1,3 Faculty of Pharmaceutical Sciences, PCTE Group of Institutes, Ferozepur Road, Near Baddowal Cantt, Jhandey, Ludhiana
2 Doctorate of Pharmacy, ISF College of Pharmacy, Ghal Kalan, Moga, Punjab, India
Hepatocellular carcinoma (HCC) is the most common and aggressive form of liver cancer, representing a significant global health burden. It is one of the leading causes of cancer-related mortality worldwide, with its incidence rising across diverse populations and geographical regions. The highest prevalence is observed in regions with endemic chronic Hepatitis B (HBV) and Hepatitis C (HCV) infections, such as Asia and sub-Saharan Africa. In developed countries, the growing prevalence of alcohol-related liver disease and non-alcoholic fatty liver disease (NAFLD) is contributing to an increasing number of HCC cases. Chronic liver injury, driven by factors such as viral infections, alcohol consumption, and metabolic disorders, is a major risk factor for HCC, often leading to cirrhosis, a key precursor to liver cancer. The progression from cirrhosis to HCC is driven by complex molecular mechanisms involving genetic mutations, epigenetic alterations, inflammation, and fibrosis, which together create a microenvironment conducive to tumorigenesis. Despite improvements in early detection and therapeutic strategies, the treatment options for advanced HCC remain limited, with surgical resection, liver transplantation, and systemic therapies offering modest survival benefits. This highlights the urgent need for more effective and targeted therapies that can address the underlying molecular pathways driving HCC progression. Understanding the intricate molecular pathophysiology of HCC is essential for developing novel therapeutic approaches that can significantly improve patient outcomes.
One of the most prevalent and deadly cancers in the world is hepatic cancer, primarily hepatocellular carcinoma (HCC). Due to late-stage diagnosis and few available treatment choices, it causes a large percentage of cancer-related deaths with a poor prognosis. A better understanding of HCC's development and treatment approaches is necessary due to its high morbidity and mortality rates [1]. One of the main causes of HCC is a chronic infection with the hepatitis B or hepatitis C viruses, which results in chronic liver inflammation. Additional significant risk factors include exposure to environmental pollutants including aflatoxins, metabolic diseases like diabetes and obesity, excessive alcohol use, and non-alcoholic fatty liver disease (NAFLD).[2]
Hepatocytes give rise to HCC, which frequently occurs against a backdrop of cirrhosis and chronic liver disease, as shown in Figure 1. As shown in Figure 2, the pathophysiology of HCC includes a number of genetic and epigenetic changes that result in unchecked cellular growth, angiogenesis, and immune evasion. The formation of HCC is linked to molecular mechanisms that aid in tumor initiation and progression, such as the β-catenin, PI3K/Akt/mTOR, and JAK/STAT signaling pathways. Since HCC frequently exhibits no symptoms in its early stages, early detection is difficult, which worsens the prognosis[3].
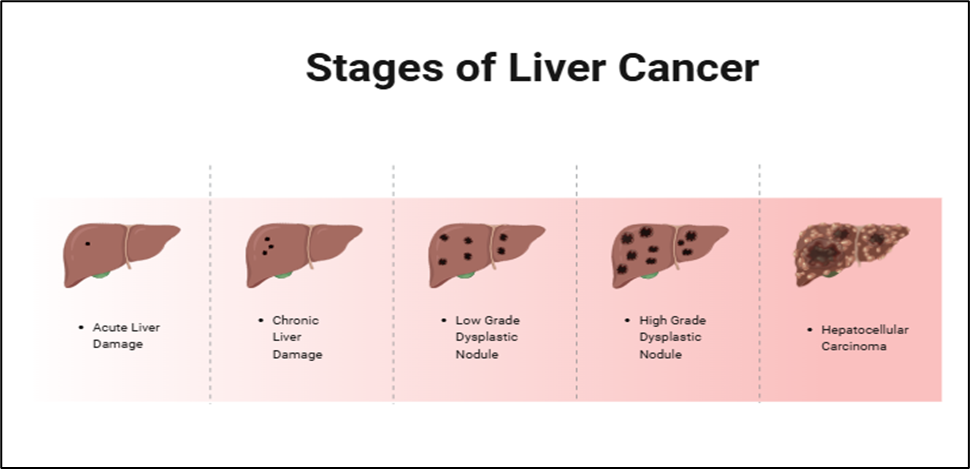
