
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sardar Patel College of Pharmacy, Bakrol, 388315, Gujarat, India
In pharmaceutical new technology, transdermal drug delivery systems (TDDS) have made a fascinating research topic and are one of the most commonly manufactured pharmaceutical products in the global market. These systems can overcome the associated disadvantages of other delivery routes, such as oral and parenteral. A transdermal drug delivery system (TDDS) is a promising delivery system that gives prolonged drug release at a predetermined time. It has many positive consequences, such as passing the first-pass effect, enhancing patient convenience by providing a single application rather than multiple dosing frequencies, and appendageal, intracellular and intercellular. Permeation of drug substances through the stratum corneum remains a significant challenge because it is the rate limiting step for permeation for most molecules. This review article highlights the advances and limitations of the strategies to improve the transdermal delivery of drugs in to the skin, including physical and chemical methods, specifically focusing on providing a comprehensive understanding of transdermal drug delivery systems and enhancement strategies. various penetration enhancing strategies have been successfully employed to enhance the permeation of common and high molecular weight drugs.
Most small molecule medications are typically administered orally since oral and parenteral administration are the two most popular drug delivery methods. The primary goal of a transdermal medication delivery system is to deliver pharmaceuticals in to systemic circulation through the skin at a predefined rate with minimum inter and intra patient variation. (1) pre-set dosages, mobility and patient self-administration are benefits of the oral route. For these reasons, administering drugs orally is still the most practical method. However, due to fast stomach breakdown and size restricted transport through the epithelium, most therapeutic peptides or proteins are not administered orally. Therefore, injections are the most common technique of administering macromolecules. (2) However, injections have some drawbacks, including the invasive nature of injections that cause pain and lower patient acceptance/compliance, in addition to the need for administration by a trained administrator. (3)
1.1. Advantages (4)
1.2. Disadvantages (5)
1.3. Limitations (6)
1.4. Properties that influence transdermal drug delivery (7)(8)
Effective transdermal drug delivery can be formulated by considering three factors drug, skin, and vehicles.so the factors affecting this can be divided in to biological and physiochemical factors.
A. Biological factors
B. Physiochemical factors
1.5. Ideal molecular properties for transdermal drug delivery (8)
From the above considerations, we can conclude with some observations that can be termed ideal molecular properties for drug penetration.
They are as follows,
2. SKIN STRUCTURE AND ANATOMY (9)(10)
2.1. Skin
The skin is the largest organ of the human body.it acts as a protective barrier against external influences such as ultraviolet radiation, chemical and physical insults, attacks by harmful microorganisms and mechanical irritation. Furthermore, the skin regulates the body’s physiological parameters by providing a barrier against water evaporation and temperature loss. Skin diseases such as infections triggered by bacteria or viruses and the immunologically caused chronic skin diseases psoriasis, atopic dermatitis, urticaria or ichthyosis damage the skin barrier.
Physiological functions can no longer be maintained, increasing risk of further infection. Symptoms such as pain, soreness and wetness affect the patient’s quality of life.
2.2. Skin Anatomy (11)
Human skin consists of two layers, the epidermis and the dermis. the epidermis can be divided in to four layers, with the stratum corneum on top, followed by the stratum granulosum, stratum spinosum, and stratum basale. The stratum corneum plays the most decisive part in skin penetration. It consists of dead corneocytes embedded in a crystalline lamellar lipid matrix. In contrast to the living keratinocytes, the already dead corneocytes here have a solid protein envelope that prevents the absorption of substances. This envelope has a hook like structure that enables the corneocytes to interlock. Between the surfaces of the corneocytes are the corneodesmosomes, proteins that connect the individual corneocytes. The structure of corneocytes, connected via corneodesmosomes, is already formed in deeper layers of the epidermis and is supplemented by different proteins at the transition to the stratum corneum to strengthen the mechanical stability of this skin layer.
