Department of Pharmacology, BVV Sangha’s Hanagal Shri Kumareshwar College of Pharmacy Bagalkote-587101, Karnataka, India.
Parkinson's disease (PD) is complex neurodegenerative disorder characterised by both motor and non-motor symptoms. Levodopa treatment effectively address motor manifestations but the management of non-motor features remains clinically challenging. Tricyclic antidepressants (TCAs) is largely superseded by newer antidepressant classes that possess unique multimodal pharmacological profile that warrants re-evaluation in PD therapeutics. Current evidence demonstrating that TCAs offer dual-pathway benefits that robust symptomatic control of depression, anxiety, chronic pain and autonomic dysfunction, coupled with potential disease-modifying effects through anti-inflammatory, anti-apoptotic, mitochondrial protective and neuroplasticity-enhancing mechanisms. Molecular pathways through which TCAs modulate neuroinflammation, enhance mitochondrial bioenergetics and promote neuronal survival, while addressing the clinical challenges and strategic implementation of these agents in PD management. The integration of TCAs into personalized treatment paradigms requires careful consideration of their risk-benefit profile, particularly in vulnerable populations that offer significant advantages for patients with complex symptoms profiles refractory to first-line interventions.
PD affects approximately 2-3% of the population over 65 years globally and prevalence projects and indicates that double in 2040 due to demographic aging [1]. While the traditional therapeutic only focus on motor symptoms, the critical impact of non-motor manifestations on quality of life has gained increasing recognition. Depression affects 40-50% of PD patients, while pain, sleep disturbances and autonomic dysfunction collectively contribute significantly to disability and reduced quality of life [2].
The pharmacological management of PD has been dominated by dopaminergic therapies, particularly levodopa/carbidopa combinations. However, the treatment of neuropsychiatric comorbidities presents unique challenges that extend beyond dopamine replacement. While selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) represent first-line options for depression management, Tricyclic Antidepressants (TCAs) offer a multifaceted therapeutic profile that may simultaneously address several PD-specific pathophysiological processes [3].
The prevalence of depression in PD substantially exceeds that in the general population, with distinctive features including higher rates of anxiety, apathy, and anhedonia [4]. Furthermore, the noradrenergic deficit resulting from locus coeruleus degeneration in PD may render purely serotonergic antidepressants less effective for certain symptom domains. This neurobiological rationale coupled with emerging understanding of TCA neuroprotective properties, justifies a comprehensive re-examination of their role in modern PD management.
The neuropathology of PD involves significant degeneration of the noradrenergic locus coeruleus, contributing substantially to symptoms of apathy, fatigue, and impaired attention. This noradrenergic deficit is increasingly recognized as a fundamental driver of non-motor disability in PD [5]. TCAs with potent norepinephrine reuptake inhibition properties (e.g., nortriptyline, desipramine) directly address this neurochemical deficit. A randomized controlled trial by Menza et al. demonstrated that nortriptyline produced significantly greater improvement in depressive symptoms compared to placebo in PD patients (68% response rate vs. 32%), with particular efficacy for symptoms of apathy and anhedonia [6]. The noradrenergic enhancement provided by these agents may also improve cognitive aspects such as sustained attention and processing speed, domains frequently impaired in PD.
The therapeutic advantage of TCAs over selective serotonergic agents for apathy management stems from their direct action on the mesocorticolimbic dopamine system. By increasing norepinephrine availability in the prefrontal cortex, TCAs indirectly enhance dopaminergic neurotransmission in circuits critical for motivation, reward processing, and executive function [7]. This effect is particularly relevant given the limited efficacy of direct dopaminergic therapies for non-motor symptoms such as apathy.
