1Dean Academics, Sai Nath University, Ranchi, Jharkhand 835219, India.
2Associate Professor, Department of Pharmacy, Sai Nath University, Ranchi, Jharkhand 835219, India.
3Student, B. Pharm, Department of Pharmacy, Sai Nath University, Ranchi, Jharkhand 835219, India.
4Assistant Professor of Pharmacology, Department of Pharmacy, Faculty of Medical Science and Research, Sai Nath University, Ranchi, Jharkhand 835219, India
The relentless pursuit of competitive advantage in sports has fueled the widespread misuse of performance-enhancing substances (PESs) and doping practices, posing significant ethical and health concerns. This comprehensive review delves into the historical and contemporary perspectives on doping, examining the intricate classifications of prohibited substances and methods outlined by the World Anti-Doping Agency (WADA). It provides an in-depth exploration of various PESs, including anabolic-androgenic steroids, peptide hormones, stimulants, narcotics, and blood doping techniques, elucidating their mechanisms of action and performance-enhancing effects. The review also addresses the physiological responses induced by exercise, their impact on drug pharmacokinetics, and the challenges associated with doping detection. Furthermore, it highlights the spectrum of sports-related injuries, emphasizing the importance of comprehensive rehabilitation strategies and the judicious use of medications. The pivotal role of sports pharmacology and pharmacy in promoting athlete health, preventing inadvertent doping, and fostering fair competition is underscored. The review advocates for the integration of sports pharmacology into medical curricula and the establishment of structured training programs to equip healthcare professionals with the necessary knowledge and skills to navigate the complexities of medication use in athletes. Interprofessional collaboration among sports pharmacologists, pharmacists, and other healthcare providers is emphasized as a crucial component in optimizing athlete care and safeguarding the integrity of sports competitions.
In today's highly competitive sports environment, the focus has shifted from the honor of winning to the lucrative multimillion-dollar endorsements and contracts. As a result, athletes often compromise their integrity and take significant risks to gain a competitive edge and enhance performance. Milliseconds can determine the winner in modern sports, making any advantage crucial for securing medals and endorsements worth millions. Consequently, the use of performance-enhancing substances (PESs) has surged. Pharmacosanation, the study of biologically active substances that improve resistance to adverse factors, enhance recovery from biological stressors, or prevent illness, has proven beneficial in helping athletes manage the emotional and physical stresses of training and competition [1, 2, 3, 4]. A 1997 Sports Illustrated survey revealed that 98% of 198 aspiring US Olympians would take a banned PES if it guaranteed a win without detection, and half would do so even if it led to death after five years [5, 6, 7].Historically, the use of PES dates back to the Bible's "Garden of Eden" and the ancient Chinese Emperor Shen-Nung's use of "ma-huang" (Ephedra) in 2737 BC [8, 9]. Ancient Olympic athletes consumed herbal teas and mushrooms to boost performance, and South American athletes used stimulants like strychnine and cocaine[10,11,12]. The dangers of PESs were evident in the deaths of English cyclists Arthur Linton and Tom Simpson due to substance abuse[13,14,15]. In response, regulations were established to ban certain substances in sports[16]. High-profile cases, such as Jamaican sprinter Usain Bolt losing a gold medal because teammate Nesta Carter used a PES at the Beijing Olympics, highlight the widespread issue[17,18,19]. American sprinter Tyson Gay tested positive for a banned substance in 2013, resulting in a one-year ban and forfeiture of his 2012 Olympic silver medal[20,21,22]. Colombian cyclist Maria Luisa Calle Williams was banned for four years after testing positive for Heptaminol doping in 2015, despite winning a gold medal at the Pan American Games in 2011[23,24,25]. The prevalence of PES abuse among athletes underscores the need for stringent regulations and ongoing efforts to maintain fair competition and athlete health[26,27,28]. Exercise-Induced Physiological Responses and Their Influence on Pharmacokinetics: Implications for Enhancing Athletic Performance During exercise, vasodilation occurs in skeletal muscle arterioles, while vasoconstriction is observed in inactive areas of the body[29,30,31]. Factors such as increased local temperature, CO2 levels, lactic acid concentration, and enzymatic liver activity can lead to heightened excretion of drugs with low extraction ratios, such as caffeine and ibuprofen, thereby altering the pharmacokinetics and pharmacodynamics of these medications[32,33,34,35]. Skeletal muscles comprise various fiber types, including fast-oxidative glycolytic fibers, slow-oxidative fibers, and fast-oxidative glycolytic fibers[36]. Endurance events like marathon running primarily engage slow-oxidative fibers, whereas short, high-intensity endurance events like a 1-mile run predominantly involve fast-oxidative glycolytic fibers[37,38]. These fibers hypertrophy differently based on the type of exercise performed[39]. Endurance training increases the number of mitochondria and capillaries, particularly around slow-oxidative and fast-oxidative glycolytic fibers, while short-duration, high-intensity exercises like weightlifting result in hypertrophy of fast-oxidative glycolytic fibers[40,41]. During exercise, energy for short-duration, high-intensity activities is derived from immediate energy systems like anaerobic glycolysis and creatine phosphate, whereas oxidative phosphorylation mainly fuels endurance-type exercise[42,43,44]. Heart rate and stroke volume increase in proportion to exercise intensity, with stroke volume plateauing earlier than heart rate due to increased contractility and venous return[45,46]. This increased cardiac output primarily serves the active muscles, heart, and skin[47]. Endurance training boosts capillary density in muscles and stroke volume, while heart rate typically decreases at rest[48,49].Exercise is characterized by a rise in systolic blood pressure and, often, a slight decrease in diastolic pressure[50]. Plasma volume decreases during exercise due to increased capillary filtration and muscle oxygen consumption[51]. Adequate ventilation during exercise is ensured by neurogenic control of respiration, which facilitates sufficient blood oxygenation even during intense physical activity[52]. Ultimately, the ability of the heart to pump blood to the muscles determines exercise capacity. The use of medications to modify physiological responses and enhance endurance and exercise capacity is common among athletes.[53]
Historical and Contemporary Perspectives on Doping in Sports
The historical use of artificial methods to enhance performance in sports dates back to ancient times, evidenced by the abuse of substances like opium in horses in 1889 and the exploitation of mushrooms, plants, and herbal mixtures by Roman gladiators and Greek Olympic athletes as far back as 776 BC [54,55,56]. Throughout history, various stimulants such as caffeine, heroin, strychnine, and cocaine have been combined and abused by athletes, with amphetamines emerging as a popular stimulant in the 1930s [57,58].