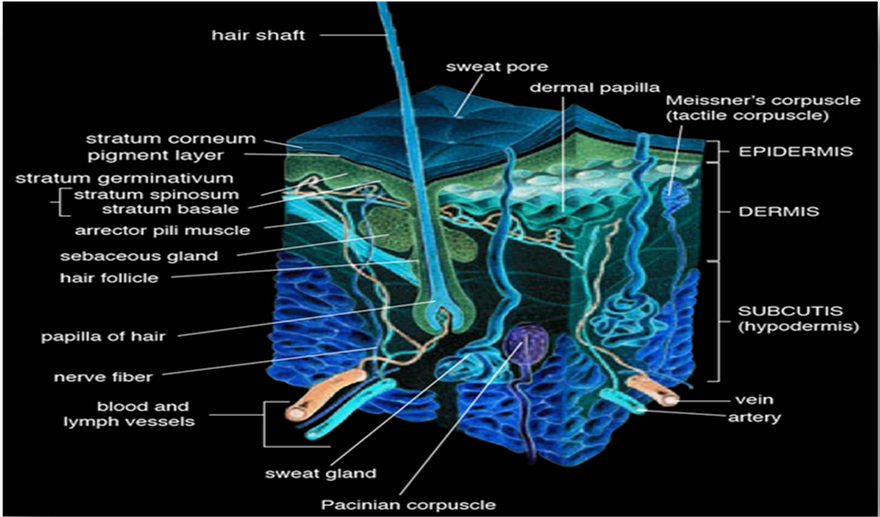
Figure no.1. Regional variation in water permeability of stratum corneum
Between the stratum corneum and the stratum granulosum, tight junctions separate the stratum corneum from the lower layers of the epidermis. The stratum granulosum and stratum spinosum mainly protect the lower skin layers from water loss and are the site of differentiation of the corneocytes. The lowest layer of the epidermis is the stratum basale. The keratinocytes are produced from the stem cells contained there. The transit time from their formulation in the stratum basale to the stratum corneum is 14 days. The complete renewal cycle takes 28 days. The dermis beneath the epidermis ensures the flexibility of the skin and temperature maintenance of the body. It consists mainly of collagen fibers interspersed with elastic fibers, surrounded by a matrix of through the dermis. The dermis and subcutis underneath are irrelevant for penetrating dermal therapy substances. In systemic therapy with transdermal system, however, drugs must be able to penetrate the blood vessels in the dermis and subcutis.
2.3. Biochemistry of the stratum corneum(11)
The surrounding lipid matrix consists equally of ceramides with a chain length of 16 to 33 carbons, cholesterol derivatives and free fatty acids, predominantly with chain length of 22 or 24 carbon atoms. The lipids are arranged in a lamellar structure in which the lipophilic head groups of the ceramides, cholesterol and free fatty acids are directed toward one another. The non-covelant interactions of the head groups thus create lipophilic and hydrophilic area in stratum corneum from which the lipid bilayer results. Investigations of the composition of the individual components showed the cholesterol derivatives and ceramides have a hexagonal structure in a 1:1 ratio.
The addition of free fatty acids results in a shift to orthorhombic packing. The packing density is increased, which leads to the deduction that a balanced composition of the ingredients is essential for an intact skin barrier. Substances can be transported intercellularly, transcellularly or a corneodesmosomal pathway through the stratum corneum. The penetration mechanism will be addressed in a subsequent part of this review.
3. DRUG PERMEATION THROUGH THE SKIN (12)(13)
3.1. Fundamentals of skin permeation
Until the last century, the skin was supposed to be impermeable, except for gases. However, in the current century, the study indicated the permeability of lipid-soluble drugs. Also, it was recognized that various layers of skin are not equally permeable. i.e., the epidermis is less permeable than the dermis. After an enormous controversy, all doubts about stratum corneum permeability were removed and using isotopic tracers; it was suggested that stratum corneum significantly hamper permeation.
The average human skin contains 40-70 hair follicles and 200-250 sweat per square centimeter. Especially water-soluble substances pass faster through these ducts. Still, these ducts do not contribute much to skin permeation. Therefore, most neutral molecules pass through the stratum corneum by passive diffusion. Regional variation in water permeability of stratum corneum showed in table 1.