Through dual noradrenergic enhancement and sodium channel blocking effects, TCAs effectively address both central sensitization and peripheral pain mechanisms. A systematic review by Skapinakis et al. confirmed their efficacy in PD-related pain syndromes with number needed to treat (NNT) of 4.3 for neuropathic pain components [8]. The analgesic effects manifest independently of mood improvement, providing additional therapeutic value. The descending noradrenergic pain inhibitory pathways, which originate in the locus coeruleus and project to the spinal cord dorsal horn, are particularly relevant in the context of PD-related pain [9]. By enhancing noradrenergic signalling, TCAs restore the function of these compromised inhibitory pathways.
The histamine H1 receptor antagonism of sedating TCAs (e.g., amitriptyline, doxepin) provides rapid relief for insomnia, often within the first administration. This effect is particularly valuable in PD patients experiencing sleep maintenance insomnia and frequent nocturnal awakenings. Furthermore, TCAs may reduce REM sleep behavior disorder symptoms through their serotonergic modulation [10]. The sleep-enhancing properties extend beyond simple sedation, with evidence suggesting that TCAs can increase slow-wave sleep and improve sleep continuity in PD patients [11]. Anticholinergic properties can be therapeutically harnessed to reduce sialorrhea, a socially disabling symptom affecting up to 70% of PD patients. This effect, mediated through muscarinic receptor blockade in salivary glands, provides an alternative to localized botulinum toxin injections [12]. While anticholinergic burden must be carefully considered, the targeted use of TCAs for sialorrhea management in selected patients represents a valuable therapeutic option.
2. Neuroprotective Mechanisms: Molecular Pathways and Therapeutic Potential.
Neuroinflammation represents a critical driver of PD progression, characterized by chronic microglial activation, astrocytic dysfunction, and pro-inflammatory cytokine release. TCAs demonstrate significant anti-inflammatory properties through multimodal pathway regulation. TCAs suppress microglial activation by inhibiting the NLRP3 inflammasome and nuclear factor kappa-B (NF-κB) signaling pathways. Experimental studies by Liu et al. demonstrated that nortriptyline reduces production of interleukin-1β (IL-1β) and tumor necrosis factor-alpha (TNF-α) through AMP-activated protein kinase (AMPK)-dependent mechanisms, with dose-dependent suppression observed in the 10-50 μM range [13]. This effect disrupts the vicious cycle of neuronal damage and inflammatory activation that characterizes PD progression. Additionally, TCAs promote microglial polarization toward the neuroprotective M2 phenotype, enhancing production of anti-inflammatory cytokines including IL-10 and transforming growth factor-beta (TGF-β) [14].
The anti-inflammatory effects of TCAs extend beyond microglial modulation to include direct actions on neuronal survival pathways. By reducing the production of pro-inflammatory mediators, TCAs mitigate excitotoxicity and oxidative stress, both of which contribute significantly to dopaminergic neuron vulnerability in PD [15]. Beyond microglial modulation, TCAs enhance astrocytic function through β-adrenergic receptor signaling, improving glutamate clearance via upregulation of GLT-1 and GLAST transporters and increasing neurotrophic factor release. This glial support contributes to neuronal resilience against excitotoxicity and oxidative stress, both prominent in PD pathogenesis [16]. The astrocytic glutamate transporter upregulation is particularly relevant given the evidence of glutamatergic excitotoxicity in PD progression. Mitochondrial dysfunction represents a cornerstone of PD pathogenesis, affecting complex I activity and oxidative phosphorylation. TCAs address these deficiencies through multiple mechanisms, Activation of the PGC-1α pathway increases mitochondrial mass and functional capacity, potentially counteracting the reduced mitochondrial content observed in PD substantia nigra neurons [17].
