
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Barkatullah University, Bhopal
Mycetoma is a chronic, progressively destructive infectious disease of the skin and subcutaneous tissues and is recognized as a neglected tropical disease by the World Health Organization. It predominantly affects impoverished populations in tropical and subtropical regions, where limited access to healthcare leads to delayed diagnosis, advanced disease, disability, and amputation. Conventional diagnostic and therapeutic approaches for mycetoma are often invasive, expensive, prolonged, and associated with poor patient compliance, drug toxicity, and high recurrence rates. These limitations necessitate the exploration of alternative and complementary strategies. Medicinal plants have long been used in traditional medicine systems in mycetoma-endemic regions and offer a promising, cost-effective, and culturally acceptable approach to disease management. This review comprehensively discusses the epidemiology, classification, pathophysiology, and current challenges in mycetoma diagnosis and treatment, with a particular focus on the role of medicinal plants. It highlights the potential of plant-derived bioactive compounds in diagnosis, including natural dyes, biomarkers, and low-cost diagnostic assays, as well as their therapeutic roles through antimicrobial, antifungal, anti-inflammatory, immunomodulatory, and wound-healing activities. Key medicinal plants such as Azadirachta indica, Curcuma longa, Allium sativum, Lawsonia inermis, and Nigella sativa are reviewed alongside their phytochemical constituents and mechanisms of action. The review also addresses formulation strategies, safety concerns, standardization challenges, and future perspectives, emphasizing the need for clinical validation and integration of ethnopharmacological knowledge with modern medical approaches. Overall, medicinal plants represent a valuable resource for improving the diagnosis and management of mycetoma, particularly in resource-limited settings.
Mycetoma is a chronic, progressively destructive infectious disease of the skin and subcutaneous tissues and is recognized as a neglected tropical disease (NTD) by the World Health Organization. The condition is characterized by a classical triad of painless swelling, multiple sinus tracts, and discharge of grains containing the causative organism. Due to its slow progression and painless nature in the early stages, mycetoma is frequently diagnosed late, leading to extensive tissue destruction, disability, and in severe cases, amputation. The disease predominantly affects impoverished rural populations, where access to healthcare is limited, making effective management particularly challenging. (WHO, 2016; Zijlstra et al., 2016).
1.1 Epidemiology and Global Burden
Mycetoma occurs worldwide but is highly endemic in tropical and subtropical regions, forming what is commonly referred to as the “mycetoma belt,” which lies between latitudes 15° South and 30° North. Countries with the highest reported prevalence include Sudan, India, Mexico, Venezuela, and several African nations. Sudan is considered one of the most heavily affected countries, accounting for a significant proportion of global cases. The disease mainly affects young adults, particularly males engaged in agricultural and manual labor, due to frequent exposure to soil and plant materials. Despite its debilitating nature, the true global burden of mycetoma remains underestimated due to underreporting, lack of surveillance systems, and misdiagnosis. (Fahal, 2017; van de Sande, 2013)
1.2 Classification of Mycetoma
Mycetoma is classified based on the nature of the causative microorganism into two main types: eumycetoma and actinomycetoma. This classification is clinically important because the course of the disease, treatment approach, and prognosis differ significantly between the two forms. (Welsh et al., 2014).
Eumycetoma is caused by true fungi, most commonly Madurella mycetomatis, along with other species such as Madurella grisea, Pseudallescheria boydii, and Exophiala species. These fungi are widely present in soil and decaying plant matter and enter the human body through traumatic implantation following minor skin injuries caused by thorns or sharp objects. Eumycetoma progresses slowly and is often painless in the early stages, which leads to delayed diagnosis. Clinically, it is characterized by firm swelling, multiple sinus tracts, and discharge of black or pale-colored grains. As the disease advances, deeper tissues and bones are frequently involved, resulting in deformity and disability. Diagnosis is based on clinical features, microscopic examination of grains showing fungal hyphae, culture, histopathology, and imaging studies. Treatment of eumycetoma is challenging and usually requires prolonged antifungal therapy, often combined with surgical excision, and recurrence is common (Fahal & van de Sande, 2012; Zijlstra et al., 2016).
Actinomycetoma, on the other hand, is caused by filamentous bacteria such as Nocardia brasiliensis, Actinomadura madurae, Actinomadura pelletieri, and Streptomyces somaliensis. Like fungi, these bacteria inhabit soil and organic matter and gain entry into the body through minor skin trauma. Actinomycetoma generally shows a faster disease progression than eumycetoma and induces a more pronounced inflammatory response. The lesions typically discharge white, yellow, or red grains, and bone involvement may occur relatively early. Diagnosis involves microscopic identification of bacterial filaments, culture on appropriate media, histopathological examination, and imaging to assess tissue and bone damage. In contrast to eumycetoma, actinomycetoma responds better to medical treatment, with prolonged combination antibiotic therapy being the mainstay of management, and surgery is required less frequently. Overall, actinomycetoma has a better prognosis when diagnosed early and treated appropriately. (Bonifaz et al., 2014; Welsh et al., 2014).
