Hamsa Homoeopathy Medical College Hospital and Research Centre, Ksheerasagar, Mulugu, Siddipet, Telangana
Bone is a dynamic and highly specialized connective tissue that combines inorganic calcium salts, mainly calcium phosphate and carbonate, with organic collagen fibers. This unique composition allows bones to withstand both compressive and tensile forces, making them comparable in strength to materials like iron and steel. Despite their hardness and mineralization, bones are living tissues with high vascularity, actively undergoing remodeling and self-repair after injury, including fractures. Bone fractures, resulting from trauma or disease, pose significant challenges in pain management and tissue regeneration. Homeopathy offers a range of remedies aimed at accelerating fracture healing, reducing pain, and supporting callus formation without interfering with conventional fracture management. Key remedies frequently used include Arnica montana for early trauma and swelling, Symphytum officinale to stimulate callus formation and promote bone regeneration, Ruta graveolens for periosteal injuries, Calcarea phosphorica and Calcarea carbonica for delayed or weak healing, and Hypericum for nerve-rich injuries. Clinical observations and emerging studies suggest that individualized homeopathic protocols can result in faster radiological union, improved functional outcomes, and decreased analgesic requirements when combined with standard orthopedic care. While current research highlights promising results, further rigorous trials are needed to determine the precise efficacy and integration of homeopathic remedies in fracture management.
The structural and functional complexity of bone arises from its dual composition—rigid mineralized matrix for structural support, and flexible collagen for resilience. Bone continuously remodels in response to mechanical stress, exhibiting properties such as disuse atrophy and overuse hypertrophy. There are two principal types of bone formation (ossification): direct (membranous) ossification, which forms bones such as the clavicle and skull, and indirect (cartilaginous) or endochondral ossification, responsible for most skeletal bones like those of the limbs and trunk. Bone tissue is organized into compact and spongy types, with distribution varying by bone type and location—compact bone provides strength on the outer surfaces, while spongy bone occupies inner regions and supports hematopoiesis. Bone health and adaptability are essential to musculoskeletal integrity, enabling bones to heal after fractures and adjust to physiological demands throughout life.?
AIMS & OBJECTIVES
MATERIALS
A review of authoritative literature on bone physiology and fracture healing, including textbooks such as B.D. Chaurasia's Handbook of General Anatomy and The Essentials of Human Osteology with Colour Atlas.
Standardized descriptions and definitions of bone structure, ossification (direct/membranous and indirect/cartilaginous), and types of bone (compact, spongy, long, short, flat, irregular, pneumatic, sesamoid).
Clinical case data and observations from documented protocols where homeopathic remedies such as Arnica montana, Symphytum officinale, Ruta graveolens, Calcarea phosphorica, Calcarea carbonica, and Hypericum were administered in fracture management, alongside conventional orthopedic care.
METHODS
Comprehensive review and synthesis of anatomical, physiological, and pathological features of bone, focusing on composition, remodeling capacity, and fracture healing mechanisms.
Systematic examination of the evidence base regarding homeopathic treatment for bone fractures, including selection criteria for remedies tailored to injury phase and symptom profile.
Documentation of ossification mechanisms—differentiating between membranous and cartilaginous ossification—and their clinical significance in fracture healing.
Analysis of observed outcomes, including time to radiological union, pain relief, callus formation, and functional recovery in patients receiving both conventional and individualized homeopathic fracture care.
Reference to established clinical and research methodologies from reviewed literature to support validity and reproducibility.