Figure 1. Represents the different stages of Liver Cancer
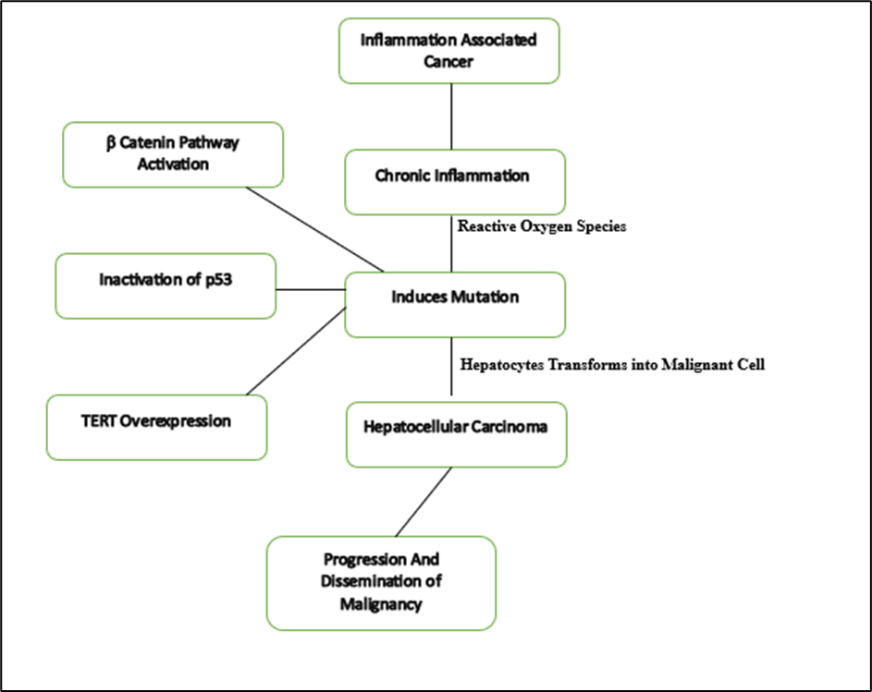
Figure 2. Represents the pathway involved in HCC.
Depending on the liver function and disease stage, HCC can be treated in multiple ways. For early-stage HCC liver transplantation and surgical resection continue to be the most successful curative therapies [4]. However, due to stringent eligibility requirements and restricted donor availability these therapies are ineffective only for a tiny percentage of patients (Torre et al., 2015). For intermediate-stage HCC, localized therapies including radiofrequency ablation (RFA) and Trans arterial chemoembolization (TACE) are utilized. They provide palliative advantages but have limited long term effectiveness (Chen & Bai Although systemic treatments such as immune checkpoint inhibitors (nivolumab, pembrolizumab) and tyrosine kinase inhibitors (soravifenib lenvatinib) have demonstrated promise for advanced HCC treatment resistance and adverse effects remain major obstacles.
Induced pluripotent stem cells (iPSCs) have emerged as a transformative technology in regenerative medicine, with significant implications for hepatic cancer therapy as represented in Figure 3. (Takahashi & Yamanaka, 2006). iPSCs are generated by reprogramming adult somatic cells into a pluripotent state, allowing them to differentiate into various cell types, including hepatocytes. This ability makes iPSCs a promising tool for disease modeling, drug discovery, and regenerative therapies (Wu & Shi, 2017). One of the key applications of iPSCs in HCC treatment is their use in patient-specific disease modeling. By generating HCC-specific iPSC lines, researchers can study tumor progression, identify novel biomarkers, and test new therapeutic agents in a personalized manner (Takahashi & Yamanaka, 2006).
Additionally, iPSC-derived hepatocytes hold potential for liver regeneration and transplantation, offering a renewable source of functional liver cells that could alleviate the shortage of donor organs (Wu & Shi, 2017). Furthermore, iPSCs have the potential to enhance immune-based therapies for HCC. By differentiating iPSCs into immune cells such as natural killer (NK) cells and T cells, researchers can develop targeted immunotherapies to combat HCC (Rasi et al., 2015). The combination of iPSC technology with gene-editing tools such as CRISPR-Cas9 further expands the therapeutic possibilities, allowing for the correction of genetic mutations associated with liver cancer (Gish & Liu, 2017).
Despite these promising applications, several challenges must be addressed before iPSC-based therapies can be widely implemented. The risk of tumorigenicity, ethical considerations regarding genetic modifications, and the need for efficient differentiation protocols are significant hurdles that require further investigation (Llovet et al., 2016). Nonetheless, ongoing research and technological advancements continue to enhance the feasibility of iPSC-based therapies for hepatic cancer (Wu & Shi, 2017). By addressing these challenges and exploring innovative approaches, iPSCs may play a crucial role in the future of hepatic cancer treatment (Chen & Bai, 2019).