Notably, the use of male hormones by the Soviet Olympic team in the 1950s and the revelation of East Germany's state-sponsored program for performance enhancement following the fall of the Berlin Wall underscore the pervasive nature of doping in sports [59,60]. Subsequent efforts by organizations like the International Olympic Committee (IOC) and law enforcement agencies, such as the discovery of banned substances like erythropoietin during the 1998 Tour de France, have highlighted the need for robust measures to combat doping [61, 62]. In response to these challenges, the World Anti-Doping Agency (WADA) was established in 1999 to oversee and coordinate anti-doping efforts across all sports disciplines [63]. Comprising experts from various fields including sports medicine, pharmacology, physiology, pharmacy, genetics, and laboratory science, WADA releases an updated list of banned substances annually, categorizing doping substances and methods as prohibited at all times (in-competition and out-of-competition), substances prohibited only during competition, and substances prohibited in specific sports[64,65]. In accordance with the World Anti-Doping Agency (WADA), the term "doping" encompasses a range of scenarios within the realm of sports, including the presence of banned substances or their metabolites in an athlete's sample, whether through direct consumption or inadvertent exposure [66]. Additionally, doping extends to instances of actual or attempted use of prohibited substances or methods by athletes to gain a competitive advantage [67]. Failures or refusals to submit samples for testing, as well as evasive tactics to avoid testing altogether, are also considered doping violations [68, 69]. Furthermore, neglecting to report missed tests or whereabouts information constitutes a breach of anti-doping regulations [70, 71]. Any interference with the doping control process, such as tampering with samples or obstructing testing procedures, is likewise prohibited [72]. Moreover, the trafficking or attempted trafficking of banned substances or methods, whether for personal use or distribution to others, falls under the umbrella of doping [73]. Lastly, involvement in activities that promote, facilitate, or cover up doping practices, including administering prohibited substances to athletes or aiding in their use, constitutes a violation of anti-doping regulations and reflects an intentional complicity in doping-related activities [74,75,76].
The use of performance-enhancing drugs by athletes is universally condemned by major international sports organizations, such as the International Olympic Committee (IOC), on ethical grounds [77]. Not only does doping pose significant health risks and potential for permanent neurological damage to the athlete, but it also undermines the fundamental principles of fair play and integrity in sport [78]. However, exemptions to the ban on prohibited substances or methods are granted in cases where athletes have documented medical conditions necessitating the use of such substances or methods [79]. This process, known as a Therapeutic Use Exemption (TUE), involves thorough review of applications by the Therapeutic Use Exemption Committee according to predefined criteria to ensure that legitimate medical needs are met [80].
IOC's Prohibited Substances: Ensuring Fairness and Safety in Sports
The International Olympic Committee (IOC) has outlined a detailed list of prohibited substances for athletes, classified into several categories such as stimulants, narcotics, beta-blockers, masking agents, diuretics, peptide hormones, mimetics, and analogs, as well as anabolic steroids, beta-2 agonists, and other anabolic agents [81, 82, 83].
Stimulants banned by the IOC include compounds like amiphenazole, amineptine, amphetamines, bupropion, bromantan, cocaine, caffeine, ephedrines, fencamfamine, methylphenidate, mesocarb, pipradrol, pentetrazol, salbutamol, strychnine, and terbutaline. These substances can increase alertness and physical performance, offering an unfair advantage [84, 85, 86,87,88].
The list of prohibited narcotics comprises buprenorphine, dextromoramide, diamorphine (heroin), meperidine, methadone, morphine, and pentazocine [89,90]. These drugs are typically used for pain management but can also alter performance [91].
Beta-blockers
such as acebutolol, alprenolol, atenolol, betaxolol, esmolol, labetalol, metoprolol, nadolol, oxprenolol, and sotalol are restricted due to their ability to mitigate anxiety and reduce tremors, which can be advantageous in sports requiring precision[92,93].
