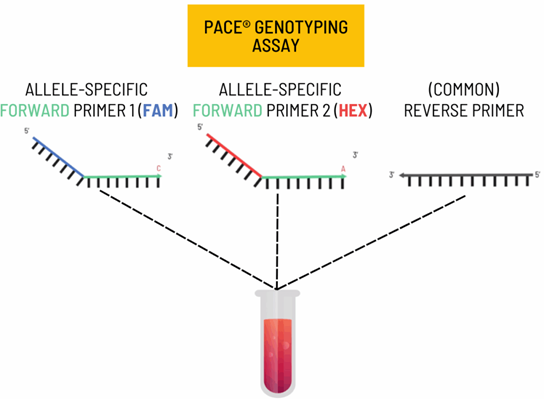
Fig.1: Genotyping Techniques
Sequencing:
By enabling the identification of both known and unknown genetic variations linked to drug response, sequencing technologies offer a more thorough method of comprehending a person's genetic composition. Pharmacogenomics research has been transformed by whole-genome sequencing (WGS) and next-generation sequencing (NGS), which allow for the large-scale and high-throughput examination of genetic data. WGS identifies every variation in a person's genome, including SNPs, insertions, deletions, and structural alterations that could impact medication metabolism and treatment results. On the other hand, NGS provides a variety of sequencing choices, including focused gene panels that concentrate on particular pharmacogenes like CYP2D6, TPMT, or VKORC1, or whole-exome sequencing, which only targets coding regions. Comprehensive genetic profiling is possible using whole-genome sequencing (WGS) and next-generation sequencing (NGS) 25.
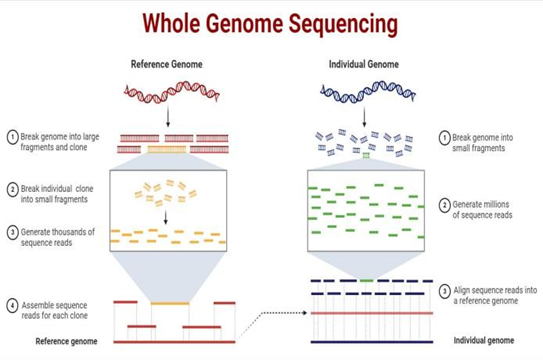
Fig.2: whole-genome sequencing (WGS)
Genome-wide association studies (GWAS):
Find new loci linked to medication response or adverse drug reactions (ADRs) using genome-wide association studies (GWAS). In contrast to targeted genotyping, which looks at known variants, GWAS scans millions of people's genomes to find SNPs that are more common in patients who show a particular toxicity or therapeutic response. Many new pharmacogenetics indicators associated with diseases like thiopurine toxicity, statin-induced myopathy, and warfarin sensitivity have been found as a result of this objective, data-driven approach. GWAS provides important insights into the molecular reasons behind individual variability in drug effects by identifying candidate genes and pathways involved in pharmacodynamics or pharmacokinetics through the analysis of huge datasets of genetic and clinical data38-39.
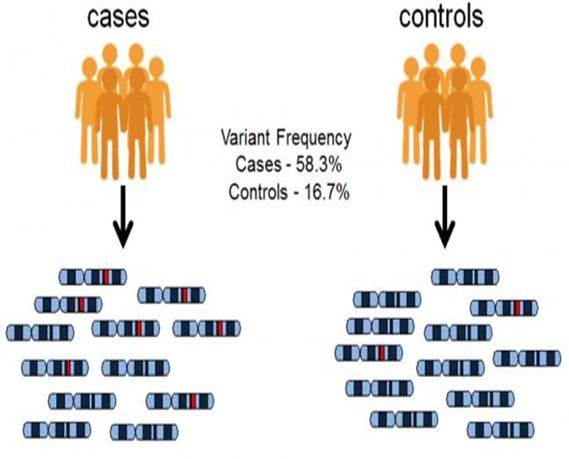
Fig.3: Genome-wide association studies (GWAS)
Bioinformatics Tools:
Curated gene-drug data for clinical interpretation is available from databases such as PharmGKB, dbSNP, and CPIC. In order to evaluate genetic data and convert it into information that can be used in therapeutic settings, bioinformatics tools are essential. Comprehensive resources that relate genetic variations to medication metabolism, efficacy, and toxicity can be found in curated databases like CPIC (Clinical Pharmacogenetics Implementation Consortium), dbSNP (Database of Single Nucleotide Polymorphisms), and PharmGKB (Pharmacogenomics Knowledgebase). PharmGKB helps medical professionals make evidence-based treatment decisions by gathering and annotating pharmacogenomics data, such as gene–drug correlations, clinical guidelines, and variant summaries. As a resource for genetic research and clinical studies, the National Centre for Biotechnology Information (NCBI) maintains the dbSNP database, which lists millions of SNPs and minor genetic variations present in many populations40-41.