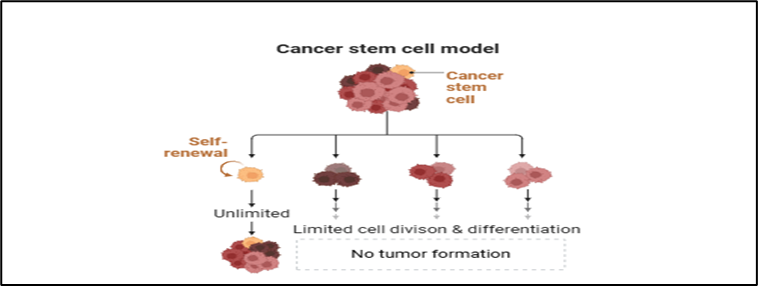
Fig.3. Represents the principle of stem cell therapy
Mechanisms of iPSC Therapy in Hepatic Cancer
By such mechanisms as liver regeneration, disease modeling, gene therapy, and immunotherapy, induced pluripotent stem cells (iPSCs) provide an integrated approach to the treatment of hepatic cancer. As an alternative to transplantation, iPSCs allow patients with hepatocellular carcinoma (HCC) and chronic liver disease to restore liver function through the generation of hepatocyte-like cells (HLCs). Patient-derived iPSCs also provide physiologically relevant models for the investigation of tumor biology, allowing precision medicine approaches and personalized drug screening for the identification of effective therapies (Wu, J., & Shi, Y. (2017). Gene therapy applications of iPSC technology, allowing targeted therapies for hepatic cancer, include silencing oncogenes, correcting tumor suppressor mutations, and delivering therapeutic genes by CRISPR-Cas9 editing. Moreover, by boosting anti-tumor immunity against liver cancer antigens including glypican-3 (GPC3) and alpha-fetoprotein (AFP), iPSC-derived immune cells, such as CAR-T and natural killer (NK) cells, offer promising immunotherapeutic approaches. By producing these immune cells on a large scale as "off-the-shelf" treatments, the drawbacks of conventional autologous cell therapies are removed, increasing scalability and accessibility. Despite drawbacks like as immune evasion, tumorigenicity hazards, and inefficient differentiation, developments in bioengineering, gene editing, and immune modulation continue to improve iPSC-based therapies. With further development, iPSCs could revolutionize hepatic cancer treatment by combining advanced immunotherapy, customized treatments, and regenerative medicine into a successful and comprehensive approach.
Applications of iPSCs in Hepatic Cancer Research
Induced pluripotent stem cells (iPSCs) have transformed the landscape of hepatic cancer research, offering innovative applications in disease modeling, drug discovery, regenerative medicine, gene therapy, and immunotherapy. As a versatile and patient-specific cell source, iPSCs provide unprecedented opportunities to study hepatocellular carcinoma (HCC) and other liver malignancies while also paving the way for personalized therapeutic strategies. One of the most significant applications of iPSCs in hepatic cancer research is their use in disease modeling, which allows scientists to replicate the complex genetic and molecular characteristics of liver cancer in a controlled laboratory setting. (Ang, L. T., Tan, A. K (2021) By reprogramming somatic cells from HCC patients into iPSCs and differentiating them into hepatocytes or hepatic tumor cells, researchers can develop patient-specific cancer models that closely mimic the heterogeneity of liver tumors. These models help in understanding the molecular mechanisms driving HCC progression, including genetic mutations, epigenetic modifications, and interactions within the tumor microenvironment. Traditional cancer cell lines and animal models often fail to fully recapitulate the complexity of human liver cancer, making iPSC-based models a more accurate and physiologically relevant alternative. Furthermore, iPSCs enable the creation of 3D liver organoids that better simulate the tumor microenvironment, providing a more dynamic platform for studying tumor-stroma interactions and therapeutic responses.
Another critical application of iPSCs in hepatic cancer research is their role in drug screening and personalized medicine. Conventional drug testing methods rely on immortalized cancer cell lines and animal models, which often do not accurately predict patient responses due to species differences and the lack of genetic variability in established cell lines. iPSC-derived liver cancer models overcome these limitations by offering patient-specific platforms for high-throughput drug screening, enabling the identification of novel therapeutic compounds with greater precision. By generating iPSCs from diverse patient populations and differentiating them into hepatic tumor cells, researchers can test the efficacy and toxicity of anticancer drugs in a genetically diverse setting, leading to more effective and personalized treatment strategies. This approach also facilitates the identification of biomarkers associated with drug sensitivity or resistance, allowing clinicians to tailor therapies to individual patients based on their genetic profiles. Additionally, iPSC-derived hepatocytes serve as valuable tools for evaluating drug-induced hepatotoxicity, which remains a major concern in cancer treatment. Many chemotherapy agents and targeted therapies cause liver damage, necessitating reliable models to assess their hepatic safety profiles. The use of iPSC-derived hepatocytes in toxicity screening helps mitigate adverse effects and optimize drug formulations for safer clinical applications.