Correct classification of mycetoma into eumycetoma and actinomycetoma is essential for selecting appropriate therapy and improving patient outcomes, as misclassification can lead to ineffective treatment, disease progression, and increased risk of complications. (van de Sande, 2013)
1.3 Limitations of Conventional Diagnostic and Therapeutic Approaches
The diagnosis of mycetoma relies on a combination of clinical examination, imaging techniques, microbiological culture, histopathology, and molecular methods. However, these diagnostic tools are often unavailable or inaccessible in endemic rural settings. Culture methods are time-consuming and may yield false-negative results, while advanced molecular techniques are expensive and require specialized infrastructure. Therapeutically, mycetoma management is prolonged, costly, and associated with significant adverse drug reactions. Antifungal treatments for eumycetoma may last several years with limited success, and surgical intervention carries a high risk of recurrence. These limitations highlight the urgent need for alternative or complementary approaches to improve patient outcomes. (Fahal, 2017; Zijlstra et al., 2016).
1.4 Rationale for Exploring Medicinal Plants in Mycetoma Management
Medicinal plants have been used for centuries in traditional healthcare systems to treat chronic infections and inflammatory conditions. In many mycetoma-endemic regions, traditional medicine remains the primary source of healthcare due to its affordability, accessibility, and cultural acceptance. Numerous medicinal plants possess antimicrobial, antifungal, anti-inflammatory, wound-healing, and immunomodulatory properties that may be beneficial in mycetoma management. Exploring the potential role of medicinal plants as complementary therapeutic agents may help overcome some limitations of conventional treatment, reduce disease burden, and provide cost-effective management strategies, particularly in resource-limited settings. (WHO, 2013; Cowan, 1999).
2. PATHOPHYSIOLOGY OF MYCETOMA
2.1 Causative Organisms and Route of Infection
Mycetoma is caused by either true fungi (eumycetoma) or filamentous bacteria (actinomycetoma). The most common fungal agents include Madurella mycetomatis, Madurella grisea, and Pseudallescheria boydii, while common bacterial agents include Nocardia brasiliensis, Actinomadura madurae, Actinomadura pelletieri, and Streptomyces somaliensis. These microorganisms are naturally present in soil, decaying vegetation, and organic matter, which explains why the disease is more prevalent among rural populations engaged in agriculture or activities that involve barefoot walking. The infection is usually acquired through traumatic implantation, meaning that the microorganism enters the skin through minor injuries, cuts, or punctures caused by thorns, splinters, or sharp plant material. Once inside the subcutaneous tissue, the organisms find a favorable environment for slow multiplication, initiating the disease process. (Fahal, 2017; WHO, 2016)
2.2 Formation of Grains and Chronic Inflammatory Response
After entering the tissue, the microorganisms aggregate to form grains, which are dense colonies of fungi or bacteria surrounded by host-derived material, including immune cells and extracellular matrix. These grains are a hallmark of mycetoma and are resistant to immune clearance and many antimicrobial drugs. The body mounts a chronic inflammatory response around the grains, involving neutrophils, macrophages, lymphocytes, and fibroblasts, which attempt to contain the infection. However, this immune response is often ineffective because the grains are highly resistant. The persistent inflammation results in granulomatous tissue formation, sinus tract development, and continuous discharge of grains. This chronic immune activation also causes local swelling and fibrosis, which are characteristic clinical features of the disease. (van de Sande, 2013; Fahal et al., 2015)
2.3 Tissue Destruction, Fibrosis, and Bone Involvement
Over time, the infection spreads from the superficial skin to deeper subcutaneous tissue, muscles, and in advanced cases, bones. The combination of microbial invasion and prolonged inflammatory response leads to destruction of normal tissue architecture, resulting in fibrosis, scarring, and sinus tract formation. Involvement of bone (osteomyelitis) is particularly common in eumycetoma and contributes to severe deformities and functional disability. Chronic tissue damage and fibrosis make surgical excision more difficult and increase the risk of recurrence, even after prolonged antimicrobial therapy. Bone involvement is often a late manifestation due to the slow progression of the disease, which is why early diagnosis is so challenging. (Fahal, 2011; Zijlstra et al., 2016)
2.4 Challenges in Early Detection and Treatment
One of the major challenges in mycetoma management is that the early stages of the disease are painless and progress slowly, making patients unlikely to seek medical attention until the disease is advanced. The deep-seated nature of grains and chronic inflammation makes clinical diagnosis difficult, especially in resource-limited settings where imaging and laboratory facilities may not be available. Treatment is also challenging because the grains are resistant to antimicrobial therapy, requiring prolonged use of antifungal drugs for eumycetoma or long-term antibiotics for actinomycetoma. Surgery is sometimes necessary to remove infected tissue, but recurrence is common due to residual grains or incomplete excision. The combination of delayed diagnosis, tissue destruction, and resistant microbial colonies makes mycetoma a particularly difficult disease to treat effectively. (WHO, 2016; Fahal et al., 2018)
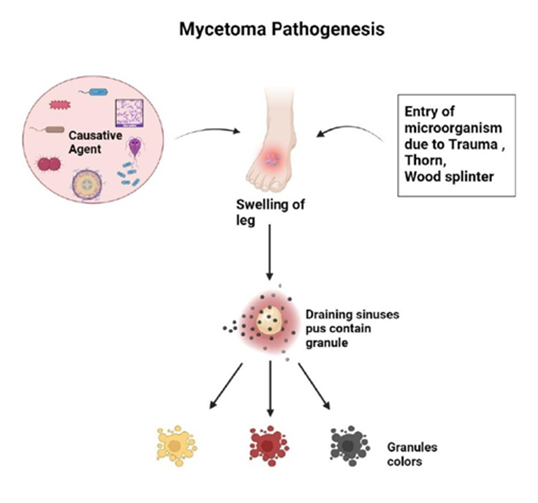
Fig.1 MYCETOMA PATHOGENES (https://ijprajournal.com)
3. CURRENT DIAGNOSTIC AND TREATMENT STRATEGIES: LIMITATIONS