REVIEW OF LITERATURE
Definition
1. Bone
(Synonyms : Os ; Osteon ) is one-third connective tissue. It is impregnated with calcium salts which constitute two-thirds part. The inorganic calcium salts (mainly calcium phosphate, partly calcium carbonate, and traces of other salts) make it hard and rigid, which can afford resistance to compressive forces of weight-bearing and impact forces of jumping. The organic connective tissue (collagen fibres) makes it tough and resilient (flexible), which can afford resistance to tensile forces. In strength, bone is comparable to iron and steel . Despite its hardness and high calcium content the bone is very much a living tissue. It is highly vascular, with a constant turn-over of its calcium content. It shows a characteristic pattern of growth. It is subjected to disease and heals after a fracture. It has greater regenerative power than any other tissue of the body, except blood. It can mould itself according to changes in stress and strain it bears. It shows disuse atrophy and overuse hypertrophy.¹
2. Formation of Bone
The process of gradual bone formation is known as Ossification. Mesenchymal cells which differentiate into osteogenic cells form a structural basis which gives rise to bone directly or through an intermediary stage of cartilage. Thus ossification is classified as-
Ossification in membrane is an urgent affair and the process is completed with extreme rapidity whereas ossification in cartilage is a gradual and leisurely procedure. The process of ossification is essentially similar in both types and the final histological structure of membrane and cartilage bones is identical . In ossification, the first thing to take place in the embryonic stage is the condensation of mesenchyme at the predetermined site of formation of future bone. Such condensations of mesenchyme have an inherent property for self-differentiation into either cartilage or bone.
Membranous Ossification : If bone is formed directly into the mesenchymal rudiment, it is called Membranous or Intramembranous or Direct ossification and the bone developed is called a membrane bone.
Examples: Clavicle, bones of face and vault of skull.
Sequence of events in Membranous Ossification:
This is a process in which ossification starts directly in a membrane where the osteoblasts simply lay down bone.
2. Cartilaginous Ossification
If the mesenchymal rudiment is first converted into a cartilaginous model (hyaline cartilage) of the same shape as future bone which is subsequently destroyed and replaced by (but is never changed into) bone it is called Cartilaginous or Intracartilaginous or Endochondral or Indirect ossification and the bone developed is called a ‘Cartilage bone’. Most bones of the body are preformed in cartilage.
Examples: Bones of limbs (except clavicle), trunk and base of skull.
Sequence of events in Cartilaginous Ossification:
Important points in Cartilaginous Ossification:
Secondary Cartilage bone: In certain bones such as mandible and clavicle, which are primarily ossified in membrane, and there is no preformed cartilaginous model, cartilage subsequently appears, e.g., at the neck of mandible and sternal end of clavicle, proliferates and undergoes ossification. This is known as ‘secondary cartilage bone and its histological structure differ from cartilage bone. Its cells are larger and more closely packed and the matrix is much more fibrous²
On gross examination of a section of any bone, it is seen to be composed of two kinds of tissue:
Compact bone All bone has a dense outer layer consisting of compact bone that appears smooth and solid.
Spongy, cancellous or trabecular bone Internal to compact bone is spongy bone, consisting of honycomb, needle-like, or flat pieces, called trabeculae.
Distribution of compact and spongy or cancellous bones
Microscopic structure of bone
Compact bone : The structural unit of compact bone is the osteon, or the Haversian system, which consists of concentric sheets of bone matrix (called the lamellae) surrounding a central Haversian canal. In other words. The whole complex of concentric lamella surrounding a canal is called a Harversian system, or osteon
Each Haversian system consists of:
Spongy bone : The spongy bone has no Haversian system but has trabeculae that align along the line of stress,and contain irregular lamellae.
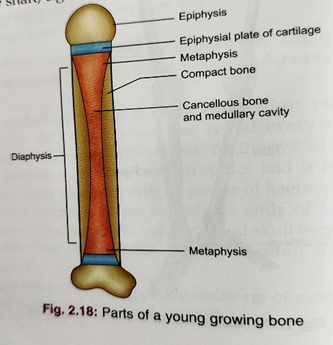
Parts of a Growing Long Bone
(1) Diaphysis: The portion of a long bone between the two cartilaginous ends is known as diaphysis. It is the elongated shaft of the bone which ossifies from the primary centre of ossification that develops first in the hyaline cartilage model of the future bone.