In the field of regenerative medicine, iPSCs offer promising avenues for liver tissue engineering and transplantation in hepatic cancer patients with liver failure. Liver transplantation remains the most effective curative option for HCC patients with cirrhosis or end-stage liver disease; however, the severe shortage of donor organs and the risk of immune rejection pose significant challenges. iPSC technology provides a potential solution by enabling the generation of patient-specific hepatocytes or liver tissue constructs for transplantation, eliminating the need for donor organs and reducing the likelihood of immune rejection. (Nishimura, T., Kaneko (2022). Differentiation protocols have been developed to generate functional hepatocyte-like cells (HLCs) from iPSCs, capable of performing essential liver functions such as detoxification, albumin secretion, and bile acid production. While challenges remain in achieving fully mature hepatocytes that can function equivalently to primary liver cells, advances in bioengineering approaches, such as 3D bioprinting and organoid technology, are helping to improve the structural and functional integration of iPSC-derived liver tissues. The transplantation of iPSC-derived hepatocytes into liver cancer patients may not only support liver regeneration but also create a more favorable hepatic microenvironment, potentially suppressing tumor growth and enhancing the efficacy of other cancer therapies.
In addition to regenerative applications, iPSCs are being explored as platforms for gene therapy in hepatic cancer. HCC is driven by various genetic mutations and dysregulated signaling pathways, making gene-targeted interventions a promising therapeutic approach. iPSCs can be genetically modified using advanced gene-editing tools such as CRISPR-Cas9 to correct tumor suppressor gene mutations, silence oncogenes, or introduce therapeutic genes that enhance anti-tumor immunity. For example, iPSC-derived hepatocytes can be engineered to restore functional TP53 expression, a critical tumor suppressor frequently mutated in HCC, thereby inhibiting cancer progression. Additionally, iPSCs offer a powerful system for studying the role of specific genes in liver cancer development, allowing researchers to manipulate gene expression in iPSC-derived liver cells and analyze their effects on tumor growth, invasion, and metastasis. This genetic engineering capability extends to iPSC-derived immune cells, which can be modified to enhance their anti-tumor activity and improve the effectiveness of immunotherapies.
One of the most exciting applications of iPSCs in hepatic cancer research is their use in immunotherapy, particularly in the development of chimeric antigen receptor (CAR) T-cell and natural killer (NK) cell therapies. Traditional CAR-T cell therapy, which involves engineering a patient’s T-cells to recognize and attack cancer cells, has shown remarkable success in blood cancers but faces challenges in solid tumors like HCC due to the immunosuppressive tumor microenvironment and limited T-cell persistence. iPSC-derived CAR-T cells offer a novel solution by providing a renewable and standardized source of T-cells that can be mass-produced and engineered for enhanced tumor-targeting capabilities. Unlike conventional CAR-T therapies that rely on patient-derived T-cells, iPSC-derived CAR-T cells can be generated from a single iPSC line, allowing for off-the-shelf availability and greater scalability. These cells can be designed to target liver cancer-specific antigens such as glypican-3 (GPC3), alpha-fetoprotein (AFP), or epithelial cell adhesion molecule (EpCAM), improving the precision and efficacy of treatment. Moreover, iPSC-derived CAR-T cells can be genetically modified to resist immune suppression and increase their persistence in the hostile tumor microenvironment, addressing one of the key limitations of CAR-T therapy in solid tumors.
Beyond CAR-T cells, iPSCs are also being utilized to generate NK cells for liver cancer immunotherapy. NK cells play a crucial role in anti-tumor immunity by recognizing and eliminating cancer cells without prior antigen sensitization. iPSC-derived NK cells offer a promising alternative to conventional NK cell therapies, as they can be produced in large quantities and genetically optimized for enhanced tumor-targeting ability. (Hendriks, D. F. G., Miyaoka, Y., & Andersson, T. B. (2022). These cells can be engineered to express high-affinity receptors for liver cancer antigens, increasing their cytotoxic activity against HCC cells. Additionally, iPSC-derived NK cells can be combined with immune checkpoint inhibitors to overcome tumor-induced immune evasion and improve overall treatment efficacy. The ability to generate standardized, genetically enhanced NK cells from iPSCs holds immense potential for advancing adoptive cell therapy in hepatic cancer.
Despite these promising applications, several challenges must be addressed to fully realize the potential of iPSC-based therapies in hepatic cancer research. One of the primary concerns is the risk of tumorigenicity, as iPSCs have the potential to form teratomas if residual undifferentiated cells persist in the final cell product. Ensuring the complete differentiation of iPSCs into target cell types and implementing rigorous quality control measures are critical for minimizing this risk. Additionally, the scalability and cost-effectiveness of iPSC-derived therapies remain significant hurdles, as current protocols for iPSC generation, differentiation, and expansion require extensive time and resources. Advances in automation, bioreactor-based production, and synthetic biology approaches may help overcome these limitations and facilitate the widespread adoption of iPSC-based applications in hepatic cancer research.