Table 1. Regional variation in water permeability of stratum corneum
|
Sr no. |
Skin region |
Thickness (µm) |
Permeation time (mg/cm2/hr) |
Diffusivity (cm2/secx1010) |
|
1 |
Abdomen |
15.0 |
0.34 |
6.0 |
|
2 |
Volar forearm |
16.0 |
0.31 |
5.9 |
|
3 |
Back |
10.5 |
0.29 |
3.5 |
|
4 |
Forehead |
13.0 |
0.85 |
12.9 |
|
5 |
Scrotum |
5.0 |
1.70 |
7.4 |
|
6 |
Back of hand |
49.0 |
0.56 |
32.3 |
|
7 |
Palm |
400.0 |
1.14 |
535.0 |
|
8 |
Plantar |
600.0 |
3.90 |
930.0 |
Series of steps in sequence:
Previously, the skin was considered an impermeable protective barrier, but later investigations are carried out, proving skins utility as a route for systemic administration.
The various steps involved in the transport of drugs from patch to systemic circulation are as follows.
The permeation of drug molecules through the skin is shown in figure no.2
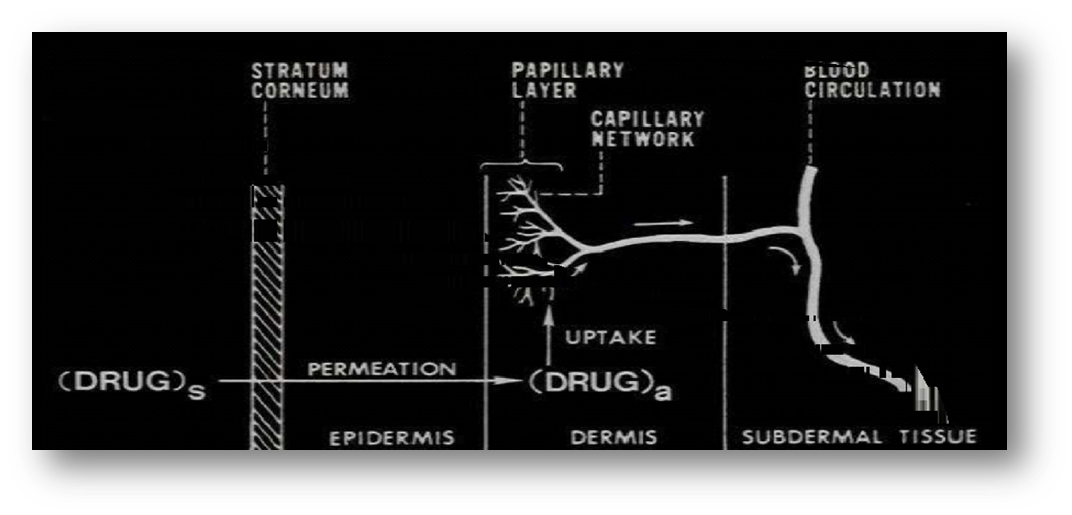
Figure no.2. Multilayer skin model showing the sequence of Transdermal permeation of drug for systemic delivery
Intracellular regions in the stratum corneum are filled with lipid rich amorphous material. In dry stratum corneum, the intracellular volume may be 5% to 1% in fully hydrated stratum corneum.
The microstructure of stratum corneum is shown in figure no.3.
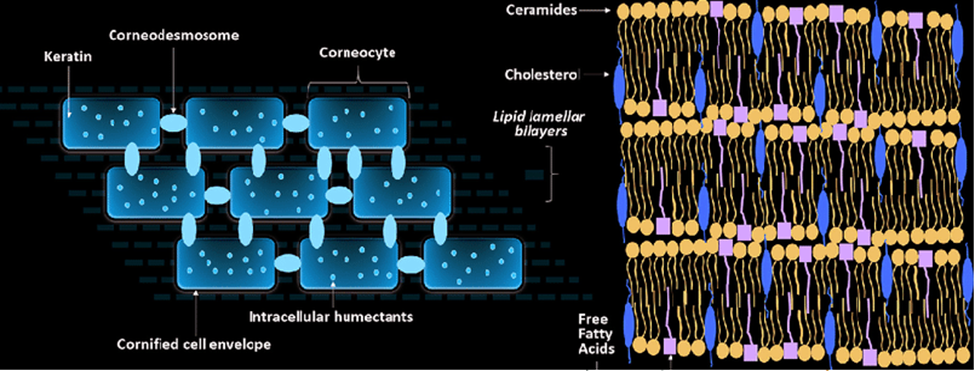
Figure no.3. The microstructure of stratum corneum
Percutaneous absorption involves the passive diffusion of substances through the skin. A molecule may use two diffusional routes to penetrate normal intact skin: appendageal and epidermal.