(2) Epiphyses: The two cartilaginous ends of a growing long bone are known as epiphyses. They develop from secondary centres of ossification. Epiphyseal plate of cartilage It is a plate of thin layer of epiphyseal cartilage which connects each epiphysis to the diaphysis. Epiphyseal line -The peripheral margin of the epiphyseal cartilage is known as epiphyseal line.
Types of epiphysis
(3) Metaphysis: It is the epiphyseal end of diaphysis of young growing bone adjacent to the epiphyseal cartilage. Metaphysis is the site of advancing ossification.Importance of metaphysis
4. PHYSIOLOGY OF BONE
Bone cells : The cells of bone are:
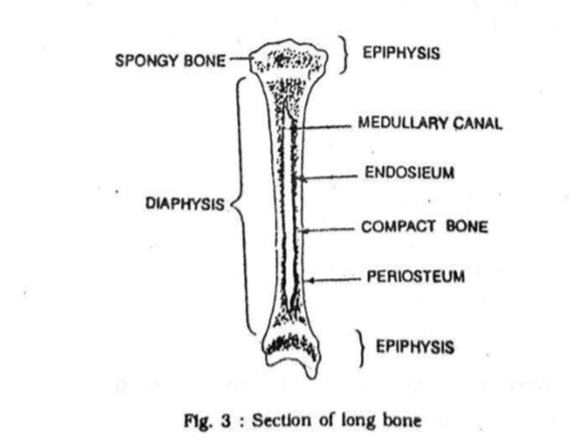
PERIOSTEUM : Periosteum is a thick fibrous membrane covering the surface of the bone except the articular surface.Structurally it consists of two layers:
Functions of periosteum:
ENDOSTEUM : Endosteum is a thin vascular membrane which lines the inner surface of the bony tissue that forms the medullary cavity of all the long bones. It is composed of a single layer of flattened osteoprogenitor cells and a very small amount of connective tissue. The endosteum, along with the periosteum functions for the growth of bone in diameter. The endosteum takes part in bone repair and remodeling.
BONE MARROW : The bone marrow is a soft, spongy, gelatinous tissue found in the medullary cavity of long bones and the spaces between the trabeculae of the spongy part of all bones. Types: two types – red and yellow bone marrow.
Red bone marrow It is the centre for haemopoiesis (production of blood cells).At birth, the marrow of all the bones of the body is red and haemopoietic. By about 7 years of age, yellow bone marrow appears in the middle of the shafts of long bones replacing the red bone marrow. With age, more and more of it is converted to the yellow type. In an adult, roughly half of the bone marrow is still red.In adults, red bone marrow is restricted to the bones of the skull, the vertebral column, sternum, ribs, pelvis, and the metaphyseal and epiphyseal ends of the long bones such as the humerus, tibia and femur.
Yellow bone marrow Yellow bone marrow is contained in the medullary cavity of the diaphyseal portion or the shaft of long bones. By the time a person reaches old age, nearly all of the red marrow is replaced by Yellow marrow. Yellow bone marrow is composed mainly of cells containing fat which accounts for its colour. Functions of bone marrow:
5 T.S of Bone 2
6. TYPES OF BONES
According to region:
According to size and shape :
According to ossification (development):
According to structure:
1. Macroscopically:
2. Microscopically (according to organization of collagen fibres):
Long Bones : Long bones are found in the limbs, eg. the clavicle, humerus, femur, radius, ulna, tibia and fibula, The length of the long bones is greater than that of their breadth.
Short Long Bones (Miniature Long Bones) : Short long bones are found in the hand and foot, e.g. metacarpals, metatarsals and phalanges. These bones are miniature in size. They have only one epiphysis. The length of the bones exceeds other measurements,
Short Bones : Short bones are also found in the wrist and ankle, e.g. the scaphoid, lunate, talus, and calcaneum. Short bones are cuboidal in shape. Short bones are composed of cancellous bone surrounded by a thin layer of compact bone. Short bones are covered with periosteum, and the articular surfaces are covered by hyaline cartilage.
Flat Bones : Flat bones are found in the vault of the skull (e.g. frontal and parietal bones), chest wall (e.g. ribs. sternum and scapula).Flat bones are composed of thin inner and outer plates of compact bone (the tables), separated by a layer of spongy or cancellous bone (the diploe).