Advances in iPSC Technology and Hepatic Cancer Therapy
Induced pluripotent stem cell (iPSC) technology has undergone significant advancements in recent years, positioning itself as a transformative tool in hepatic cancer therapy. As researchers continue to refine reprogramming techniques, differentiation protocols, gene-editing strategies, and immunotherapy applications, iPSCs are increasingly recognized for their potential to address critical challenges in liver cancer treatment. Hepatocellular carcinoma (HCC), the most common form of liver cancer, remains a leading cause of cancer-related mortality worldwide due to its late-stage diagnosis, high recurrence rate, and limited therapeutic options. Traditional treatments, including surgery, chemotherapy, targeted therapy, and immunotherapy, have shown variable success, but many patients continue to face poor prognoses. The emergence of iPSC technology offers a paradigm shift by enabling personalized medicine, regenerative approaches, and novel immunotherapies tailored to the complexities of hepatic cancer. Recent advances in iPSC generation have significantly improved efficiency and safety, reducing the risks associated with genomic instability and tumorigenicity. Early iPSC reprogramming methods relied on integrating viral vectors, which posed concerns regarding insertional mutagenesis and oncogene activation. However, the development of non-integrative reprogramming techniques, such as episomal vectors, Sendai virus, synthetic mRNA, and small molecules, has enhanced the safety profile of iPSCs, making them more suitable for clinical applications. Additionally, the discovery of optimized transcription factor combinations and culture conditions has increased the efficiency and reproducibility of iPSC generation, allowing for more consistent production of patient-specific cells for therapeutic use. Another significant advancement in iPSC technology is the development of robust differentiation protocols that enable the generation of functional hepatocyte-like cells (HLCs). Early attempts to derive hepatocytes from iPSCs faced challenges due to incomplete maturation and limited functionality. However, recent breakthroughs in three-dimensional (3D) culture systems, organoid models, and biomaterial scaffolds have improved the structural and functional properties of iPSC-derived hepatocytes. These advancements have enabled the development of liver tissue constructs that closely mimic native liver architecture and physiology, enhancing their potential for transplantation and disease modeling in hepatic cancer research. Furthermore, co-culture systems that integrate iPSC-derived hepatocytes with other liver cell types, such as hepatic stellate cells, Kupffer cells, and endothelial cells, have facilitated the creation of more physiologically relevant liver models for studying tumor-stroma interactions and drug responses in HCC. (Hendriks, Andersson, T. B. (2022). Gene-editing technologies, particularly CRISPR-Cas9, have revolutionized iPSC-based approaches to hepatic cancer therapy by enabling precise genetic modifications. By correcting mutations in tumor suppressor genes, such as TP53 and PTEN, or silencing oncogenes like MYC and TERT, researchers can generate genetically enhanced hepatocytes with improved tumor-suppressing properties. Additionally, iPSCs provide a valuable platform for modeling HCC-associated genetic alterations, allowing for the identification of novel therapeutic targets and the development of gene-based interventions. Beyond hepatocyte-based applications, iPSC-derived immune cells have emerged as a promising avenue for advancing immunotherapy in hepatic cancer treatment. The generation of chimeric antigen receptor (CAR)-T cells from iPSCs has opened new possibilities for overcoming the challenges associated with conventional CAR-T cell therapy in solid tumors. Traditional CAR-T therapies require autologous T-cell harvesting, which is time-consuming and often impractical for HCC patients with compromised immune function. In contrast, iPSC-derived CAR-T cells can be mass-produced from a single engineered iPSC line, providing an off-the-shelf immunotherapy option with standardized potency and reduced variability. Additionally, iPSC-derived CAR-T cells can be genetically modified to enhance their persistence, trafficking, and resistance to the immunosuppressive tumor microenvironment, thereby improving their efficacy against liver cancer antigens such as glypican-3 (GPC3) and alpha-fetoprotein (AFP). Another breakthrough in iPSC-based immunotherapy involves the generation of natural killer (NK) cells for hepatic cancer treatment. Unlike T cells, NK cells do not require antigen priming and can directly target liver cancer cells through innate immune mechanisms. iPSC-derived NK cells have shown significant promise in preclinical studies, demonstrating potent anti-tumor activity and the ability to overcome immune evasion strategies employed by HCC cells. Moreover, genetic engineering approaches have enabled the enhancement of iPSC-derived NK cells with improved tumor-targeting capabilities, including the expression of high-affinity receptors and resistance to immune checkpoint inhibitors. The combination of iPSC-derived NK cells with existing immunotherapies, such as checkpoint blockade inhibitors and cytokine therapies, is an area of active research aimed at further improving treatment outcomes for HCC patients. The integration of iPSC technology with advanced bioengineering techniques has also led to the development of innovative delivery systems for hepatic cancer therapy. One such approach involves the use of iPSC-derived extracellular vesicles (EVs), which can serve as natural carriers for therapeutic molecules. These EVs can be engineered to deliver small