1. Appendageal route: Appendageal route comprises transport via sweat glands and hair follicles with their associated sebaceous glands. Therefore, these routes circumvent penetration through the stratum corneum and are known as shunt routes. This route is of minor importance because of its relatively small area, approximately 0.1% of the total skin area.
2. Epidermal route: For drugs, which mainly cross intact the horney layer, two potential micro routes of entry exist, the transcellular (intracellular)and intercellular pathways.
Transcellular: Transcellular pathways means the transport of molecules across the epithelial cellular membrane. These include passive transport of small molecules, active transport of ionic and polar compounds and endocytosis and transcytosis of macromolecules.
Paracellular: Paracellular pathway means the transport of molecules around or between the cells. Tight junctions or similar situations exist between the cells. A permeants principal pathway is decided mainly by the partition coefficient (log k). Hydrophilic drugs partition preferentially in to the intracellular route. Most permeants permeate the stratum corneum by both routes. However, the tortuous intercellular pathway is widely considered to provide the principal route and significant barrier to the permeation of most drugs.
4. STRATEGIES TO ENHANCE TRANSDERMAL DELIVERY (14)(15)
Although transdermal delivery of the drugs is an excellent alternative to other routes of drug delivery, permeation via the stratum corneum remains a big challenge. Stratum corneum is a formidable skin barrier, and efforts have been made to overcome it. There are many ways to improve the transdermal permeation of drugs; they can be classified into active or physical and passive or chemical strategies.
4.1. Physical Methods
They involve the application of external stimuli for the active enhancement of transdermal permeation
4.1.1. Sonophoresis
It refers to the application of ultrasound to enhance transdermal drug delivery. The exact mechanism of how ultrasound increases transdermal permeability needs to be better understood. However, acoustic cavitation, which structurally modifies stratum corneum lipids to create diffusional channels, could be the mechanism of ultra-sound-induced permeation. Increased skin permeation by thermal effects has also been hypothesized, increasing the skin permeability and drug diffusion coefficients. (16) An enhancement of skin permeation by ultrasound widens the advantages and application of transdermal delivery. It can be classified into low, intermediate, and high-frequency sonophoresis according to the applied frequency. Sonophoresis can be used as pretreat for the skin before drug application to increase its effect or as a formulation that can be applied simultaneously. Although that there are many compounds are marketed as ultrasound-enhanced transdermal delivery, such as Lidocaine which was approved in 2004, there are still some challenges regarding this technology which include the development of inexpensive ultrasound devices that can assure efficient transdermal delivery as well as the safety of this technology remains an issue since high-frequency ultrasound may induce second-degree burns. (17)
4.1.2.Microneedles (MNs)
Recently, MNs have been introduced as an effective way to enhance drug penetration into the skin. They are painless, micronized projections arranged in arrays; when applied to the skin, it can increase percutaneous permeation dramatically. The first report on this system was in late 1990. Since stratum corneum thickness is only 10-20μm, MNs with a few hundred microns can deliver the drug and bypass this barrier successfully. MNs are painless since they avoid the sensory nerve fibers. Structurally, MNs can be classified into four types: solid MNs, dissolving MNs, coated MNs, and hollow MNs. Solid MNs can be used as skin pre-treatment to enhance percutaneous drug permeation.