Irregular Bones : Irregular bones are bones with various shapes. These bones are found in the base of the skull and the face (e.g. temporal, sphenoid, ethmoid, zygomatic, maxilla, mandible); vertebral column (e.g. vertebrae) and pelvis (e.g. hip bone).They are composed of a thin shell of compact bone with an interior made up of cancellous bone.
Pneumatic Bones : Certain flat or irregular bones contain a large hollow space within their body which contains air. Air-filled spaces make these bones lighter, e.g. maxilla, sphenoid, ethmoid, and mastoid part of the temporal bone. Function: Pneumatic bones make the skull light in weight, help in resonance of voice, and act as air conditioning chambers for the inspired air.
Sesamoid Bones : Sesamoid bones are round or oval small bones that are formed within tendon where the tendon passes over a joint. The greater part of a sesamoid bone is buried in the tendon, and the free surface is covered with cartilage. The largest sesamoid bone is the patella, which is located in the tendon of the quadriceps femoris. Other sesamoid bones are found in the tendons of the flexor pollicis brevis and flexor hallucis brevis. The function of sesamoid bone is to reduce friction on the tendon; to alter the direction of pull of a tendon.4
7. DEFINITION OF A FRACTURE
A fracture is defined as a break in the continuity of a bone, either complete or incomplete, resulting from trauma, repetitive stress, or pathological weakening. It may involve the bone alone or extend into the adjacent soft tissues, joints, or skin. Fractures are broadly classified according to their morphology, mechanism, and involvement of surrounding structures.5
8. TYPES OF FRACTURE
1.Classification Based on Skin Integrity
Fractures are first divided based on whether the skin overlying the fracture site remains intact or not:
2. Classification Based on Fracture Line (Morphology)
Fractures can also be categorized according to the orientation and pattern of the fracture line
3. Classification Based on Location
Fractures may be described by their anatomical location within the bone:
In children, growth plate (physeal) injuries are further classified according to the Salter-Harris system (Types I–V)8
4. Classification Based on Stability
Fractures can be categorized based on their inherent stability and tendency to displace:
5. Special Types of Fractures
6. Pediatric-Specific Fracture Types
Due to the unique properties of growing bone, certain fracture types occur predominantly in children:
9. CLINICAL FEATURES OF FRACTURES
Fractures, defined as a break in the continuity of bone, are common injuries in both traumatic and pathological contexts. Recognizing the clinical features of fractures is essential for timely diagnosis and management. These features vary depending on the type, location, and severity of the fracture.
1. Pain
Pain is the most immediate and prominent symptom following a fracture. Pain was usually localized to the site of the fracture and is exacerbated by movement or weight-bearing. This pain results from periosteal irritation, muscle spasm, and stimulation of nerve endings by bone fragments. In some cases, pain may be referred or minimal in cases of pathological fractures.10
2. Swelling and Edema
Swelling occurs soon after a fracture due to bleeding from bone and surrounding soft tissue. This inflammatory response leads to fluid accumulation, which may contribute to increased pressure and discomfort in the affected area. The extent of swelling can be an indirect indicator of the severity of the injury.12
3. Deformity
Visible or palpable deformity is a key sign of displaced fractures. Angular displacement, rotation, or shortening of the limb may occur, especially in long bone fractures. Deformities suggest significant displacement or comminution of the bone, requiring prompt orthopedic assessment.8
4. Loss of Function
Fractures often impair the function of the affected limb or body part. This may manifest as inability to bear weight, grip, or perform movements, depending on the site involved. The loss of function results from pain, mechanical disruption, or associated soft tissue injury.13
5. Crepitus
Crepitus refers to a grating or crackling sound felt or heard when fractured bone ends rub against each other. While considered a classic sign, it should not be elicited deliberately as it may exacerbate soft tissue injury or displace bone fragments14.