interfering RNA (siRNA), microRNA (miRNA), or chemotherapeutic agents directly to liver cancer cells, enhancing drug delivery specificity while minimizing systemic toxicity. Additionally, iPSC-derived EVs have been shown to possess immunomodulatory properties, making them a potential tool for modulating the tumor microenvironment in HCC. (Nishimura, T., Kaneko, S., (2022) Another exciting development in iPSC-based hepatic cancer therapy is the use of organ-on-a-chip technology, which allows researchers to create microfluidic liver models for studying cancer progression and drug responses in a highly controlled environment. These microphysiological systems integrate iPSC-derived hepatocytes, immune cells, and endothelial cells to replicate the complex interactions that occur within the liver, providing a powerful platform for screening new therapies and investigating mechanisms of resistance in HCC. Despite these remarkable advancements, several challenges must be addressed before iPSC-based therapies can be widely implemented in clinical settings for hepatic cancer treatment. One of the primary concerns is the potential for tumorigenicity associated with residual undifferentiated iPSCs. Rigorous quality control measures, including advanced cell sorting techniques and genetic screening, are necessary to minimize the risk of teratoma formation. Additionally, the scalability and cost-effectiveness of iPSC-derived therapies remain significant hurdles, as current manufacturing processes require extensive time, resources, and regulatory approvals. Efforts to automate iPSC production, optimize differentiation protocols, and develop cost-effective bioreactor systems are underway to overcome these limitations. Another key challenge in iPSC-based hepatic cancer therapy is the issue of immune compatibility. While autologous iPSC-derived therapies eliminate the risk of immune rejection, they require individualized cell production, which is time-intensive and costly. Alternatively, the development of universal donor iPSC lines with reduced immunogenicity presents a potential solution, allowing for the creation of allogeneic cell therapies that are broadly applicable across patient populations. Research efforts are exploring strategies such as human leukocyte antigen (HLA) editing and immune cloaking techniques to generate hypoimmunogenic iPSC lines that can evade immune detection without compromising their therapeutic efficacy. Looking ahead, the continued advancement of iPSC technology, coupled with interdisciplinary collaborations in stem cell biology, bioengineering, and oncology, will be critical in unlocking the full potential of iPSC-based hepatic cancer therapies. The integration of artificial intelligence (AI) and machine learning in iPSC research is also expected to accelerate discoveries by enabling predictive modeling of differentiation pathways, optimizing cell manufacturing processes, and identifying new therapeutic targets. As these technologies converge, the future of hepatic cancer treatment may see a shift toward more personalized, regenerative, and immune-based approaches driven by iPSC innovations. In conclusion, the rapid progress in iPSC technology is reshaping the landscape of hepatic cancer therapy by providing novel solutions for disease modeling, drug screening, regenerative medicine, gene therapy, and immunotherapy. Advances in iPSC reprogramming, differentiation, gene editing, and immune engineering have enhanced the safety, efficacy, and scalability of iPSC-based therapies, bringing them closer to clinical application. While challenges remain in terms of tumorigenicity, cost, and immune compatibility, ongoing research and technological innovations continue to refine iPSC-based strategies for combating liver cancer. As these approaches evolve, iPSC technology holds immense potential to revolutionize hepatic cancer treatment, offering more effective, personalized, and potentially curative therapies for patients facing this devastating disease.
Clinical Implications and Current Challenges
The clinical implications of induced pluripotent stem cell (iPSC) technology in hepatic cancer therapy are vast, offering potential breakthroughs in personalized medicine, regenerative treatments, drug discovery, and immunotherapy. However, despite these promising advancements, significant challenges remain in translating iPSC-based therapies from bench to bedside. One of the most important clinical implications of iPSC technology is its ability to generate patient-specific hepatocytes for transplantation, which could serve as an alternative to liver transplantation in patients with hepatocellular carcinoma (HCC) and end-stage liver disease. (Zhu, H., Xue, 2021). The severe shortage of donor organs and the risk of immune rejection in allogeneic transplantation have long been barriers to effective treatment, but iPSC-derived hepatocytes offer a potentially unlimited and patient-matched source of functional liver cells, reducing the need for immunosuppression and improving long-term graft survival. Additionally, iPSC-derived hepatocytes can be used for disease modeling and drug screening, allowing for personalized treatment strategies tailored to an individual patient’s genetic and molecular profile. By using iPSC-derived hepatocytes from HCC patients, researchers can study tumor-specific mutations and epigenetic changes in vitro, identifying novel drug targets and testing the efficacy of chemotherapy, targeted therapies, and immunotherapies in a controlled laboratory setting before administering them to patients. This approach, often referred to as precision medicine, could help improve treatment response rates and reduce adverse effects associated with ineffective therapies. Furthermore, iPSC-derived hepatocytes provide an invaluable