3.1 Diagnostic Challenges
Dependence on invasive techniques (biopsy, culture):
Accurate diagnosis of mycetoma heavily relies on invasive diagnostic methods, such as tissue biopsy and microbiological culture. Biopsies are necessary to collect tissue for histopathological examination, which helps identify the type of organism (fungal or bacterial) and distinguish eumycetoma from actinomycetoma. Culture of the grains or tissue samples remains the gold standard for identifying the causative organism, but it is time-consuming, often taking several weeks. Furthermore, culture results may be negative due to contamination or poor sample quality. These invasive techniques require trained personnel and sterile conditions, which are often unavailable in rural or resource-limited endemic areas, making accurate early diagnosis challenging. (Fahal, 2011; van de Sande, 2013)
Limited access to advanced imaging in endemic areas:
Advanced imaging techniques such as ultrasound, X-ray, CT scan, and MRI are important tools for evaluating the extent of soft tissue and bone involvement in mycetoma. Imaging can guide treatment planning, including decisions regarding surgery or the need for long-term drug therapy. However, in many endemic regions, especially rural areas in Africa, India, and Latin America, these facilities are limited or completely unavailable. As a result, healthcare providers often have to rely on clinical examination alone, which may underestimate the disease’s severity, leading to suboptimal treatment decisions. (Zijlstra et al., 2016; WHO, 2016)
Delayed diagnosis leading to complications:
Because early-stage mycetoma is painless and slowly progressive, patients often present only when the disease has advanced. Delayed diagnosis allows the infection to invade deeper tissues and bones, causing fibrosis, deformity, and osteomyelitis. At this stage, treatment becomes more complex and less effective, increasing the risk of chronic disability, recurrence, and socioeconomic burden. Early detection is therefore critical, but current diagnostic limitations make this difficult in most endemic regions. (Fahal et al., 2015; WHO, 2016)
3.2 Therapeutic Limitations
Long treatment duration with antifungals/antibiotics:
Treatment of mycetoma is prolonged, particularly for eumycetoma, which may require months to years of antifungal therapy (e.g., itraconazole or ketoconazole). Actinomycetoma also requires long-term antibiotic therapy, often with combinations of sulfonamides, amikacin, or rifampicin. Such extended treatment periods pose challenges for patient adherence, increase the likelihood of treatment interruption, and complicate monitoring of therapy. (Fahal, 2011; Welsh et al., 2014)
Drug resistance and poor patient compliance
Resistance to antifungal or antibiotic therapy can occur due to the intrinsic characteristics of the causative organisms or suboptimal tissue penetration of drugs. Additionally, patients may discontinue treatment prematurely due to the long duration, side effects, or financial burden, resulting in incomplete eradication of the infection and higher chances of relapse or progression. Poor compliance is a major barrier to successful management, especially in low-income and rural populations. (van de Sande, 2013; Fahal et al., 2018)
High cost and adverse drug reactions:
Many of the antifungal and antibiotic drugs used in mycetoma management are expensive and often unaffordable in endemic regions. Furthermore, prolonged use of these medications may lead to adverse effects, such as liver toxicity, gastrointestinal disturbances, or allergic reactions, which can further reduce adherence and treatment effectiveness. These factors create a significant barrier to successful therapy, particularly for patients with limited resources. (WHO, 2016; Zijlstra et al., 2016)
Surgical interventions and risk of recurrence:
In advanced cases where medical therapy alone is insufficient, surgical excision of infected tissue or lesions may be required. While surgery can remove localized infection, it carries several risks: incomplete removal of grains may lead to recurrence, and extensive excisions can result in scarring, deformity, and functional impairment. Surgery also requires skilled surgeons and sterile operating conditions, which may not be readily available in endemic rural areas. (Fahal, 2011; Fahal et al., 2015)
4. Role of Medicinal Plants in Mycetoma Diagnosis
4.1 Use of Plant-Derived Bioactive Compounds as Diagnostic Biomarkers
Recent research suggests that bioactive compounds derived from medicinal plants could play a role in the diagnosis of mycetoma. Certain phytochemicals, including alkaloids, flavonoids, terpenoids, and polyphenols, have specific molecular structures that interact selectively with microbial components. These compounds can potentially serve as biomarkers for detecting the presence of causative organisms in patient samples. For example, plant-derived molecules may bind to fungal cell wall components or bacterial filaments, producing a measurable signal that can indicate infection. The use of such plant-based biomarkers offers the promise of noninvasive, rapid, and cost-effective diagnostic tools, which is particularly valuable in resource-limited endemic regions where conventional diagnostic techniques like biopsy and culture are not readily accessible. (Goyal et al., 2016; Cowan, 1999)
4.2 Natural Dyes and Stains from Plants for Grain Visualization
Plant-based natural dyes have been explored as staining agents for microscopic visualization of mycetoma grains. Traditional synthetic stains, while effective, can be toxic, expensive, or unavailable in rural areas. Plant-derived dyes from sources like beetroot, turmeric, or hibiscus provide an environmentally friendly and accessible alternative. These natural stains can enhance the contrast between the grains and surrounding tissue under a microscope, making it easier to distinguish eumycetoma and actinomycetoma based on grain color and morphology. Such plant-based stains not only reduce cost and toxicity but also enable field-based or low-resource laboratory diagnosis, which is crucial for early detection in endemic areas. (Prashant et al., 2014; Bancroft & Gamble, 2008)