6. Bruising (Ecchymosis)
Bruising may develop hours to days after the fracture due to subcutaneous bleeding. It is particularly common in areas with a rich vascular supply, such as around the femur, arm, or facial bones. The extent and timing of bruising can sometimes help in estimating the age and severity of the fracture.15
7. Abnormal Mobility
In cases where a complete fracture results in discontinuity of the bone, there may be abnormal movement at the fracture site. This movement is often painful and can be detected during clinical examination, though care should be taken to avoid manipulation that could worsen injury.16
8. Neurovascular Compromise
Fractures may be associated with injury to nearby nerves and blood vessels, leading to numbness, pallor, coolness, or absence of pulses distal to the site of injury. This is especially important in high-risk areas such as the supracondylar humerus or femur. Early recognition is critical to prevent ischemic complications.17
9. Systemic Features (in Severe Cases)
In severe trauma or multiple fractures, systemic signs such as shock, tachycardia, or fever may occur. Open fractures or fractures with extensive soft tissue injury may predispose to infection and systemic inflammatory response. Fat embolism syndrome is a rare but serious complication seen in long bone fractures.18
10. Irregularity or palpable gap:
Discontinuity felt along the surface of the bone.8
11.Abnormal attitude or posture:
The patient holds the limb in a position that relieves pain
12. Muscle spasm:
Protective spasm of muscles around the site.General signs:Shock may occur in major fractures.
Associated injuries, vascular or nerve damage, and systemic manifestations such as fever or fat embolism may be present.8
10. INVESTIGATIONS
Plain X-ray : Radiography is the primary and most essential investigation for diagnosing a fracture. It should always be obtained in two perpendicular views, most often anteroposterior and lateral. Each radiograph must include the joint above and joint below the suspected site of injury.
Special X-ray views : Certain situations require additional views: Stress views to assess instability or ligamentous injury. Traction views, especially in fractures near the hip, to reveal the true displacement and assist in planning reduction
CT Scan (Computed Tomography) : A CT scan is particularly useful when the fracture pattern is complex, especially in regions where the joint surface is involved. It gives a clearer picture of Intra-articular fractures.
MRI (Magnetic Resonance Imaging) : MRI is valuable when a fracture is suspected but not visible on X-ray.It is especially indicated in: Occult fractures such as of the proximal femur, Stress fractures, injuries with significant soft-tissue involvement. MRI can identify :Ligament tears , Tendon injuries ,Meniscal damage ,Cartilage lesions.
Bone Scan (Scintigraphy) :A bone scan is helpful when other imaging does not show the fracture clearly.It is highly sensitive for: Early stress fractures ,Occult fractures ,Multiple fractures.
Ultrasonography :Ultrasound has limited but specific use in fracture evaluation. It can help detect: Hematoma at the fracture site ,Some occult fractures especially in children , Associated soft-tissue injuries.
Laboratory Investigations : These tests do not diagnose fractures.They are done to evaluate the patient’s general health, fitness for surgery, and any systemic issues related to trauma.
Routine tests include: Hemoglobin and complete blood count ,Blood grouping and cross-matching ,Blood sugar ,Renal function ,Electrolytes ,Coagulation profile. 19
11. GENERAL MANAGEMENT:
Management of Fractures
1. Objectives of Treatment
The primary goals in fracture management are to:
2. Principles of Fracture Management – “4 R’s”
Fracture treatment traditionally follows the “4 R’s” approach:
3. Non-operative Management
4. Operative Management
5. Rehabilitation
12. HOMOEOPTHIC APPROACH: SYNTHESIS TREASURE EDITION 2009V(SCHORENS F)
GENERALITIES – INJURIES Bones: Fractures of
GENERALS - INJURIES - Bones; fractures of: (59) acon. ang. anthraci. Arn. asaf. asar. bell-p. bell-p-sp. bry. calc. calc-ar. Calc-f. calc-i. calc-p. Calen. CARB-AC. con. cortico. cortiso. croc. crot-h. des-ac. dulc. Eup-per. ferr. fl-ac. hecla hep. HYPER. iod. kali-i. Lach. led. lyc. mang-act. mang-mix. merc. Mez. nit-ac. Petr. Ph-ac. phos. Puls. ran-b. rhus-t. rob. RUTA sep. Sil. SPIG. staph. stront-c. succ-ac. Sul-ac. sulph. Symph. Thyr. valer. vanil.