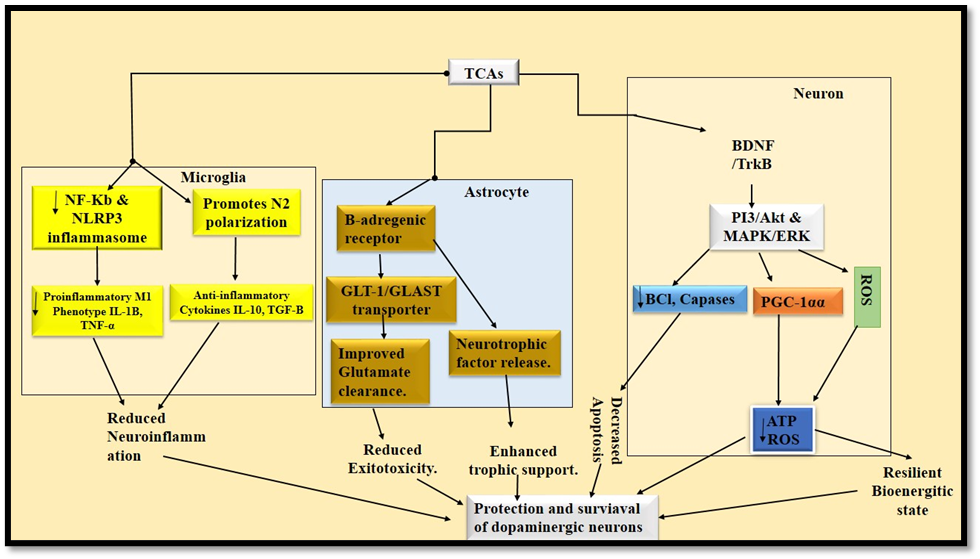
Figure 1: Tricyclic Antidepressants (TCAs) exert neuroprotection through integrated glial and neuronal mechanisms. They suppress microglial-driven neuroinflammation by inhibiting the NF-κB pathway and NLRP3 inflammasome, reducing pro-inflammatory cytokines (e.g., IL-1β, TNF-α). In astrocytes, TCAs enhance β-adrenergic signaling, boosting glutamate clearance and neurotrophic release. For neurons, TCA-induced BDNF activates PI3K/Akt and MAPK/ERK pathways, inhibiting apoptosis, while PGC-1α upregulation improves mitochondrial function and counters oxidative stress.Image created by PowerPoint (ppt)
Reduction of electron transport chain dysfunction and reactive oxygen species (ROS) production through stabilization of complex I and III activities [18]. Through direct antioxidant effects and enhanced cellular defense mechanisms, including upregulation of glutathione synthesis and superoxide dismutase activity [19]. The mitochondrial protective effects of TCAs are particularly relevant given the central role of mitochondrial dysfunction in PD pathogenesis. By improving cellular bioenergetics and reducing oxidative stress, TCAs address fundamental mechanisms underlying dopaminergic neuron vulnerability.The pro-survival effects of TCAs are mediated through robust activation of the PI3K/Akt pathway, inhibiting pro-apoptotic factors including Bad, Bax, and caspase-9 while upregulating anti-apoptotic Bcl-2 expression. This creates a powerful protective environment for vulnerable dopaminergic neurons against various apoptotic stimuli, including those induced by α-synuclein aggregates and mitochondrial toxins [20].
The anti-apoptotic effects of TCAs involve both genomic and non-genomic mechanisms. Through rapid activation of membrane-associated signaling pathways and subsequent regulation of gene expression, TCAs create a sustained anti-apoptotic environment that enhances neuronal resilience [21]. This multi-level approach to apoptosis inhibition represents a significant advantage over targeted therapies addressing single apoptotic pathways. Chronic TCA administration activates intracellular cascades (cAMP/PKA, MAPK/ERK) that phosphorylate CREB, driving Brain-Derived Neurotrophic Factor (BDNF) expression. Enhanced BDNF signaling supports multiple neuroprotective processes:
The BDNF-enhancing effects of TCAs are particularly relevant given the documented reductions in BDNF levels in PD patients [23]. By restoring neurotrophic support, TCAs may promote compensatory plasticity and slow disease progression, representing a potential disease-modifying effect beyond symptomatic benefits.