tool for studying drug-induced hepatotoxicity, a major concern in cancer treatment, as many chemotherapeutic agents and targeted drugs can cause severe liver damage. Screening drugs on patient-derived iPSC hepatocytes can help predict hepatotoxic effects in specific genetic backgrounds, leading to the development of safer and more effective treatments. Another crucial clinical implication of iPSC technology is its potential to revolutionize hepatic cancer immunotherapy. The generation of iPSC-derived chimeric antigen receptor (CAR) T cells and natural killer (NK) cells offers a scalable and standardized approach to immunotherapy, overcoming some of the limitations of autologous cell therapies. Traditional CAR-T cell therapy for solid tumors, including HCC, has faced challenges such as poor tumor infiltration, an immunosuppressive microenvironment, and limited persistence of engineered T cells. iPSC-derived CAR-T cells provide an off-the-shelf solution that can be mass-produced from a single, genetically optimized iPSC line, ensuring uniformity in potency and function while reducing manufacturing time and costs. These engineered T cells can be further enhanced with gene-editing techniques, such as CRISPR-Cas9, to improve their resistance to immune evasion mechanisms employed by liver cancer cells. Additionally, iPSC-derived NK cells have demonstrated significant promise in HCC treatment, as they do not rely on antigen specificity and can directly recognize and eliminate cancer cells through innate immune mechanisms. Unlike traditional NK cell therapies, which require donors and expansion processes, iPSC-derived NK cells can be produced in large quantities with enhanced cytotoxic properties, such as high-affinity receptors and checkpoint inhibition resistance. The combination of iPSC-derived immune cells with existing immunotherapies, including immune checkpoint inhibitors and cytokine therapies, may lead to more effective treatment regimens for HCC patients. However, despite these exciting clinical implications, several challenges must be addressed before iPSC-based therapies can be widely implemented in hepatic cancer treatment. One of the primary concerns is the risk of tumorigenicity associated with iPSC-derived cells. Since iPSCs have unlimited proliferative potential, there is always a risk of residual undifferentiated cells forming teratomas or contributing to uncontrolled cell growth. Ensuring the complete differentiation of iPSC-derived hepatocytes or immune cells is critical for minimizing this risk, and advanced quality control measures, such as single-cell RNA sequencing and flow cytometry-based purification, are being explored to enhance the safety of these cell therapies. Another major challenge is the scalability and cost-effectiveness of iPSC-derived therapies. Generating iPSCs, differentiating them into functional cell types, and ensuring their safety and efficacy require extensive time, expertise, and financial resources. Current differentiation protocols for hepatocytes still face issues related to incomplete maturation, low efficiency, and variability between batches, making it difficult to produce large-scale, standardized cell populations suitable for clinical application. Automation, bioreactor-based expansion, and advanced biomaterials are being investigated to improve the efficiency and cost-effectiveness of iPSC-derived therapies, but these technologies are still in the early stages of development. Furthermore, immune compatibility remains a key challenge in iPSC-based hepatic cancer therapy. While autologous iPSC-derived therapies offer the advantage of being patient-specific, they require individualized cell production, which is time-intensive and expensive. Allogeneic iPSC-derived therapies, which use universal donor cell lines, present a more scalable solution but carry the risk of immune rejection. Strategies such as human leukocyte antigen (HLA) editing, immune cloaking techniques, and the development of hypoimmunogenic iPSC lines are being explored to address this issue and create universally compatible iPSC-derived cell products. Regulatory and ethical considerations also pose significant barriers to the clinical translation of iPSC-based therapies for hepatic cancer. The long-term safety of iPSC-derived cells has not been fully established, and rigorous preclinical testing is required before these therapies can be approved for human use. Regulatory agencies, such as the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA), require extensive safety and efficacy data, including tumorigenicity risk assessments, genomic stability analyses, and long-term follow-up studies in animal models and clinical trials. Ethical concerns regarding the use of iPSCs, particularly in gene-editing applications, must also be addressed, ensuring that these technologies are used responsibly and equitably. Additionally, standardization of manufacturing processes and quality control protocols is essential to ensure the reproducibility and consistency of iPSC-derived cell therapies across different research laboratories and clinical centers. As research continues to advance, interdisciplinary collaborations between stem cell biologists, oncologists, bioengineers, and regulatory agencies will be essential to overcoming these challenges and translating iPSC-based hepatic cancer therapies into clinical practice. The integration of artificial intelligence (AI) and machine learning in iPSC research is also expected to accelerate progress by optimizing differentiation protocols, predicting patient responses to therapy, and identifying novel drug targets. Looking forward, the future of hepatic cancer therapy may see a shift toward more personalized, regenerative, and immune-based treatments driven by iPSC technology.