Masking agents
like bromantan, epitestosterone, and probenecid are prohibited as they can conceal the presence of other banned substances in the body, making them undetectable during doping tests[94,95].
The diuretics
on the IOC's banned list include acetazolamide, bendroflumethiazide, bumetanide, chlorthalidone, canrenone, ethacrynic acid, furosemide, hydrochlorothiazide, spironolactone, and triamterene[96,97]. These substances promote water loss and can be used to achieve rapid weight reduction or to dilute urine, masking the presence of other drugs[98].
Prohibited peptide hormones, mimetics, and analogs include corticotrophins, erythropoietin, human chorionic gonadotropin (HCG, banned in males), human growth hormone, insulin (permitted only for certified insulin-dependent diabetes), insulin-like growth factor (IGF-I), and various gonadotropins (e.g., luteinizing hormone, clomiphene, cyclofenil, tamoxifen—all banned in males)[99,100]. These substances can significantly enhance muscle growth, recovery, and overall athletic performance[101]. The IOC's list of banned anabolic steroids and other anabolic agents features androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, clostebol, danazol, dehydrochlormethyl-testosterone, dehydroepiandrosterone, dihydrotestosterone, drostanolone, ethylestrenol, formebolone, fluoxymesterone, furazabol, mesterolone, metandienone, methandriol, methyl-testosterone, mibolerone, nandrolone, 19-norandrostenediol, 19-norandrostenedione, norethandrolone, oxandrolone, oxymesterone, oxymetholone, stanozolol, stenbolone, testosterone, and trenbolone[102,103,104]. These agents are known to enhance muscle mass and strength, providing a significant performance edge[105].
The stringent enforcement of these prohibitions is integral to the IOC's dedication to maintaining fair competition and safeguarding the health and safety of athletes[106,107].
Comprehensive Classification of Prohibited Substances and Methods by WADA
The World Anti-Doping Agency (WADA) classifies prohibited substances and methods into several categories, some of which are banned at all times, while others are restricted during competition or in specific sports[108]. Substances that are prohibited at all times include non-approved substances (S0), anabolic agents (S1), which are further divided into anabolic androgenic steroids (both exogenous and endogenous) and other anabolic agents[109]. Peptide hormones, growth factors, related substances, and mimetics fall under S2[110]. Beta-2 agonists are classified as S3, hormone and metabolic modulators as S4, and diuretics and masking agents as S5[111]. WADA also prohibits certain methods at all times[112]. These include the manipulation of blood and blood components (M1), chemical and physical manipulation (M2), and gene doping (M3)[113]. Substances that are specifically prohibited in-competition include stimulants (S6), which are categorized into nonspecified and specified stimulants, narcotics (S7), cannabinoids (S8), and glucocorticoids (S9). Additionally, beta-blockers (P1) are prohibited in particular sports[114,115]. Athletic performance is multifaceted, relying on four key dimensions: skill, strength, endurance, and recovery [116]. Each sport demands a unique combination of these elements for optimal performance [117]. Performance-enhancing substances (PESs), commonly referred to as performance-enhancing drugs (PEDs), offer advantages across these dimensions, providing enhancements tailored to the specific requirements of each sport. Below, we provide an overview of commonly utilized PESs [118,119].
Revealing the Intricacies of PESs in Enhancing Athletic Performance
Anabolic-androgenic steroids derive their name from their dual actions: anabolic effects that stimulate tissue growth and androgenic effects responsible for masculine characteristics. This duality has led to their misuse in sport to enhance performance. Gonadal steroids, including androgens and estrogens, exert significant influence on bone metabolism throughout the lifespan of both sexes. Their roles encompass vital functions such as growth, development, and maintenance of reproductive organs, as well as the promotion of protein Synthesis, resulting in increased muscle mass and weight. Additionally, they contribute to masculinization, overall growth, and bone maturation. Nandrolone, an injectable anabolic-androgenic steroid, possesses a prolonged half-life, facilitating the detection of its metabolites. Testosterone administration is commonly assessed through the epitestosterone glucuronide to testosterone glucuronide ratio, termed the "T/E ratio." Dihydrotestosterone, an endogenous compound, holds promise for eliciting anabolic effects due to its heightened affinity for the androgenic receptor. Indirect androgen doping strategies involve the use of compounds like clomiphene, raloxifene, and toremifene, or aromatase inhibitors such as aminoglutethimide, anastrozole, letrozole, and exemestane. Over the last 15 years, steroid precursors, notably anabolic steroid precursors or prohormones, have surged in popularity as performance-enhancing drugs (PEDs).

Fig. 1. MOA of Anabolic-Androgenic Steroids
An anabolic steroid is transported into the target tissue cell cytoplasm where it can either bind the androgen receptor, or be reduced by the cytoplasmic enzyme 5-alpha reductase. The N-receptor complex undergoes a structural change that allows its translocation into the cell nucleus, where it directly binds to specific nucleotide sequences of the chromosomal DNA. The produced DNA interferes with the physiological biosynthesis of testosterone.