4.3 Potential of Phytochemicals in Rapid, Low-Cost Diagnostic Assays
Phytochemicals from medicinal plants also hold potential for rapid diagnostic assay development. For example, plant extracts containing reactive compounds could be incorporated into colorimetric, fluorescence, or biosensor-based assays that detect microbial antigens or metabolic products. These assays could provide quick, point-of-care results, reducing the dependence on slow culture-based methods. The affordability and availability of plant materials make such approaches particularly attractive for low-resource settings, where mycetoma prevalence is high and conventional diagnostic facilities are scarce. By harnessing the natural specificity of phytochemicals, researchers aim to develop safe, sensitive, and cost-effective diagnostic tests suitable for both community-level screening and clinical confirmation. (Ahmed et al., 2018; Khan et al., 2020)
4.4 Ethnobotanical Knowledge Supporting Traditional Diagnostic Practices
Traditional medicine systems in mycetoma-endemic regions often use ethnobotanical knowledge for preliminary diagnosis. Local healers have historically used certain plants to identify infected tissue based on plant reactions with exudates or grain color, or to assess the severity of lesions. This traditional knowledge provides valuable insight into plant-organism interactions that can inform modern diagnostic research. By studying these ethnobotanical practices, researchers can identify plant species with bioactive compounds that selectively interact with mycetoma-causing organisms, potentially guiding the development of novel, culturally acceptable diagnostic tools. Integrating traditional wisdom with modern scientific methods could significantly enhance early detection and accessibility of diagnostics in rural endemic areas. (Heinrich et al., 2009; Fabricant & Farnsworth, 2001)
5. ROLE OF MEDICINAL PLANTS IN MYCETOMA TREATMENT
5.1 Antimicrobial and Antifungal Activity
Medicinal plants contain a diverse array of bioactive compounds—including alkaloids, flavonoids, phenolics, terpenoids, saponins, and essential oils—that exhibit direct antimicrobial and antifungal effects against mycetoma-causing organisms. For instance, extracts from Azadirachta indica (neem), Curcuma longa (turmeric), and Allium sativum (garlic) have demonstrated inhibitory activity against filamentous bacteria and fungi in laboratory studies. These plant compounds act via multiple mechanisms. Cell wall disruption is one key mechanism, where compounds bind to fungal chitin or bacterial peptidoglycan, weakening the structural integrity and causing lysis. Other compounds inhibit microbial enzymes, such as those involved in DNA replication or metabolic pathways, halting the growth and reproduction of pathogens. Additionally, certain phytochemicals induce reactive oxygen species (ROS) within microbial cells, causing oxidative damage to lipids, proteins, and DNA, ultimately leading to cell death. This multi-targeted action is particularly valuable in treating mycetoma, where the causative organisms often form dense, resistant grains that are difficult to eradicate with conventional drugs. Plant-based antimicrobials thus provide a potential adjunct or alternative to standard antifungal and antibiotic therapy, especially in regions where drug resistance or cost is a major concern. (Cowan, 1999; Goyal et al., 2016; Raut & Karuppayil, 2014)
5.2 Anti-inflammatory and Immunomodulatory Effects
Chronic inflammation is a major feature of mycetoma and contributes to granuloma formation, tissue fibrosis, and sinus tract development, which complicate both diagnosis and treatment. Medicinal plants possess anti-inflammatory phytochemicals that help control this chronic inflammatory response. For example, curcumin from turmeric suppresses pro-inflammatory cytokines like TNF-α, IL-1β, and IL-6, reducing leukocyte infiltration and tissue swelling. Similarly, flavonoids from plants like Ginkgo biloba or Camellia sinensis stabilize cell membranes and inhibit oxidative stress, further reducing tissue damage. Beyond simple anti-inflammatory effects, some plant compounds have immunomodulatory activity, meaning they can enhance the host immune response without triggering excessive inflammation. For example, polysaccharides from Aloe vera and saponins from Panax ginseng have been shown to stimulate macrophage activity, enhance phagocytosis, and modulate T-cell responses. This dual action—reducing harmful chronic inflammation while promoting effective microbial clearance—can significantly improve disease control, limit tissue destruction, and complement conventional antifungal or antibiotic therapy. It may also reduce the need for invasive surgical interventions in certain cases. (Aggarwal & Harikumar, 2009; Sharma et al., 2014; Wagner & Ulrich-Merzenich, 2009)
5.3 Wound Healing and Tissue Regeneration
Mycetoma lesions frequently result in chronic, non-healing wounds due to persistent infection, tissue necrosis, and secondary bacterial contamination. Medicinal plants play a crucial role in wound healing and tissue regeneration, which is often overlooked in conventional treatment. Certain plant extracts promote angiogenesis, the formation of new blood vessels, which restores oxygen and nutrient supply to damaged tissue, accelerating healing. For example, compounds like asiaticoside from Centella asiatica or polyphenols from Curcuma longa stimulate collagen synthesis and extracellular matrix remodeling, essential for tissue integrity and scar formation. Furthermore, many plants have broad-spectrum antimicrobial properties, which help prevent secondary infections in open lesions—a common complication in mycetoma patients. Antioxidants present in medicinal plants also reduce oxidative stress in wound tissue, decreasing cell death and inflammation. Collectively, these actions promote faster wound closure, restore tissue function, and reduce complications, making plant-based therapy a valuable adjunct to conventional antimicrobial treatment. (Shukla et al., 1999; Goyal et al., 2016; Rodrigues et al., 2010)