Future Directions in iPSC-based Hepatic Cancer Treatment
The future of induced pluripotent stem cell (iPSC)-based hepatic cancer treatment holds immense promise, with ongoing advancements in regenerative medicine, gene editing, immunotherapy, and bioengineering paving the way for more effective and personalized therapeutic strategies. One of the most exciting directions is the refinement of iPSC-derived hepatocyte-like cells (HLCs) for transplantation and liver tissue regeneration. While current differentiation protocols have improved the functionality of iPSC-derived hepatocytes, challenges such as incomplete maturation, limited engraftment efficiency, and immune compatibility still hinder their clinical application. Future research will likely focus on optimizing 3D culture systems, organoid models, and scaffold-based liver constructs to enhance the structural and functional properties of iPSC-derived liver cells. (Zhu, H., Xue, C (2021). Additionally, the integration of vascularized liver organoids with microfluidic systems, or "liver-on-a-chip" technology, could revolutionize in vitro disease modeling and drug screening, providing a highly accurate platform for testing patient-specific therapies before clinical application. Another major future direction is the advancement of gene-editing technologies, particularly CRISPR-Cas9, in iPSC-based hepatic cancer therapy. By leveraging precise genome-editing techniques, researchers can correct genetic mutations associated with hepatocellular carcinoma (HCC), engineer hepatocytes with enhanced tumor-suppressing properties, and develop more effective gene therapy strategies. Moreover, the use of epigenetic editing tools could allow for the targeted reprogramming of cancerous cells back to a normal state, opening new possibilities for reversing tumor progression. Immunotherapy is also expected to see significant progress with iPSC-derived immune cells, such as chimeric antigen receptor (CAR)-T cells and natural killer (NK) cells. The ability to generate off-the-shelf, standardized immune cells from a single iPSC source will likely overcome the limitations of current autologous therapies, making treatment more accessible and cost-effective. Future studies will focus on enhancing the persistence, tumor-infiltration capacity, and resistance to immunosuppressive mechanisms in iPSC-derived immune cells, ensuring their long-term efficacy against liver cancer. The combination of iPSC-derived immune therapies with existing checkpoint inhibitors, cytokine therapies, and cancer vaccines could lead to more comprehensive and durable anti-tumor responses. Additionally, the emerging field of iPSC-derived extracellular vesicle (EVs) holds significant potential for hepatic cancer treatment. EVs derived from iPSC-hepatocytes or immune cells can serve as natural drug delivery vehicles, transporting therapeutic molecules such as small interfering RNA (siRNA), microRNA (miRNA), or chemotherapeutic agents directly to liver cancer cells. Future research will explore the engineering of iPSC-derived EVs for targeted delivery, ensuring increased specificity and reduced systemic toxicity in cancer treatment. Another promising direction is the development of universal donor iPSC lines with reduced immunogenicity, which could eliminate the need for patient-specific cell generation and facilitate the large-scale production of iPSC-derived therapies. By utilizing gene-editing techniques to remove or modify human leukocyte antigen (HLA) expression, researchers aim to create hypoimmunogenic iPSC lines that can be used in allogeneic transplantation without triggering immune rejection. The application of artificial intelligence (AI) and machine learning in iPSC-based research is also expected to accelerate progress by optimizing differentiation protocols, predicting patient responses to therapies, and identifying novel drug targets. AI-driven analysis of large-scale genomic and transcriptomic data could lead to more efficient screening of iPSC-derived hepatocytes and immune cells, improving their therapeutic efficacy. As these technologies converge, the future of hepatic cancer treatment will likely shift towards more personalized, regenerative, and immune-based approaches, ultimately improving patient outcomes and survival rates. However, before these innovations can be widely implemented, challenges such as regulatory approval, scalability, safety, and cost-effectiveness must be addressed through continued interdisciplinary research and clinical trials.
CONCLUSION
In conclusion, induced pluripotent stem cell (iPSC) technology holds immense promise for revolutionizing hepatic cancer therapy through regenerative medicine, personalized drug screening, gene therapy, and immunotherapy. The ability to generate patient-specific hepatocytes offers new avenues for liver tissue regeneration and transplantation, while iPSC-derived immune cells, such as CAR-T and NK cells, provide innovative approaches to cancer immunotherapy. Furthermore, advancements in gene editing, 3D organoid models, and extracellular vesicle-based drug delivery are expanding the potential applications of iPSCs in hepatocellular carcinoma (HCC) treatment. (Ang, L. T., Tan, A. K (2021) However, despite these advancements, several challenges remain, including the risk of tumorigenicity, immune rejection, scalability, and regulatory hurdles. Future research will focus on refining differentiation protocols, improving safety measures, and developing universally compatible iPSC lines to overcome these limitations. Additionally, the integration of artificial intelligence (AI) in iPSC research is expected to accelerate drug discovery and optimize treatment strategies. As these technologies continue to evolve, iPSC-based therapies have the potential to significantly improve survival rates, reduce treatment-related toxicities, and ultimately provide curative options for patients with hepatic cancer. With continued interdisciplinary collaboration and rigorous clinical trials, iPSC technology could become a cornerstone in the future of liver cancer treatment.
REFERENCES



Jyoti Sharma, Dilshad Malik, Harmanjot Kaur, The Potential of Induced Pluripotent Stem Cells in Hepatic Cancer Therapy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3720-3733. https://doi.org/10.5281/zenodo.18063224
 10.5281/zenodo.18063224
10.5281/zenodo.18063224