In this type, the MNs penetrated the skin, and then the drug is delivered by the channels that are generated. Hence this type uses the 'poke and patch' approach of delivery. Various materials such as silicon, polymers including both biodegradable and non-degradable polymers such as polylactic-glycolic acid (PLGA), maltose, and metals including stainless steel and nickel have been used to form solid MNs. Dissolving MNs are driving attention due to their advantages over the other types, including high drug loading, convenience, and easy fabrication method. This type uses the 'poke and release' approach of delivery, which relies on the penetration of the skin by the microneedle patch and then drug release from the loaded dissolving tips. Polymers such as polyvinyl alcohol were utilized and dissolved four minutes after inserting into the skin. Hollow MNs use the 'poke and flow' approach of delivery via micronized holes within the needles. Materials such as glass, silicone, and stainless steel can be used to fabricate this type of MNs. The flow rate via the holes has to be controlled since a high flow rate may cause pain. Besides drug delivery, hollow MNs can be exploited in blood extraction analysis using the poke and flow approaches. Coated MNs utilize the 'coat and poke' delivery approach, which includes the insertion of the microneedle patch first into the skin, followed by releasing the drug coated on the microneedle tips. Coated MNs are solid MNs with superior advantages and patient compliance; they are considered single-step administration systems compared to solid MNs, which are complex two-step administration systems. Stainless steel and titanium have been employed as materials to fabricate this system. (18)
4.1.3.Iontophoresis
It was developed to facilitate the delivery of ionized solute across tissue membranes with inherently low partition coefficients due to their charged states. The principle of the iontophoresis technique is based on the fact that the like charges repels each other and opposite charge attract. Thus, during iontophoresis, if delivery of the positively charged drug, the charged drug is dissolved in the electromotive force, the drug is repelled and moves across the stratum corneum towards the cathode, placed elsewhere on the body. The drug permeation is caused by any one or a combination of the following mechanisms.
4.1.4. Magnetophoresis
This method involves the application of a magnetic field which acts as an external driving force to enhance the diffusion of a diamagnetic solute across the skin. Skin exposure to a magnetic field also induces structural alterations that increase permeability. This technique can be used for the permeation of diamagnetic molecules. This method has been implemented for the transdermal delivery of benzoic acid. The diffusion flux is directly proportional to the intensity of the applied magnetic field. This method involves the application of a magnetic field which acts as an external driving force to enhance the diffusion of a diamagnetic solute across the skin. (19)
4.1.5.Electroporation
Electroporation is the phenomenon in which cell membrane permeability to ions and macromolecules is increased by exposing the cell to short high electric field pulses. The mechanism for electroporation is by two pathways through pores formed in the multiple lipid bilayers connecting corneocytes and through appendage cells. (20) The efficacy of the transport of drugs depends on the electrical parameters and the physiochemical properties of drugs. In electroporation, the transdermal delivery of the drug molecule is increased by the application of a high voltage (100 volts) in the form of direct current (DC). (21)
4.1.6. Thermal ablation
It is a technique that involves the application of heat to increase drug permeation via the skin, causing depletion of the SC without damaging the deeper underlying tissues with an exposure period ranging from 1 microsecond to 100 milliseconds. The underlying mechanism involves stratum corneum vaporization and removal without damaging the deeper tissues. This can be done in two ways: 1) moderate temperature (less than 100?) for an extended period or 2) high temperature (more than 100?) for a short period, with the latter being more favorable to avoid skin damage. Different ways can be used to perform thermal ablation, including chemical heating, radiofrequency, and laser. Thermal ablation has been widely used to deliver macromolecules and vaccines, but care should be taken since excessive heat may damage the deeper layers and cause thermohaemolysis.(20)
4.1.7. Velocity-based devices
They include the application of velocity within the range of 100-200 m/s to punctuate the skin, using compressed gas or a coiled spring as a power source. This technique was used mainly to deliver vaccines and macromolecules, including monoclonal antibodies and hormones besides nucleic acids providing a needle-free approach based on jet injection for drug delivery. Although this technology offers an excellent alternative to conventional needles, some limitations were reported during their usage, including pain and bruising at the administration site.
4.2. Chemical Methods (21)
Chemical or passive methods to enhance transdermal permeation include chemical penetration enhancers, eutectic systems, and prodrugs.
4.2.1. Chemical enhancers
Chemical enhancers are one of the most commonly used methods to enhance skin penetration. Drug partitioning into the skin can be increased by several mechanisms, either by extraction of intercellular lipids or proteins of the stratum corneum or by hydration of the stratum corneum, which temporarily and reversibly changes the barrier nature of the skin and increases drug penetration. Ideally, the chemical enhancer should be non-toxic and non-irritant, compatible with other ingredients, biodegradable, cheap, and available, and change the morphological nature of the skin reversibly. There are many classes of penetration enhancers depending on their chemical structure, including fatty alcohols like (propylene glycol and ethanol), fatty acids like (oleic acid), sulfoxides like (dimethyl sulfoxide DMSO and dimethylformamide DMF), terpenes like camphor, surfactants (cationic, anionic, zwitterion, non-ionic-ionic) and urea. The safety of penetration enhancers should be a concern since they can cause skin irritation, including swelling, local inflammation, erythema, and dermatitis.