GENERALS - INJURIES - Bones; fractures of - compound fracture: (5) ARN. Calen. crot-h. hyper. Lach.
GENERALS - INJURIES - Bones; fractures of - slow repair of broken bones: (29) anthraci. asaf. CALC. calc-ar. calc-f. calc-i. CALC-P. calen. des-ac. Ferr. fl-ac. iod. lyc. mang-act. mang-mix. merc. Mez. nit-ac. Ph-ac. phos. puls. RUTA sep. Sil. staph. succ-ac. sulph. SYMPH. Thyr.
GENERALS - INJURIES - Bones; fractures of - slow repair of broken bones - children; in: (4) Calc. Calc-f. Calc-p. sil.21
13. CASE:
Name: [XXXXXX], Age/Sex: 35 years/Female, Occupation: Government school Teacher, Chief Complaints Fracture of femur following an accident, operated surgically, but with delayed healing (3 months). Gastric complaints developed after prolonged allopathic treatment.
History of Present Illness The patient met with a road traffic accident and sustained a fracture of the femur bone associated with an open wound. She was immediately admitted to a hospital, consulted with an orthopedic surgeon, and underwent surgical fixation. Postoperatively, despite regular follow-up and medical care, after three months there was no notable symptomatic relief. The surgical wound showed delayed healing, and the patient developed gastric discomfort and indigestion, likely secondary to analgesic and antibiotic usage. Due to these persisting complaints, she sought Homoeopathic treatment.
Past History No history of any major illness prior to the accident. No known drug allergy. General Examination Patient was moderately built and nourished. The operated wound was partially healed with mild tenderness and slow granulation tissue formation. Diagnosis: Fracture shaft of femur (post-operative, delayed union). Gastritis due to prolonged conventional medication.
Follow-Up and Outcome. After the commencement of Homoeopathic treatment, gradual improvement was noted. Wound healing progressed satisfactorily. Radiological evidence showed bony callus formation and improved union. Gastric complaints subsided completely. The patient returned to normal mobility and daily activities.
Conclusion: This case demonstrates the role of Homoeopathic treatment in promoting wound healing, aiding bone repair, and addressing associated gastric complaints after a surgical procedure for fracture.
Before Treatment
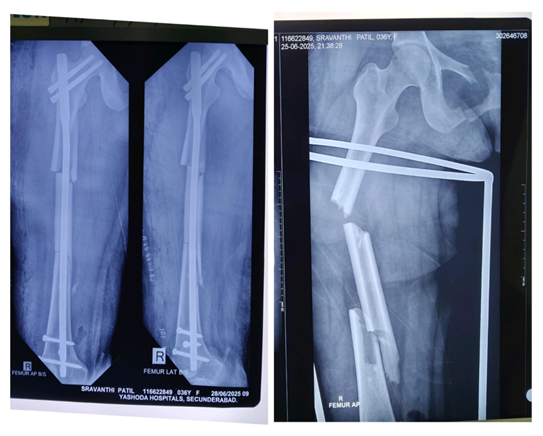
The X-ray images show a comminuted fracture of the right femur shaft with displacement
There are multiple fragments (comminution) evident in the femoral shaft.The alignment is maintained surgically with an intramedullary nail and interlocking screws, indicating the patient had operative fixation (intramedullary nailing). The right side is indicated (R). The second image (on the right) shows the initial fracture pattern before surgical fixation, with the bone clearly broken into more than two pieces. This is a comminuted, displaced fracture of the right femoral shaft that has been treated with intramedullary nailing.