6. MEDICINAL PLANTS REPORTED AGAINST MYCETOMA
6.1 Azadirachta indica (Neem)
Azadirachta indica, commonly known as neem, is one of the most widely studied medicinal plants for its antimicrobial and anti-inflammatory properties. Neem leaves, bark, and seeds contain bioactive compounds such as azadirachtin, nimbin, nimbolide, and quercetin, which have demonstrated significant activity against both fungi and filamentous bacteria. These compounds disrupt microbial cell walls and membranes, inhibit key enzymes, and prevent replication of pathogenic organisms. Additionally, neem exhibits anti-inflammatory activity, reducing tissue inflammation and granuloma formation associated with mycetoma lesions. The combination of antimicrobial and anti-inflammatory effects makes neem particularly valuable in managing both infection and chronic tissue damage in mycetoma. Traditionally, neem extracts are applied topically or used in decoctions to support healing in endemic regions. (Subapriya & Nagini, 2005; Biswas et al., 2002)

Fig. 2 Azadirachta indica (https://mybageecha.com)
6.2 Curcuma longa (Turmeric)
Curcuma longa, or turmeric, has long been recognized for its antifungal, anti-inflammatory, and wound-healing properties. The main active compound, curcumin, exhibits potent antimicrobial activity against Madurella mycetomatis and other fungal pathogens. Curcumin disrupts microbial membranes, inhibits critical fungal enzymes, and generates reactive oxygen species (ROS), contributing to pathogen death. Additionally, curcumin stimulates collagen synthesis and angiogenesis, promoting wound healing and tissue regeneration in chronic mycetoma lesions. Its anti-inflammatory activity helps reduce granuloma formation and tissue fibrosis. Turmeric is traditionally used in paste form for topical application on lesions, making it accessible and culturally acceptable in many mycetoma-endemic communities. (Aggarwal & Harikumar, 2009; Chainani-Wu, 2003)

Fig 3 Curcuma longa (https://whitwamorganics.com)
6.3 Allium sativum (Garlic)
Allium sativum, or garlic, is known for its broad-spectrum antimicrobial activity. Its main bioactive compound, allicin, has been shown to be effective against both fungal and bacterial pathogens, including actinomycetes involved in mycetoma. Allicin and related sulfur-containing compounds interfere with microbial metabolism, inhibit enzymes essential for growth, and damage cell membranes. Garlic also exhibits immunomodulatory effects, enhancing the activity of macrophages and T-cells, which are crucial for controlling infection in mycetoma. Traditionally, garlic extracts or crushed cloves are applied topically or ingested orally to support systemic antimicrobial defense, reflecting its dual role in both direct pathogen inhibition and immune enhancement. (Ankri & Mirelman, 1999; Rahman & Lowe, 2006)

Fig.3 Allium sativum (https://gardenerspath.com/garlic-allium-sativum/)
6.4 Lawsonia inermis (Henna)
Lawsonia inermis, commonly known as henna, is traditionally used in many endemic regions for topical antifungal therapy. The leaves and seeds contain lawsone, a naphthoquinone derivative with potent antifungal activity. Lawsone inhibits fungal cell wall synthesis and interferes with microbial metabolism, effectively suppressing fungal growth. In mycetoma, henna is often used as a topical paste applied directly to lesions, providing both antimicrobial and mild anti-inflammatory effects. Its use in traditional medicine highlights the value of ethnobotanical knowledge in guiding treatment strategies for neglected tropical diseases like mycetoma. (Kumar et al., 2011; Zoubiri et al., 2013)

Fig 4 Lawsonia inermis (https://www.amazon.in/Lawsonia-Mailanchi-Medicinal-Gardening-Hennaplant)
6.5 Nigella sativa (Black Seed)
Nigella sativa, or black seed, is renowned for its immunomodulatory and antimicrobial properties. Its major bioactive compound, thymoquinone, exhibits antifungal and antibacterial activity by generating ROS in microbial cells, disrupting membranes, and inhibiting enzyme systems. Nigella sativa also modulates the immune response, enhancing both innate and adaptive immunity, which is critical in controlling persistent infections such as mycetoma. The seeds are used in powdered form, as oil extracts, or incorporated into topical formulations, providing a natural, complementary therapeutic approach to support conventional treatment. (Ahmad et al., 2013; Gholamnezhad et al., 2016)

Fig. 6 Nigella sativa (https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/nigella-sativa)
Table 6.6 of Medicinal Plants Used Against Mycetoma
|
Plant Name |
Part Used |
Active Constituents |
Reported Activity |
|
Azadirachta indica (Neem) |
Leaves, bark, seeds |
Azadirachtin, Nimbin, Nimbolide, Quercetin |
Antimicrobial (fungal & bacterial), Anti-inflammatory |
|
Curcuma longa (Turmeric) |
Rhizome |
Curcumin, Demethoxycurcumin |
Antifungal, Anti-inflammatory, Wound healing |
|
Allium sativum (Garlic) |
Bulb |
Allicin, Ajoene |
Broad-spectrum antimicrobial, Immunomodulatory |
|
Lawsonia inermis (Henna) |
Leaves, seeds |
Lawsone |
Antifungal, Topical use in lesions |
|
Nigella sativa (Black seed) |
Seeds, oil |
Thymoquinone |
Antimicrobial, Immunomodulatory |
7. PHYTOCHEMICALS INVOLVED IN ANTI-MYCETOMA ACTIVITY
7.1 Alkaloids