4.2.2. Prodrug
It is a compound that is inactive in its parent form, and after entering the body, it will convert back to its active form. This approach has been investigated for transdermal delivery; the resultant prodrug has different physicochemical properties, including lipophilicity, partition coefficient, and solubility, resulting in better skin penetration. Prodrug is formed upon modification of the drug's chemical structure, most commonly through covalent linkage of the active drug with inactive moiety by an ester bond. Upon contact with skin, non-specific esterases of the skin will cleave the bond, liberating the active drug to exert its action. Many drugs showed improved permeation using this approach, for example, diclofenac acid prodrug formation to enhance transdermal delivery.
4.2.3.Eutectic systems
Eutectic systems are formulations that combine two compounds in an adequate ratio and the resultant mixture substance has a melting point lower than this of each compound alone. This lowering of melting point leads to an increment in insolubility in the stratum corneum lipids and hence better skin penetration.
4.2.4. Other methods (22)(23)(24)
4.2.4.1. Asymmetric TPX membrane method:
A prototype patch can be fabricated for this. A heat-sealable polyester film (type 1009, 3m) with a concave 1cm diameter will be used as the backing membrane. The drug sample is dispensed into the concave membrane, covered by a TPX {poly(4-methyl-1-pentene)} asymmetric membrane, and sealed by an adhesive. [(Asymmetric TPX membrane preparation): These are fabricated using the dry/wet inversion. TPX is dissolved in a mixture of solvent (cyclohexane) and nonsolvent additives at 60°c to form a polymer solution. The polymer solution is kept at 40°C for 24 hrs and cast on a glass plate to a predetermined thickness with a Gardner knife. After that, the casting film is evaporated at 50°C for 30 sec; then, the glass plate is immersed immediately in a coagulation bath [maintained at 25°C]. After 10 minutes of immersion, the membrane can be removed; air dry in a circulation oven at 50°C for 12 hrs].
4.2.4.2. Circular Teflon mold method:
Solutions containing polymers in various ratios are used in an organic solvent. The calculated amount of the drug is dissolved in half the quantity of the same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. Di-N-butyl phthalate is added as a plasticizer into a drug-polymer solution. The contents will be stirred for 12 hrs and poured into a circular Teflon mold. The molds will be placed on a leveled surface and covered with an inverted funnel to control solvent vaporization in a laminar flow hood model with an air speed of 0.5 m/s. The solvent is allowed to evaporate for 24 hrs. Before evaluation, the dried films will be stored for another 24 hrs at 25±0.5°C in a desiccator containing silica gel to eliminate aging effects. The type of films will be evaluated within one week of their preparation.
4.2.4.3. Mercury substrate method:
In this method, the drug is dissolved in a polymer solution along with a plasticizer. The above solution is stirred for 10- 15 minutes to produce a homogenous dispersion and poured into a leveled mercury surface, covered with an inverted funnel to control solvent evaporation.
4.2.3.4. By using the "IPM membranes" method:
The drug is dispersed in a mixture of water and propylene glycol containing carbomer 940 polymers and stirred for 12 hrs in a magnetic stirrer. The dispersion is to be neutralized and made viscous by adding triethanolamine. Buffer pH 7.4 can be used to obtain solution gel if the drug solubility in an aqueous solution is very poor. The formed gel will be incorporated into the IPM membrane.
4.2.4.5.By using the "EVAC membranes" method: I
In order to prepare the target transdermal therapeutic system, 1% Carbopol reservoir gel, polyethylene (PE), and ethylene vinyl acetate copolymer (EVAC) membranes can be used as rate control membranes. If the drug is not soluble in water, propylene glycol prepares the gel. The drug is dissolved in propylene glycol, and Carbopol resin will be added to the above solution and neutralized using a 5% w/w sodium hydroxide solution. The drug (in gel form) is placed on a sheet of backing layer covering the specified area. A rate-controlling membrane will be placed over the gel, and the edges will be sealed by heat to obtain a leakproof device.