Fig.4: Bioinformatics Tools
CLINICAL APPLICATIONS AND CASE STUDIES:
Abacavir Hypersensitivity:
Hypersensitivity responses are essentially eliminated by pre- treatment HLA-B*57:01 testing. Pharmacogenetics testing for HLA-B*57:01 is now required prior to beginning abacavir therapy in order to avoid this. Abacavir can be safely administered to patients who test negative under regular clinical supervision, but it should never be given to patients who test positive25. Abacavir-induced hypersensitivity responses have all but disappeared since pre-treatment HLA-B*57:01 screening was used, marking a significant advancement in clinical pharmacogenomics and precision medicine26.
Warfarin Dosing:
CYP2C9 and VKORC1 genotyping aids in dosage optimization and bleeding reduction. Due to the narrow therapeutic index of the commonly used oral anticoagulant warfarin, even slight dose changes might result in thrombosis or bleeding. VKORC1 and CYP2C9 are two important genetic variables that have a considerable impact on warfarin dose needs and response27. The active S-enantiomer of warfarin is metabolized by the CYP2C9 enzyme, and people with reduced-function alleles such CYP2C92 or CYP2C93 have slower drug metabolism. Standard warfarin dosages may therefore result in elevated plasma levels and a higher risk of bleeding. However, drug sensitivity is impacted by the VKORC1 gene, which genes for the vitamin K epoxide reductase complex subunit 1 (the pharmacological target of warfarin) 28.
Carbamazepine Toxicity:
Severe cutaneous responses can be avoided by screening for HLA- B15:02*. In people who are genetically predisposed, the antiepileptic and mood-stabilizing medication carbamazepine can result in severe cutaneous adverse reactions (SCARs), including toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS)29. The HLA-B*15:02 allele, which is more common in those of East and Southeast Asian heritage, is closely associated with these potentially fatal reactions. When the HLA-B15:02 molecule presents drug-modified peptides, the allele predisposes people to an abnormal immune response that activates cytotoxic T cells that target mucosal and skin tissues. Furthermore, a wider range of carbamazepine hypersensitivity syndromes, such as drug rash with eosinophilia and systemic symptoms (DRESS), have been linked to another variant, **HLA-A31:01**30.
Thiopurines Toxicity:
In leukemia and autoimmune treatment, TPMT genotyping avoids myelosuppression. Thiopurine medications, such as azathioprine, 6-mercaptopurine, and thioguanine, are frequently used to treat autoimmune diseases, leukaemia, and inflammatory bowel disease31. However, there is a considerable danger of myelosuppression when using them, which can cause pancytopenia and potentially fatal infections in those who are genetically susceptible. The main cause of this toxicity is decreased or nonexistent activity of the enzyme thiopurines S-methyltransferase (TPMT), which inactivates thiopurine metabolites. In hematopoietic cells, people with homozygous or compound heterozygous loss- of-function TPMT alleles build up too many cytotoxic thioguanine nucleotides, which suppresses bone marrow. Similarly, impaired detoxification of thiopurine metabolites and increased toxicity risk are caused by mutations in the NUDT15 gene, which are more prevalent in East Asian and Hispanic populations32.
These examples show how pharmacogenomic testing may be used in real-world clinical settings to improve patient safety26-29.
CHALLENGES AND LIMITATIONS:
Pharmacogenomics encounters obstacles in spite of encouraging results:
In order to deploy pharmacogenomics in a fair and efficient manner, these problems must be resolved34-40.
RECENT ADVANCES AND FUTURE PERSPECTIVES:
By forecasting ADR risk from intricate datasets, recent advancements in artificial intelligence (AI) and machine learning are transforming pharmacogenomics35. Multi-gene ADR risk assessment is now possible because to prediction algorithms and polygenic risk scores (PRS). Post-marketing safety surveillance is improved by combining pharmacogenomics and pharmacovigilance data36. Additionally, wearable biosensors and point-of-care genetic testing might soon offer real-time medication response monitoring. Global precision medicine is being accelerated by collaborative efforts like the All of Us Research Program and the 100,000 Genomes Project, which are creating enormous genetic datasets41-52.
CONCLUSION:
Forecasting ADR risk from intricate datasets, recent advancements in artificial intelligence (AI) and machine learning are transforming pharmacogenomics. Multi-gene ADR risk assessment is now possible because to prediction algorithms and polygenic risk scores (PRS). Post-marketing safety surveillance is improved by combining pharmacogenomics and pharmacovigilance data. Additionally, wearable biosensors and point-of-care genetic testing might soon offer real-time medication response monitoring. Global precision medicine is being accelerated by collaborative efforts like the All of Us Research Program and the 100,000 Genomes Project, which are creating enormous genetic datasets.
REFERENCE





Vaishali Bhutambare, Ajay Bhagwat, Ankita Bhapkar, Shivani Zodge, Sajiya Momin, Role of Pharmacogenomics in Predicting Adverse Drug Reactions, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4010-4020. https://doi.org/10.5281/zenodo.17711928
 10.5281/zenodo.17711928
10.5281/zenodo.17711928