3. Clinical Application and Risk Mitigation Strategies
3.1 Strategic Patient Selection Criteria
TCAs are particularly suitable for PD patients presenting with specific symptom clusters:
Careful patient selection is paramount, with particular attention to contraindications including significant cognitive impairment, cardiac conduction abnormalities, narrow-angle glaucoma, and prostatic hypertrophy. The presence of these conditions typically precludes TCA use due to increased risk of serious adverse events.
3.2 Agent Selection and Dose Optimization
The principle of "start low and go slow" is particularly important in PD patients, who often demonstrate increased sensitivity to medication side effects. Therapeutic drug monitoring, when available, can guide dose optimization while minimizing adverse effects [24].
3.3 Comprehensive Monitoring and Safety Protocols
The implementation of systematic monitoring protocols can significantly enhance the safety profile of TCAs in vulnerable PD populations. Particular attention should be paid to potential drug interactions, especially with other anticholinergic agents and medications affecting cardiac conduction.
4. Integrating Evidence into Clinical Practice
The dual-pathway utility of TCAs in PD represents a unique therapeutic opportunity that bridges symptomatic management and potential disease modification. While their symptomatic benefits are well-established in specific clinical contexts, the emerging evidence for neuroprotective effects warrants serious consideration in the broader therapeutic strategy for PD.
The principal clinical challenge lies in balancing these potential benefits against the well-documented risks, particularly in vulnerable populations such as elderly patients with cognitive impairment or cardiovascular comorbidities. The anticholinergic burden associated with TCAs necessitates careful cognitive monitoring, while the potential for orthostatic hypotension requires systematic cardiovascular assessment.
The multimodal pharmacological action of TCAs—simultaneously addressing noradrenergic deficiency, pain pathways, sleep architecture, and neuroinflammatory processes—provides a comprehensive approach to PD management that newer, more selective antidepressants cannot replicate. This broad-spectrum activity may be particularly advantageous in PD patients with multiple co-occurring non-motor symptoms, potentially reducing polypharmacy and simplifying treatment regimens.
Future research directions should prioritize:
6. CONCLUSION
TCAs represent a valuable, though underutilized, therapeutic option in Parkinson's disease management. Their unique capacity to address multiple non-motor symptoms while potentially modifying underlying disease processes through anti-inflammatory, neurotrophic, and mitochondrial protective mechanisms positions them as dual-pathway therapeutics. The evidence supporting their neuroprotective effects, while primarily preclinical, provides a compelling rationale for their considered use in selected PD patients.
The integration of TCAs into personalized treatment paradigms requires thoughtful consideration of individual patient characteristics, comorbidities, and treatment goals. While safety concerns necessarily limit their use as first-line agents, their potential benefits in specific clinical contexts underscore the continued relevance of these classic psychotropic medications in modern neurology practice. With careful patient selection, appropriate agent choice, and vigilant monitoring, TCAs can provide significant benefits for PD patients with complex symptom profiles that have proven refractory to first-line interventions.
As our understanding of PD pathophysiology evolves, the multimodal mechanisms of TCAs may assume increasing importance in developing comprehensive treatment strategies that address both symptomatic burden and disease progression. Future research exploring the optimal integration of these agents into PD management protocols will be essential for fully realizing their therapeutic potential.
ACKNOWLGEMENT:
We are grateful to the Department of Pharmacology, B.V.V.S Hanagal Shri Kumareshwar College of Pharmacy Bagalkote for providing all the needful to carry out this review work.
Abbreviations:
Conflicts Of Interest:
The authors declare no conflict of interest
Funding
Not Applicable
REFERENCES

Rakesh Bagle, Bhumika, Shubham Teli, Chandrashekhar V. M., Mallappa Shalavad*, The Dual-Pathway Utility of Tricyclic Antidepressants in Parkinson's Disease: Integrating Neuroprotective Mechanisms with Symptomatic Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1344-1351 https://doi.org/10.5281/zenodo.17571230
 10.5281/zenodo.17571230
10.5281/zenodo.17571230