2. Glucocorticoids [123, 124, 125]
Glucocorticoids, whether natural or synthetic, are steroid hormones renowned for their anti-inflammatory properties. These hormones orchestrate anabolic actions by stimulating processes such as gluconeogenesis and the utilization of amino acids and fatty acids. Additionally, they alleviate fatigue and inflammation, enhance mental alertness, and elevate pain tolerance. Glucocorticoids can induce ergogenic effects in both humans and animals, hence their inclusion on WADA's list of prohibited substances. However, athletes may apply for Therapeutic Use Exemptions (TUE) if they declare the use of glucocorticoids. It's noteworthy that topical formulations of glucocorticoids, when employed for specific medical conditions such as nasal, ophthalmic, auricular, buccal, dermatological (including iontophoresis/phonophoresis), gingival, and perianal disorders, are not banned and do not necessitate a TUE or declaration of use.

Fig. 2. MOA of Glucocorticoids
glucocorticoid after binding with glucocorticoid receptor forms GC-GR complex that exhibits two types of mechanism such as transactivation through its acetylation by HAT (histone acetyltransferase) and transrepression; through its deacetylation by HDAC2 (histone deacetylase 2) the transactivation mechanism it shows various anti-inflammatory effects whereas; transrepression mechanism exhibits numerous inflammatory effects.
3. Beta agonists [126, 127, 128]
Beta agonists are phenylethanolamines characterized by various substituents on the terminal amino group and the aromatic ring. Their utilization is prohibited in sports due to their stimulant and anabolic properties. Athletes are restricted from their usage unless they obtain prior valid medical authorization. However, salbutamol, a beta-adrenergic agonist, is permitted for asthma treatment through inhalation. The evaluation of inhaled salbutamol via urinalysis becomes challenging if unauthorized systemic administration has been administered.

Fig. 3. MOA of Beta-Agonist
?-Agonists are effective bronchodilators due primarily to their ability to relax airway smooth muscle (ASM). They exert their effects via their binding to the active site of ?-adrenoceptors on ASM, which triggers a signaling cascade that results in a number of events, all of which contribute to relaxation of ASM.
4. Beta blockers [129, 130, 131]
Beta blockers exert their effects by decreasing heart rate and minimizing muscle tremors, which can enhance performance in precision sports like archery and shooting, where stability and accuracy are critical. However, their influence is detrimental in endurance sports. These medications impair aerobic capacity by reducing cardiac output and limiting the body's ability to increase heart rate during prolonged physical exertion. Consequently, athletes in endurance disciplines may experience a decrease in performance due to the reduced efficiency of oxygen delivery to the muscles.

Fig. 4. MOA of Beta Blockers
Beta-blockers also decrease blood pressure via several mechanisms, including decreased renin and reduced cardiac output. The negative chronotropic and inotropic effects lead to a decreased oxygen demand; that is how angina improves after beta-blocker usage.
5. Stimulants [132, 133, 134]
Stimulants exert both central and peripheral effects on the nervous system, acting to temporarily excite or accelerate physiological activities. These agents enhance alertness, mitigate fatigue, and influence mood and cardiovascular function. Caffeine, a well-known stimulant, effectively counteracts drowsiness, boosts endurance, and improves performance in bodybuilding exercises. According to a recent meta-analysis it is proved that caffeine consumption has significant ergogenic effects, notably increasing maximal muscle strength in the upper body and enhancing muscle power. Methylphenidate, another prominent stimulant, undergoes extensive metabolism, resulting in the production of ritalinic acids. Due to the specific chemical properties of ritalinic acids, they often evade traditional detection methods for stimulant drugs. This metabolic transformation complicates the monitoring and regulation of methylphenidate use in competitive sports, where its performance-enhancing effects can offer an unfair advantage. The pharmacological actions of stimulants like caffeine and methylphenidate are linked to their ability to modulate neurotransmitter systems, particularly those involving dopamine and norepinephrine. By influencing these pathways, stimulants can enhance cognitive function, increase energy levels, and improve physical performance. However, the use of such substances in sports raises ethical and health-related concerns, given their potential for abuse and adverse effects on cardiovascular health.

Fig. 5. MOA of Stimulants
The general mechanism of stimulants revolves around increased catecholamine levels and increased agonistic activity at adrenergic receptors
6. Peptide hormones, growth factors and related substance [135, 136, 137]
Hormones are metabolized rapidly, resulting in a very short half-life, and are excreted in minimal quantities as unchanged compounds in the urine. Growth hormone (GH), or somatotropin, is a polypeptide hormone produced by the anterior pituitary gland. GH functions to increase lean body mass, energy, performance, muscle mass and strength, stroke volume, and maximal oxygen uptake. The abuse of GH in sports is rising due to the challenges in its detection. Monitoring insulin concentrations in blood is crucial for doping control in athletes because exogenous insulin administration can enhance performance. Short-acting insulin is particularly used by bodybuilders, weightlifters, and powerlifters to increase muscle bulk. The International Olympic Committee (IOC) has banned its use except under a Therapeutic Use Exemption (TUE). Erythropoietin (EPO) is a peptide hormone that stimulates red blood cell production by acting on bone marrow. It can increase VO2max by 20%, significantly enhancing the oxygen-carrying capacity of the blood. Recombinant human erythropoietin (epoetin alfa and darbepoetin) is also employed to boost performance in endurance sports such as running, cycling, and skiing, where high oxygen uptake is essential for optimal performance. Human chorionic gonadotropin (hCG) is a glycoprotein hormone secreted by the placenta, playing a crucial role in the development of sexual glands. In the context of sports, hCG is used to stimulate gonadal testosterone synthesis during and after the self-administration of testosterone or anabolic steroids. Its use is prohibited in male athletes. In summary, various hormones, including GH, insulin, EPO, and hCG, are utilized for their performance-enhancing effects in sports. The rapid metabolism and short half-life of these hormones, combined with the sophisticated methods needed for detection, contribute to their abuse. Effective doping control measures and stringent regulations are essential to ensure fair competition and protect athletes' health.