4.2.4.6. Aluminium-backed adhesive film method:
Transdermal drug delivery systems may produce unstable matrices if the loading dose is more significant than 10 mg. Aluminium backed adhesive film method is a suitable one. For the preparation of the same, chloroform is the choice of solvent because most of the drugs and adhesives are soluble in chloroform. The drug is dissolved in chloroform, and adhesive material will be added to the drug solution and dissolved. A custom-made aluminum former is lined with aluminum foil, and the ends are blanked off with tightly fitting cork blocks.
4.2.4.7. By using the free film method:
A free cellulose acetate film is prepared by casting it on a mercury surface. A polymer solution of 2% w/w will be prepared using chloroform. Plasticizers are to be incorporated at 40% w/w of polymer weight. Five ml of the polymer solution was poured into a glass ring placed over the mercury surface in a glass petri dish. The solvent's evaporation rate is controlled by placing an inverted funnel over the petri dish. The film formation is noted by observing the mercury surface after complete evaporation of the solvent. The dry film will be separated and stored between the sheets of wax paper in a desiccator until use. Free films of different thickness can be prepared by changing the volume of the polymer solution.
4.3. Nanotechnology-based transdermal drug delivery systems by nanocarrier (19)(25)(26)(27)
4.3.1. Carriers and vehicles
4.3.1.1. Micro or nanocapsules
These comprise multiple concentric bilayers of surfactant separated by a polar liquid medium, generally water, in which the hydrophilic additives can be incorporated. Their lipid core allows encapsulation of lipid additives, and their multilamellar (lipid/water) structure creates good skin affinity leading to cutaneous penetration and good hydration.
4.3.1.2. Nanoemulsions/submicron emulsions/ mini emulsions
These are oil-in-water emulsions with an average droplet size ranging from 100 to 500 nm. They have excellent stability and do not undergo phase separation during storage. They have a liquid lipophilic core and are appropriate for lipophilic compound transportation. Many studies showed reduced transepidermal water loss, which means support to the skin's barrier function. Nanoemulsion viscosity is very low, which is interesting because they can be produced as sprays.
4.3.1.3. Solid lipid nanoparticles
Solid lipid nanoparticles (SLNs) have recently been investigated as carriers for enhanced skin delivery of sunscreens, vitamins A and E, triptolide, and glucocorticoids. It is thought that their enhanced skin penetrating ability is primarily due to increased skin hydration caused by the occlusive film formed on the skin surface by the SLN. A 31% increase in skin hydration has been reported following four weeks of application of SLN-enriched cream.
4.3.1.4. Multiple emulsions
These w/o/w emulsions consist of the dispersion of a w/o emulsion in an aqueous phase under several conditions. One can incorporate different water-soluble ingredients (even if they are incompatible) and oil-soluble additives. Like SLNs, these substances will be protected and released sustained by controlling droplet breakdown. These systems can have high oily phase contents (65%, Trixera, Bain emollient, Avène) and thus present good hydration. Their efficacy has been demonstrated in dermatology to treat stretch marks (Triffadiane, CS Dermatologie).
4.3.1.5. Microemulsions
These formulations are superior for cutaneous delivery compared with other conventional vehicles. These systems are identified as transparent water, oil, and surfactant mixtures. They are thermodynamically stable and optically isotropic. Microemulsions are spontaneously produced in a narrow range of oil-water-surfactant compositions, represented on pseudo-ternary diagram phases. They are dynamic systems with continuously fluctuating interfaces. Their good dermal and transdermal delivery properties could be attributed to their excellent solubilizing properties. Their high solubilizing properties improve indispensability and thus reduce the efficient dose, thereby increasing tolerability. Furthermore, their restructuring effect on skin and hair (because of their high lipid content) makes microemulsion formulations adapt to altered skin and hair conditions.