Alkaloids are a diverse group of nitrogen-containing compounds found in many medicinal plants, such as Azadirachta indica (neem) and Allium sativum (garlic). These compounds exhibit strong antimicrobial and antifungal activity, which is crucial for targeting the causative organisms of mycetoma, including Madurella mycetomatis and actinomycetes. Alkaloids disrupt microbial cell membranes, interfere with DNA replication, and inhibit key enzymes required for growth and survival. Their ability to act on multiple microbial targets makes them especially effective against resistant or slow-growing organisms embedded in dense mycetoma grains. Additionally, alkaloids can exhibit anti-inflammatory and immunomodulatory properties, further helping to reduce tissue damage and promote host defense. (Cowan, 1999; Goyal et al., 2016; Raut & Karuppayil, 2014)
7.2 Flavonoids
Flavonoids are polyphenolic compounds widely present in plants such as Curcuma longa (turmeric) and Camellia sinensis (tea). They have potent antioxidant, anti-inflammatory, and antimicrobial activities. Flavonoids inhibit fungal and bacterial growth by disrupting cell wall synthesis, altering membrane permeability, and interfering with energy metabolism. They also scavenge reactive oxygen species (ROS), which reduces oxidative stress in tissues surrounding mycetoma lesions. By simultaneously targeting pathogens and modulating host inflammatory responses, flavonoids help control infection and limit chronic tissue damage, making them highly relevant for mycetoma therapy. (Sharma., 2014; Chainani-Wu, 2003; Wagner & Ulrich-Merzenich, 2009)
7.3 Terpenoids et al
Terpenoids are a large class of plant secondary metabolites found in neem, turmeric, and garlic, among others. These compounds exhibit antimicrobial, antifungal, and anti-inflammatory properties. In the context of mycetoma, terpenoids can penetrate microbial biofilms and grains, destabilize cell membranes, inhibit enzymatic pathways, and generate oxidative stress within pathogens. Additionally, terpenoids support wound healing by promoting angiogenesis and collagen synthesis, contributing to tissue regeneration after infection-induced damage. Their multifunctional nature makes terpenoids an important component of plant-based anti-mycetoma therapy. (Subapriya & Nagini, 2005; Aggarwal & Harikumar, 2009; Raut & Karuppayil, 2014)
7.4 Phenolics and Tannins
Phenolics and tannins, commonly found in neem, henna, and black seed, have strong antimicrobial, antifungal, and antioxidant properties. They act by denaturing microbial proteins, binding to cell walls, and inhibiting enzymes essential for microbial survival. Tannins, in particular, form complexes with microbial proteins, impairing microbial adhesion and colonization, which is valuable for limiting the growth of actinomycetes and fungi in mycetoma lesions. The antioxidant properties of phenolics also protect host tissues from oxidative damage, reducing inflammation and aiding healing(Goyal et al., 2016; Shukla et al., 1999; Kumar et al., 2011)
7.5 Synergistic Effects of Multi-Component Plant Extracts
One key advantage of plant-based therapy is that whole extracts contain multiple bioactive compounds that can act synergistically. For example, an extract from neem or turmeric may simultaneously contain alkaloids, flavonoids, terpenoids, and phenolics, each targeting different aspects of the pathogen or host response. This multi-targeted approach enhances antimicrobial efficacy, reduces the likelihood of resistance, and also addresses inflammation and tissue repair. Unlike single-molecule drugs, which often target one specific pathway, multi-component plant extracts provide a holistic and more adaptable therapeutic effect, especially important in chronic, complex infections like mycetoma. (Ahmad et al., 2013; Cowan, 1999; Wagner & Ulrich-Merzenich, 2009)
7.6 Advantages Over Single-Molecule Synthetic Drugs
Phytochemicals offer several advantages compared to conventional single-molecule drugs. First, their multi-targeted actions can simultaneously inhibit pathogens, reduce inflammation, and promote healing. Second, they often have fewer side effects because they are naturally metabolized and are generally well-tolerated when used in traditional dosages. Third, plant-based therapies are often affordable and accessible, particularly in rural endemic areas where synthetic drugs may be expensive or unavailable. Finally, the synergistic nature of multiple phytochemicals in a single plant extract reduces the likelihood of microbial resistance, which is a major concern with long-term use of conventional antibiotics and antifungals in mycetoma. (Fabricant & Farnsworth, 2001; Goyal et al., 2016; Raut & Karuppayil, 2014)
8. FORMULATION APPROACHES USING MEDICINAL PLANTS
8.1 Herbal Ointments, Gels, and Pastes for Topical Application
Topical formulations are the most direct and practical approach for delivering medicinal plants in the management of mycetoma, especially for cutaneous lesions and sinus tracts. Herbal ointments, gels, and pastes are prepared from plant extracts such as Curcuma longa (turmeric), Lawsonia inermis (henna), and Azadirachta indica (neem) (Patel et al., 2020). These formulations allow localized delivery of bioactive compounds directly to infected tissue, enhancing antimicrobial activity while minimizing systemic side effects (Kumar & Singh, 2019). For instance, turmeric paste applied to lesions not only inhibits fungal growth but also reduces inflammation and promotes tissue regeneration (Aggarwal et al., 2007). Similarly, neem ointments combine antimicrobial and anti-inflammatory effects to aid healing (Biswas et al., 2002). The viscosity of gels and pastes ensures prolonged contact with the lesion, improving drug retention and therapeutic efficacy (Chaudhary et al., 2018). Topical formulations are particularly advantageous in resource-limited endemic areas, where systemic antifungal therapy may be expensive, unavailable, or associated with toxicity (van de Sande, 2013).