Fig. 6. MOA of Peptide hormones and Growth factors
7. Blood Doping [138, 139, 140]
Blood doping refers to the misuse of certain methods or substances to enhance oxygen delivery to muscles and improve aerobic capacity, thereby gaining a competitive advantage in sports. This practice includes autologous or homologous blood transfusions, the use of erythropoiesis-stimulating agents such as erythropoietin, and the administration of blood substitutes like perfluorocarbons and hemoglobin-based oxygen carriers. Autologous blood transfusion, where an athlete receives their own stored blood, is particularly challenging to detect. Due to its complexity, athletes frequently use this method. Detection often relies on indirect methods, such as measuring total hemoglobin mass or identifying metabolites of blood bag plasticizers, which are by-products of the containers used for blood storage. These indirect measures provide clues about the likelihood of blood doping. The administration of erythropoiesis-stimulating agents like erythropoietin increases red blood cell production, enhancing the blood's oxygen-carrying capacity. This results in improved endurance and performance in aerobic sports. Blood substitutes, such as perfluorocarbons and hemoglobin-based oxygen carriers, function similarly by increasing the amount of oxygen available to muscles. Blood doping remains prevalent in competitive sports due to its availability and the sophisticated techniques required for detection. Effective anti-doping measures and advanced detection methods are crucial for maintaining fair play and athlete health in sports.

Fig. 7. Blood Doping
8. Gene Doping [141, 142, 143]
Gene doping refers to the nontherapeutic use of genes, cells, genetic elements, or modifications in gene expression aimed at enhancing athletic performance. This practice involves the intentional application of gene therapy techniques to boost an athlete's abilities, not for the treatment or prevention of diseases, but solely to improve physical performance. In gene doping, genes are introduced or altered to enhance physiological traits such as muscle growth, endurance, or recovery. These genetic modifications can provide
athletes with significant advantages, such as increased strength, improved aerobic capacity, or faster healing. The ethical and health implications of gene doping are substantial, raising concerns about fair competition and long-term effects on athletes' well-being. As gene doping techniques evolve, detecting these modifications becomes increasingly challenging, necessitating advanced methods and stringent regulations to ensure the integrity of competitive sports.

Fig. 8. Mechanism of Gene Doping
9. Amphetamines and their derivatives [144, 145, 146]
Several compounds are metabolized into amphetamines in the human body. The presence of amphetamine in urine can indicate the ingestion of amphetamine itself or one of its precursor compounds. Stimulant drugs such as cocaine, amphetamines, and hallucinogens can alter mental alertness. Centrally, these substances enhance alertness and can provide motivational and attitudinal advantages. Peripherally, they increase cardiac output and blood flow to muscles, potentially improving performance, especially during the initial stages of exercise. In urine, unchanged cocaine is typically not present. Instead, its primary metabolic products, benzoylecgonine and ecgonine methyl ester, are detected. These metabolites are indicative of cocaine use and are commonly screened in doping tests to identify the consumption of this performance-altering substance.

Fig. 9. MOA of Amphetamines
Amphetamine increases the amounts of monoamine neurotransmitters in the cytosol through the inhibition of vesicular monoamine transporter 2 (VMAT2) as well as through disruption of the electrochemical gradients necessary for vesicular transporter function
10. Narcotic Analgesics [147, 148, 149]
Narcotic analgesics are commonly employed for pain management, acting on specific receptors within the neural axis to modulate pain signals. By predominantly depressing the nervous system, they alleviate fear, anxiety, and pain sensations, enabling athletes to surpass their usual pain thresholds. However, the misuse of these substances, driven by competitive pressures, often leads to numerous musculoskeletal injuries among athletes. Buprenorphine, characterized by its low therapeutic dosage and extended elimination period, yields minimal urinary concentrations and is typically detectable solely through immunoanalytical methods. Consequently, confirming its presence via mass spectrometry poses challenges. While codeine is permitted for its antitussive properties, it undergoes partial conversion to morphine within 24 hours of administration, rendering it a prohibited substance. Similarly, dextromethorphan, an antitussive agent, metabolically transforms into dextrorphan, the d-isomer of l-levorphanol, a banned narcotic. This metabolic conversion complicates the differentiation between licit and illicit usage, presenting diagnostic challenges.