4.3.2. Vesicular carriers
4.3.2.1. Liposomes.
Liposomes are colloidal particles formed as concentric biomolecular layers capable of encapsulating drugs. Their potential for delivering drugs to the skin was first reported by Mezei and Gulasekharam in 1980, who showed that the skin delivery of triamcinolone acetonide was four to five times greater from a liposomal lotion than an ointment containing the same drug concentration. Phosphatidylcholine from soybean or egg yolk is the most common composition, although many other potential ingredients have been evaluated. Cholesterol added to the composition tends to stabilize the structure, thereby generating more rigid liposomes. Recent studies have focused on the delivery of macromolecules such as interferon, gene delivery, and cutaneous vaccination, in some cases combining the liposomal delivery system with other physical enhancement techniques such as electroporation.
4.3.2.2. Niosomes
Niosomes are vesicles composed of nonionic-ionic surfactants evaluated as carriers for several drug and cosmetic applications. This area continues to develop with further evaluation of current formulations and reports of other vesicle-forming materials.
4.3.2.3. Transfersomes
Transfersomes are vesicles composed of phospholipids as their main ingredient with 10 to 25% surfactant (such as sodium cholate) and 3 to 10% ethanol. The surfactant molecules act as 'edge activators,' conferring ultra deformability on the transfersomes, which reportedly allows them to squeeze through channels in the stratum corneum that are less than one-tenth the diameter of the transfersome. According to their inventors, where liposomes are too large to pass through pores of less than 50 nm in size, transfersomes up to 500 nm can squeeze through to penetrate the stratum corneum barrier spontaneously.
4.3.2.4. Ethosomes
These are liposomes with high alcohol content capable of enhancing penetration to deep tissues and systemic circulation. It is proposed that alcohol fluidizes the ethosomal lipids and stratum corneum bilayer lipids, thus allowing the soft, malleable ethosomes to penetrate
4.3.2.5. Aquasomes
A new class of solid drug carriers, aquasomes, emerged in the last decade. Aquasomes are three-layered structures (i.e., core, coating, and drug) self-assembled through non-covalent bonds, ionic bonds, and Van der Waals forces. They consist of a ceramic core whose surface is noncovalently modified with carbohydrates to obtain a sugar ball, which is then exposed to the adsorption of a therapeutic agent. The core provides structural stability to a largely immutable solid. Aquasomes offer an attractive mode of delivery for therapeutic agents belonging to the class of proteins and peptides because they can overcome some inherent problems associated with these molecules. These problems include suitable routes of delivery, physical as well as chemical instability, poor bioavailability, and potential side effects. The surface modification with carbohydrates creates a glassy molecular stabilization film that adsorbs therapeutic proteins with minimal structural denaturation. Thus, these particles provide complete protection of an aqueous nature to the adsorbed drugs against the denaturing effects of external pH and temperature because there are no swelling and porosity changes with changes in pH or temperature.
Successful transdermal drug delivery requires numerous considerations owing to the nature and function of the application site. It should always be remembered that the skin's primary functions are protection and containment. As per these rulings, it is challenging to cross the skin for systemic absorption. However, with continuous exploration of the skin's structure, function, and physicochemical properties, more and more new drug products are being developed for transdermal delivery. Safe and effective drug delivery is the ultimate target for every new technology explored. The search for the ideal skin penetration enhancer has been the focus of considerable research over several decades. Although many potent enhancers have been discovered, in most cases, their enhancement effects are associated with toxicity, therefore limiting their clinical application. In recent years, using several biophysical techniques has aided in understanding the nature of the stratum corneum barrier and how chemicals interact with and influence this structure. A better understanding of the interaction of enhancers with the stratum corneum and the development of structure-activity relationships for enhancers will aid in designing enhancers with optimal characteristics and minimal toxicity. (24)(25)
CONCLUSION
Skin permeation enhancement technology is a rapidly developing field that would significantly increase the number of drugs suitable for transdermal drug delivery, resulting in the skin becoming one of the major routes of drug administration in the next decade. Research in this area has proved the usefulness of physical and chemical penetration enhancers in enhancing drug permeation through the skin. The physical and chemical penetration enhancement methods discussed in this review are promising. The focus should be on skin irritation to select penetration enhancers with minimal skin irritation with optimum enhancement effects.
REFERENCES

Ankur Patel, Strategies to Improve Transdermal Permeation, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1534-1548. https://doi.org/10.5281/zenodo.18258031
 10.5281/zenodo.18258031
10.5281/zenodo.18258031