8.2 Nanoformulations and Phytosomal Delivery Systems
Recent advances in pharmaceutical technology have enabled the development of nanoformulations and phytosomal delivery systems for medicinal plants (Patra et al., 2018). Nanoformulations involve encapsulating plant extracts or bioactive compounds into nanoparticles, liposomes, or solid lipid carriers, which improve stability, bioavailability, and targeted delivery (Singh et al., 2017). Phytosomes are complexes of phytochemicals with phospholipids, enhancing lipid solubility and membrane permeability (Maiti et al., 2006). For example, curcumin-loaded nanoparticles or phytosomes exhibit enhanced penetration into dense fungal grains and deeper tissue layers, overcoming one of the major challenges in mycetoma treatment (Yallapu et al., 2012). These advanced delivery systems also allow controlled release of bioactive compounds, maintaining effective concentrations over prolonged periods and reducing the frequency of application (Bilia et al., 2014). Nanoformulations and phytosomes thus provide a modernized, efficient, and potentially more effective method of utilizing medicinal plants in chronic mycetoma therapy (Patra et al., 2018).
8.3 Controlled Release and Enhanced Penetration Strategies
Controlled release strategies aim to maintain therapeutic levels of bioactive compounds over extended periods, reducing dosing frequency and improving patient adherence (Dash et al., 2010). Techniques such as hydrogel-based systems, polymeric carriers, and nanoencapsulation are employed to achieve sustained release (Hoffman, 2002). Enhanced penetration strategies, including ultrafine nanoparticles, liposomes, and permeation enhancers, help deliver plant-derived compounds through the skin and into deeper tissues where fungal or bacterial grains reside (Pinto et al., 2013). This is particularly important in mycetoma, where the dense structure of grains and fibrotic tissue limits drug access (van de Sande, 2013). By combining controlled release with enhanced penetration, these formulations maximize the antimicrobial, anti-inflammatory, and wound-healing potential of medicinal plants, making them highly suitable for topical and adjunctive therapy in endemic regions (Patra et al., 2018)..
9. SAFETY, TOXICITY, AND STANDARDIZATION ISSUES
9.1 Need for Toxicity Profiling and Dose Optimization
Although medicinal plants are often perceived as “natural and safe,” their bioactive compounds can have toxic effects at high doses or with prolonged use. For example, compounds like azadirachtin from neem or allicin from garlic can cause gastrointestinal irritation, hepatotoxicity, or allergic reactions if improperly dosed (Biswas et al., 2002; Benkeblia, 2004). Therefore, rigorous toxicity profiling is essential before clinical application. This includes acute, sub-acute, and chronic toxicity studies, along with evaluation of organ-specific effects, mutagenicity, and teratogenicity (Patel et al., 2020). Dose optimization studies are also critical to determine the minimum effective dose that achieves antimicrobial and wound-healing effects without causing adverse reactions (Kumar et al., 2019). In the context of mycetoma, where treatment may extend over months or years, establishing safe dosing regimens is crucial to prevent cumulative toxicity and ensure long-term safety for patients (van de Sande, 2013).
9.2 Variability in Plant Composition and Quality Control
The chemical composition of medicinal plants can vary widely depending on species, geographical origin, cultivation conditions, harvest time, and extraction method (Mandal et al., 2007). For instance, curcumin content in turmeric or thymoquinone in Nigella sativa can fluctuate significantly, affecting therapeutic efficacy and reproducibility (Aggarwal et al., 2007; Ahmad et al., 2013). Such variability poses a major challenge in both research and clinical applications. Quality control measures, such as phytochemical profiling, marker compound quantification, and chromatographic fingerprinting, are essential to ensure consistency and potency of plant-based formulations (Sasidharan et al., 2011). Without strict quality control, the same plant preparation could have sub-therapeutic activity in one batch and toxic effects in another, compromising both safety and treatment outcomes (Patra et al., 2018).
9.3 Challenges in Standardization and Regulatory Approval
Standardization of medicinal plant products is critical for widespread clinical use, but it faces several challenges (Ekor, 2014). Unlike synthetic drugs, which have a single active molecule, plant extracts are multi-component mixtures whose efficacy arises from synergistic interactions (Mukherjee et al., 2007). Standardizing such complex mixtures requires identifying key bioactive compounds or marker molecules and establishing reproducible extraction, formulation, and storage protocols (Williamson et al., 2013). Regulatory approval is further complicated because agencies like the FDA or EMA require evidence of safety, efficacy, and quality control, which is often lacking for traditional herbal remedies (Patwardhan et al., 2005). Additionally, variations in traditional preparation methods and local practices make it difficult to create globally applicable standards. Overcoming these hurdles requires a combination of scientific research, clinical trials, and harmonized regulatory guidelines to ensure that medicinal plants can be used safely, effectively, and reliably for mycetoma treatment (van de Sande, 2013).