Fig. 10. MOA of Narcotic Analgesics
11. Diuretics [150, 151, 152]
Diuretics are frequently employed to achieve rapid weight loss, serving two primary purposes: to compete in lower weight categories and to act as a "masking agent" by reducing the concentration of other banned substances in urine, thereby accelerating the elimination of performance-enhancing drugs (PEDs). Athletes often misuse diuretics in conjunction with anabolic steroids to counteract the fluid retention induced by the steroids. However, the adverse effects of diuretics, including electrolyte imbalances, muscle cramps, dehydration, and volume depletion, can lead to severe consequences, including death. Detection methods for diuretics are highly sensitive, enabling the identification of even trace amounts in urine samples.
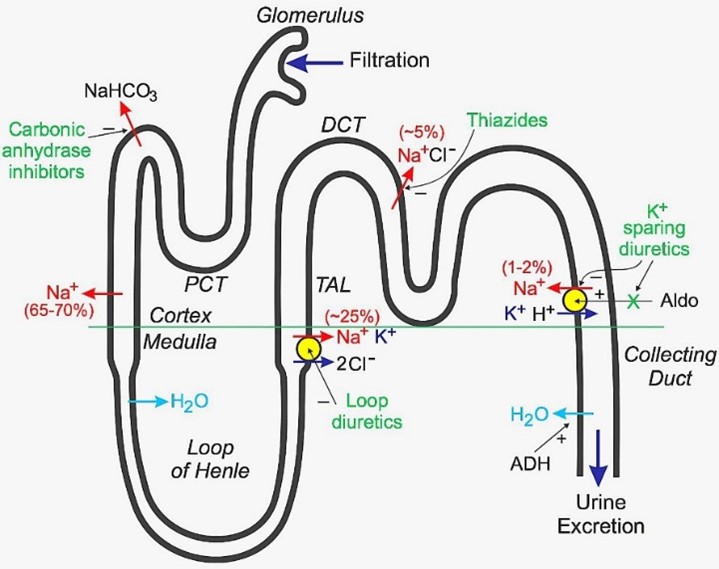
Fig. 11. MOA of Diuretics
Diminishing sodium reabsorption at different sites in the nephron, thereby increasing urinary sodium and water losses.
12. Beta-hydroxy-beta-methylbutyrate [153, 154, 155]
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the amino acid leucine and serves as a precursor to cholesterol. It has garnered increased interest among athletes due to its role in regulating protein metabolism post-exercise. HMB has been found to potentially mitigate muscle protein breakdown and aid in muscle recovery following intense physical activity. As a result, athletes are exploring its potential benefits for improving performance and enhancing muscle growth. activity. As a result, athletes are exploring its potential benefits for improving performance and enhancing muscle growth.

Fig. 12. MOA of HMB
It stimulates myofibrillar muscle protein synthesis and inhibiting muscle protein breakdown through various mechanisms, including the activation of mechanistic target of rapamycin complex 1 (mTORC1) and inhibition of proteasome-mediated proteolysis enzyme.
13. Alcohol [156, 157, 158]
The use of alcohol during competition is forbidden. The doping violation threshold for alcohol, based on hematological values, is set at 0.10 g/L. While alcohol can alleviate nervousness, anxiety, and hand tremors—beneficial in precision sports like archery and shooting—it detrimentally impacts reaction time, resulting in limb instability and sedation effects. This poses significant risks in sports such as vehicle racing. In 2018, alcohol was removed from the prohibited list, having been previously banned in four sports. National Anti-Doping Organizations are no longer obligated to test for alcohol but may provide assistance to governing bodies as deemed necessary.

Fig. 13. MOA of Alcohol
Alcohol enhancing the effect of GABA, an inhibitory neurotransmitter, on its receptors. It also inhibits the actions of 'glutamate' on the NMDA receptors, resulting in an incautious and dull state of mind.
14. Significant modifications in the World Anti-Doping Agency's (WADA) 2018 catalog of banned substances [159, 160, 161, 162]
Alcohol and cannabidiol have been eliminated from the prohibited list, except for cannabidiol products containing Tetrahydrocannabinol (THC). Bemitil, a synthetic actoprotector, has been added to the WADA monitoring program for both in-competition and out-of-competition use. Hydrocodone will be monitored specifically during in-competition periods. Additionally, Mitragynine and telmisartan have been removed from the monitoring list.
Advancements in Doping Testing
Sample collection for doping testing occurs through two methods: "in-competition" testing, conducted during events, and "out-of-competition" (OOC) testing, which occurs at squad sessions, homes, or training venues. Athletes are randomly selected for testing, with an automated draw used for OOC selections. Testing is conducted exclusively at WADA-accredited laboratories [163, 164]. During the procedure, athletes provide identification and two samples under direct supervision. Sample A undergoes analysis for banned substances or methods, while sample B is reserved for confirmation if sample A yields a positive result and the athlete requests further analysis. The emergence of personalized biomarker monitoring has led to the development of the "Athlete Biological Passport" [165, 166]. This passport tracks changes in the athlete's hematological, steroidal, and endocrine profiles. Deviations from the established normal ranges in these biomarkers may indicate doping or a medical condition. Similar to how healthcare professionals utilize disease-related biomarkers for diagnosis, selected biomarkers can be leveraged to detect doping practices in athletes [167, 168].