During Treatment

Wound Healing



DISCUSSION:
Bone, as a dynamic connective tissue, demonstrates remarkable resilience and regeneration due to its composite structure of inorganic calcium salts and organic collagen fibers. This dual composition enables resistance to both compressive and tensile forces, permitting bones to bear physical stress while maintaining flexibility. Following injury or fracture, bones exhibit an exceptional capacity for self-repair, directed by highly vascularized tissue and constant remodeling activities. However, the healing process is multifaceted, often challenged by issues such as pain, delayed union, and impaired tissue regeneration, particularly in complex or compound fractures.
In response to these challenges, the integration of homeopathic remedies with conventional orthopedic strategies has gained research attention. Remedies such as Arnica montana, Symphytum officinale, Ruta graveolens, Calcarea phosphorica, Calcarea carbonica, and Hypericum have been documented for their roles in reducing pain, minimizing swelling, and accelerating callus formation. Individualized homeopathy protocols have demonstrated promising outcomes, including faster radiological union and functional recovery, as well as a potential reduction in analgesic requirements when used as adjuncts to standard care. These benefits are particularly relevant in cases where traditional approaches alone may not meet patient needs for pain management and tissue regeneration.
Nonetheless, while clinical observations and emerging studies suggest significant benefits, there is still a critical need for rigorous, controlled trials to firmly establish the efficacy, safety, and reproducibility of homeopathic interventions in bone fracture management. The holistic perspective—encompassing anatomy, biomechanics, and alternative therapies—offers a comprehensive framework for enhancing patient recovery, but demands further substantiation through high-quality clinical research.
CONCLUSION:
Bone is a uniquely dynamic and adaptive connective tissue capable of remarkable structural support, physiological regulation, and regeneration. Its mineralized matrix, collagen framework, and continuous remodeling capacity enable it to withstand mechanical stresses and repair itself efficiently following fractures. Understanding the anatomy, physiology, and ossification processes of bone provides essential insight into the biomechanics of fracture healing and the factors influencing successful recovery.
Fracture management traditionally relies on orthopedic stabilization, but challenges such as pain, inflammation, delayed union, and compromised callus formation often necessitate supportive measures. In this context, individualized homeopathic interventions—particularly remedies such as Arnica montana, Symphytum officinale, Ruta graveolens, Calcarea phosphorica, Calcarea carbonica, and Hypericum—have shown potential in enhancing healing outcomes. Clinical observations suggest that these remedies may reduce pain, support early tissue recovery, stimulate callus formation, and improve functional results when used alongside standard medical care.
While emerging evidence highlights the promise of integrating homeopathy into fracture management, further well-designed clinical studies are required to validate efficacy, define therapeutic protocols, and ensure reproducible outcomes. A holistic approach that combines foundational anatomical knowledge, conventional orthopedic principles, and evidence-based complementary therapies may ultimately offer improved patient care and more comprehensive fracture rehabilitation.
ACKNOWLEDGEMENT
I extend heartfelt thanks to Director Dr. Umesh Akkaladevi Sir, Principal Prof. Dr. Nurus Saher Khan Madam. Hamsa Homoeopathy Medical College Hospital & Research Centre. my mentors, colleagues, and peers for their guidance, constructive suggestions, and encouragement throughout the preparation of this work.
CONFLICT OF INTEREST:
The author declares that there is no conflict of interest regarding the publication of this study. This work was conducted independently without any financial, commercial, or personal relationships that could have influenced the content, interpretation, or conclusions of the study.
REFERENCE


Dr. Srinivas Babu Kathi, Dr. Kavya Boini, Dr. Puli Pooja, Dr. Banoth Sandhya, Dr. Suguri Sravan Kumar, Dr. Satvik Bopparaju, Dr. Shaik Rakeeb Ali Ahmed, Dr. Kadarla Pranay, Structural Diversity, Adaptive Capacity, and Alternative Healing: A Study on Bone Anatomy & Pathophysiology, Fracture Care, and Homeopathic Interventions, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 3854-3871. https://doi.org/10.5281/zenodo.17700215
 10.5281/zenodo.17700215
10.5281/zenodo.17700215