10. FUTURE PERSPECTIVES
10.1 Integration of Medicinal Plants with Modern Diagnostics
One of the key future directions in mycetoma management is the integration of medicinal plants with modern diagnostic tools (van de Sande, 2013). Currently, diagnosis relies on invasive methods, microscopy, and culture techniques, which are often slow, costly, or inaccessible in endemic areas (Ahmed et al., 2017). Plant-derived compounds, such as natural dyes, bioactive metabolites, or phytochemical markers, could be incorporated into rapid, low-cost diagnostic assays (Patel et al., 2020). For example, certain plant-based stains may enhance visualization of fungal or bacterial grains in tissue samples, while specific phytochemicals could serve as biomarkers for pathogen detection in biosensor platforms (Tripathi et al., 2019). By combining traditional ethnobotanical knowledge with modern diagnostic technologies, it is possible to develop point-of-care diagnostic tools that are both affordable and effective, improving early detection and reducing disease complications (Ekor, 2014).
Another promising future perspective is the development of plant-based combination therapies (Mukherjee et al., 2007). Chronic mycetoma often requires long-term treatment with antifungals or antibiotics, which can be expensive, toxic, and associated with poor compliance (van de Sande, 2013). Plant extracts, containing multiple synergistic phytochemicals, could be used in combination with conventional drugs to enhance antimicrobial efficacy, reduce treatment duration, and minimize side effects (Aggarwal et al., 2007; Patra et al., 2018). For example, combining curcumin or neem extracts with low-dose antifungals could improve drug penetration into mycetoma grains and reduce fungal load more effectively than single-drug therapy (Yallapu et al., 2012). Such combination approaches may also mitigate drug resistance, a major challenge in long-term therapy (Dash et al., 2010). Research on these combination therapies can pave the way for more holistic, multi-targeted, and patient-friendly treatment regimens (Singh et al., 2017).
10.3 Clinical Validation and Translational Research Needs
While many medicinal plants show promising in vitro and in vivo activity against mycetoma, there is a critical need for clinical validation and translational research (Patel et al., 2020). Laboratory studies provide preliminary evidence, but controlled clinical trials are essential to establish safety, efficacy, dosing regimens, and potential interactions with conventional drugs (Mukherjee et al., 2007). Translational research should focus on optimizing formulations, standardizing extracts, and assessing long-term outcomes in real-world patient populations (Patra et al., 2018). This will not only strengthen the scientific credibility of plant-based therapies but also facilitate regulatory approval and integration into formal healthcare systems (Ekor, 2014). Collaboration between ethnobotanists, pharmacologists, clinicians, and public health experts is essential to move from traditional knowledge to evidence-based practice (Williamson et al., 2013).
10.4 Role of Ethnopharmacology in Drug Discovery for Neglected Diseases
Ethnopharmacology—the study of traditional medicinal knowledge—plays a crucial role in discovering novel therapeutic agents for neglected tropical diseases like mycetoma (Patwardhan et al., 2005). Many plants used in endemic regions have historically documented antimicrobial, anti-inflammatory, and wound-healing effects, providing a rich source of bioactive compounds (Biswas et al., 2002; Aggarwal et al., 2007). By systematically documenting, screening, and scientifically validating these plants, researchers can identify new phytochemicals, elucidate mechanisms of action, and develop plant-derived drugs tailored to neglected diseases (Mukherjee et al., 2007). This approach not only preserves cultural and traditional knowledge but also addresses the urgent need for affordable, effective, and accessible therapies in resource-limited settings (Ekor, 2014). Ethnopharmacology thus offers a sustainable and innovative path for drug discovery, particularly for diseases that attract limited commercial pharmaceutical investment (Patel et al., 2020).
11. CONCLUSION
Medicinal plants represent a promising and cost-effective alternative for the management of mycetoma, a chronic and neglected tropical disease that disproportionately affects populations in resource-limited endemic regions (van de Sande, 2013; Ahmed et al., 2017). Their multifaceted properties—including antimicrobial, antifungal, anti-inflammatory, immunomodulatory, and wound-healing effects—make them particularly valuable for addressing the complex pathophysiology of mycetoma, including persistent infection, chronic inflammation, tissue destruction, and delayed healing (Aggarwal et al., 2007; Biswas et al., 2002; Patel et al., 2020).
Beyond treatment, certain plant-derived compounds also hold potential for enhancing early diagnosis, for instance, as natural dyes, bioactive biomarkers, or components of low-cost diagnostic assays, which could facilitate timely intervention and reduce the morbidity associated with late-stage disease (Tripathi et al., 2019; Patel et al., 2020).
Despite their promise, the full potential of medicinal plants in mycetoma management remains largely underexplored, primarily due to variability in plant composition, lack of standardized formulations, limited clinical validation, and regulatory hurdles (Mukherjee et al., 2007; Ekor, 2014; Patra et al., 2018). Therefore, systematic research, translational studies, and controlled clinical trials are urgently needed to evaluate efficacy, establish safe dosing regimens, optimize delivery systems, and develop evidence-based guidelines (Dash et al., 2010; van de Sande, 2013).
In conclusion, integrating medicinal plants with modern diagnostics, therapeutic strategies, and clinical validation has the potential to transform mycetoma management, offering affordable, accessible, and culturally acceptable interventions while advancing drug discovery for neglected tropical diseases (Patwardhan et al., 2005; Williamson et al., 2013).
REFERENCES


Devendra Bansal, Rachana Akhand Giri, Roles of Medicinal Plants in the Diagnosis and Treatment of Mycetoma, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3657-3675. https://doi.org/10.5281/zenodo.18442860
 10.5281/zenodo.18442860
10.5281/zenodo.18442860