Challenges in Doping Detection: Collection and Analysis of Athlete Biological Specimens
With an extensive array of drugs listed in the World Anti-Doping Agency's (WADA) "prohibited list," the task of gathering biological specimens from athletes for the detection of performance-enhancing drugs (PEDs) is formidable [169, 170]. Samples such as urine or blood must be collected from athletes, involving the procurement and processing of multiple samples. Some samples are promptly analyzed, while others are stored for potential confirmatory analysis at a later time if necessary. These bio-specimens undergo intricate and precise biochemical analysis procedures to detect banned PEDs. Furthermore, it is impractical to collect samples from every athlete participating in sporting events worldwide [171, 172, 173]. Athletes employ various strategies to evade detection for doping. Some resort to using devices that mimic urine samples, containing maneuvered clean urine stored within a balloon inserted into the anus before competition. The catheter remains imperceptible below the perineum, allowing the athlete to expel the fake urine sample during doping control by contracting the gluteus and elevator muscles of the anus, potentially yielding false-negative results [174, 175]. Masking agents are also utilized to accelerate PED elimination or obscure detection in samples. Another tactic involves strategically timing PED use during training periods to enhance exercise intensity and subsequently improve endurance and muscular strength. While discontinuing PED use before competitions diminishes benefits, residual effects may provide a slight advantage. Additionally, some athletes actively seek novel, WADA-unlisted PEDs to evade detection until scientific investigations mandate their prohibition. The pharmaceutical industry continuously develops drugs, which, although intended for legitimate medical purposes, may inadvertently enhance athletic performance due to biochemical or biological effects. Athletes may exploit these advancements to gain an edge, sometimes outpacing regulatory measures [176, 177].
Spectrum of Sports Injuries
The majority of sports injuries stem from either repetitive strain on muscles or joints or direct physical trauma. These injuries commonly involve minor damage to bones, muscles, joints, ligaments, or tendons, such as contusions, sprains, and strains. Strains or sprains of the ankle joint are particularly prevalent. Notable sports-related injuries encompass conditions like tennis elbow (lateral epicondylitis), golfer's or baseball elbow (medial epicondylitis), lumbar strain (trauma to the lower back resulting in injured tendons and muscles causing spasm), jumper's knee (patellar tendonitis), runner's knee (patella-femoral stress syndrome), fractures, stress fractures, and dislocations. Tennis elbow gained international attention when renowned Indian cricketer Sachin Tendulkar experienced it [178, 179].
Comprehensive Injury Rehabilitation: Strategies and Considerations for Athletes
The type and severity of an injury dictate the comprehensive recovery program tailored to the individual needs of athletes. An integrated approach involving active participation from the injured athlete and their family is crucial for the success of the recovery process. In cases of amputation, the primary goals are to achieve the highest level of function and regain independent movement while enhancing overall quality of life [180]. Recovery programs designed to meet these objectives typically encompass various components, including tailored exercise regimens to stretch and strengthen the affected area, movement restrictions, physical or occupational therapy, and conditioning exercises aimed at preventing further injury. Additionally, interventions such as hot or cold therapy, Jacuzzi treatments, and the application of braces, splints, or casts may be utilized to immobilize the area, along with the use of assistive devices like crutches or wheelchairs when necessary [181, 182]. Pain management techniques and education for both the patient and their family are integral aspects of the rehabilitation process. In managing pain, caution is warranted when administering medications to athletes. While nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used to alleviate inflammation, their impact on muscle healing remains controversial, potentially impairing muscle pliability and force production. However, NSAIDs have demonstrated no adverse effects on ligament healing and may even enhance early ligament strength when administered within the first six days. Although animal studies have suggested NSAIDs may delay fracture healing, no conclusive evidence exists in humans. Fracture healing involves the differentiation of mesenchymal cells into osteoblasts and chondrocyte progenitors, with the cyclooxygenase pathway playing a pivotal role in osteogenesis and chondrogenesis. Inflammation modulators offer an alternative to NSAIDs, regulating the inflammatory process by inhibiting pro-inflammatory cytokines and stimulating anti-inflammatory cytokines. Examples include Traumeel, a marketed inflammation modulator containing a fixed combination of biological and mineral extracts, as well as topical glyceryl trinitrate, aprotinin injections, botulinum toxin, and prolotherapy for soft tissue injuries [183, 184, 185]. Prolotherapy involves injecting a sclerosant such as hypertonic glucose or phenol at the injury site to promote healing. Aprotinin, a small protein bovine pancreatic trypsin inhibitor, acts as an antifibrinolytic molecule and is used in treating soft tissue injuries. Metalloprotease inhibitors, which inhibit matrix metalloproteinases, are also emerging as promising options for soft tissue injury treatment [186, 187, 188]. To address such complex medical scenarios, pharmacy services were established at the London 2012 Olympic and Paralympic Games, representing some of the most advanced and comprehensive pharmaceutical services offered at any Olympic or Paralympic event [189, 190].
Advancing Athlete Health: The Role of Sports Pharmacology and Pharmacy in India
Sports pharmacology is integral to athletics, encompassing the study of medicines tailored to the needs of athletes. It involves regular health assessments, managing medical histories, and treating sports-related injuries [191, 192]. Athletes can mitigate illness, injury, and doping incidents through a foundational understanding of sports science, exercise physiology, and the pharmacokinetics and pharmacodynamics of biologically active substances present in food or medications [193, 194]. Medical education in India is primarily generalist, providing broad knowledge across preclinical, paraclinical, and clinical medicine [195, 196]. Specialization typically occurs at the postgraduate level, with pharmacology courses often lacking sufficient emphasis on sports pharmacology. Given the growing intersection of medicine and sports, specialized training in sports medicine for pharmacologists is imperative. Furthermore, pharmacists can leverage their expertise in drug selection and dosing to address athletes' unique treatment and preventive care needs, constituting sports pharmacy. These professionals serve as valuable resources for athletes, offering guidance on dietary supplements and prescriptions. Collaboratively, sports pharmacologists and pharmacists can establish a community dedicated to promoting doping-free sports in India [197, 198].
Advancing Athlete Health and Performance: The Role of Sports Pharmacology and Interprofessional Collaboration
The physiological effects induced by both drugs and exercises can significantly impact the performance and well-being of athletes. For instance, over-the-counter medications commonly used for treating conditions like the common cold may contain substances that elevate heart rate, induce nervousness, and elicit other reactions, potentially compromising athletic performance and safety, especially during exercise. Additionally, athletes must exercise caution with nutritional supplements, as some may inadvertently contain substances prohibited by anti-doping regulations. Understanding the pharmacological properties of drugs is crucial for athletes, as the extent of their effects depends on factors such as administration route, frequency, duration, and dosage form. Alternative therapies, including Ayurveda, may also influence athletic performance [199, 200]. The increasing use of herbal medicines and supplements, particularly in India, introduces various polyphenols, terpenoids, and alkaloids that can induce beneficial physiological changes in athletes, such as endurance enhancement with substances like Ginseng [201]. Healthcare professionals prescribing medications to athletes must exercise heightened vigilance, as certain drugs are banned by sporting organizations like the IOC and NCAA. Athletes who test positive for prohibited substances risk disqualification, suspension, or lifetime bans [202, 203]. Hence, athletes must be aware of the drugs they consume, their effects, and prescribed limits. Incorporating sports pharmacology into medical education can better equip healthcare professionals to navigate the complexities of prescribing medications to athletes. This specialized field also intersects with forensic pharmacology and plays a pivotal role in safeguarding the integrity of sports competitions. Expanding research in sports pharmacology, especially within the Indian context, is essential. Structured and accredited courses in sports sciences, including sports pharmacology, offered by recognized institutions can further enhance healthcare professionals' understanding and management of medication use in athletes. Inter professional collaboration among healthcare providers, including sports pharmacologists and pharmacists, is vital for educating athletes about the risks of inadvertent doping and optimizing health outcomes. Training in teamwork within the context of sports can facilitate effective collaboration among healthcare professionals, leading to improved strategies and outcomes in athlete care [204, 205, 206].
CONCLUSION:
The pervasive use of performance-enhancing substances (PESs) and doping practices in competitive sports underscores the need for a multifaceted approach to safeguard the integrity of athletic competitions and prioritize athlete health. The comprehensive classifications outlined by the World Anti-Doping Agency (WADA) serve as a foundation for identifying and regulating prohibited substances and methods. However, the constant evolution of PESs and doping techniques poses ongoing challenges for detection and enforcement. Advancements in analytical techniques, such as the Athlete Biological Passport and biomarker monitoring, have shown promise in enhancing doping detection capabilities. Nevertheless, athletes continue to exploit novel substances and sophisticated masking strategies, necessitating continuous vigilance and the development of cutting-edge detection methodologies. The physiological impacts of exercise on drug pharmacokinetics and pharmacodynamics underscore the importance of tailoring medication regimens to the unique needs of athletes. Comprehensive injury rehabilitation programs, integrating judicious pain management strategies and non-pharmacological interventions, are crucial for optimizing recovery and mitigating the risk of further harm. The emerging field of sports pharmacology plays a pivotal role in promoting athlete health, preventing inadvertent doping, and fostering fair competition. Integrating sports pharmacology into medical curricula and establishing structured training programs can equip healthcare professionals with the necessary knowledge and skills to navigate the complexities of medication use in athletes effectively. Interprofessional collaboration among sports pharmacologists, pharmacists, and other healthcare providers is paramount to ensuring holistic athlete care. Such collaborative efforts can facilitate the dissemination of knowledge, promote ethical decision-making, and contribute to the development of evidence-based guidelines for medication use in athletic settings. Ultimately, a concerted effort involving regulatory bodies, sporting organizations, healthcare professionals, and athletes themselves is crucial to upholding the principles of fair play and maintaining the integrity of competitive sports while prioritizing the health and well-being of athletes.
REFERENCES














K. Rajeswar Dutt1, Mahesh Kumar Yadav 2, Asfaque Ali 3 , Laxman Kumar Mahto3, Aman Sahu3, Saurav Kumar3, Sushil kumar Mandal3, Aditya kumar3, Alok Kumar3, Anuradha Kumari 3, Ayush Kumar Verma 3, Mayank Prasad 3,Arnab Roy4, The Intricate Landscape Of Performance-Enhancing Drugs And Doping In Sports: Implications For Athlete Health And Fair Competition, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 7, 387-392. https://doi.org/10.5281/zenodo.12738005
 10.5281/zenodo.12738005
10.5281/zenodo.12738005
