
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dept. of Pharmacy: Shri Ram College of Pharmacy Muzaffarnagar U.P India.
Hypertension, or high blood pressure, is a major risk factor for cardiovascular diseases, accounting for a significant burden on global healthcare systems. Despite the availability of various classes of antihypertensive drugs, issues such as side effects, drug resistance, and economic constraints limit their universal applicability. This has prompted a growing interest in alternative therapeutic options, particularly plant-based medicines. Herbal remedies, long utilized in traditional medical systems such as Ayurveda, have shown promising results in managing hypertension through mechanisms such as vasodilation, diuresis, inhibition of angiotensin-converting enzyme, antioxidant effects, and modulation of inflammatory pathways. This review presents a comprehensive analysis of selected medicinal plants including Rauwolfia serpentina, Allium sativum, Terminalia arjuna, Ocimum sanctum, and Andrographis paniculata, highlighting their phytochemical constituents, pharmacological actions, and evidence from experimental and clinical studies. Although current scientific data support their efficacy, several limitations such as lack of standardization, poor bioavailability, and insufficient clinical trials remain. Integrating herbal therapy with modern medicine may provide a safe, cost-effective, and holistic approach to hypertension management. This paper also addresses the challenges and future directions required for the broader acceptance and regulatory approval of herbal antihypertensives. Further exploration of their molecular mechanisms and long-term clinical trials will be essential to transform these age-old remedies into evidence-based therapeutics.
High blood pressure, or hypertension, is one of the most pressing health concerns of the 21st century. Often labeled a "silent killer," it quietly damages blood vessels and vital organs over time without showing clear early symptoms. As a leading contributor to heart attacks, strokes, kidney disease, and other cardiovascular complications, its impact is both global and profound. According to recent health reports, a substantial portion of the adult population is now affected, with rising trends seen in both urban and rural areas, especially in developing countries. Modern medicine offers a wide range of pharmacological options to control hypertension. These include diuretics, calcium channel blockers, beta-blockers, and ACE inhibitors, among others. While effective in lowering blood pressure, these drugs are often associated with limitations such as adverse side effects, long-term dependency, and high treatment costs. As a result, many patients either discontinue therapy or look for alternative or supportive remedies. One area gaining renewed attention is the use of medicinal plants and herbal therapies. In traditional Indian medicine systems like Ayurveda, numerous herbs have been used for centuries to regulate blood pressure and improve heart health. Today, this ancient wisdom is being revisited through the lens of modern science. Herbal drugs like Rauwolfia serpentina, Allium sativum, and Terminalia arjuna have shown promising results in preliminary clinical trials and laboratory studies. The objective of this review is to explore some of the most well-documented herbal options for hypertension. By focusing on their active compounds, mechanisms of action, and evidence from both traditional use and contemporary research, this paper aims to present a balanced view of how herbal therapies may serve as effective and safer alternatives—or complements—to conventional antihypertensive drugs.
2. Epidemiology and Global Burden of Hypertension
Hypertension has steadily evolved into a major public health concern, affecting populations across all continents, age groups, and economic strata. It is no longer considered a condition limited to affluent societies or aging populations. In fact, recent trends indicate a noticeable rise in prevalence among younger adults and in low- and middle-income countries, where healthcare access and lifestyle transitions contribute significantly to the growing numbers. As of the latest estimates by the World Health Organization, more than 1.28 billion adults globally suffer from elevated blood pressure, with nearly half unaware of their condition. The disease is often asymptomatic in its early stages, earning it the moniker of a “silent killer.” Uncontrolled hypertension is strongly associated with life-threatening complications such as stroke, myocardial infarction, heart failure, and chronic kidney disease. It is also a key contributor to premature mortality and disability-adjusted life years (DALYs) worldwide. In India, hypertension affects an estimated 30% of the adult population, with prevalence rates even higher in urban centers. Rural regions are not immune either, where detection and treatment rates are considerably lower. A disturbing pattern is the sharp increase in hypertensive cases coexisting with other non-communicable diseases like diabetes and obesity. This clustering of risk factors is exerting tremendous pressure on healthcare systems that are often already stretched thin. Socioeconomic shifts, dietary changes, physical inactivity, and psychological stress are contributing to the worsening of the hypertension burden. Despite greater awareness and the availability of medications, global control rates remain low. This gap between diagnosis and effective management underscores the urgent need for both preventive strategies and broader therapeutic options, including non-pharmacological and herbal approaches that are affordable, accessible, and culturally acceptable.
3. Pathophysiology of Hypertension
Hypertension arises from a complex interplay of genetic, physiological, and environmental factors that disrupt the delicate mechanisms regulating blood pressure. At its core, blood pressure is maintained by a balance between cardiac output and peripheral vascular resistance. Any persistent alteration in this balance can lead to elevated arterial pressure. One of the central systems involved in blood pressure control is the renin-angiotensin-aldosterone system (RAAS). Overactivity of RAAS results in increased levels of angiotensin II, a potent vasoconstrictor, and aldosterone, which promotes sodium and water retention. These changes raise blood volume and vascular resistance, both of which contribute to hypertension. Another major contributor is the sympathetic nervous system (SNS). Chronic activation of SNS, often triggered by stress, obesity, or metabolic disorders, leads to sustained vasoconstriction, increased heart rate, and enhanced cardiac output. Over time, this sympathetic overdrive damages blood vessels and impairs baroreceptor sensitivity. Endothelial dysfunction also plays a significant role in the pathogenesis of hypertension. The endothelium, which lines the inner walls of blood vessels, is responsible for producing vasodilatory substances like nitric oxide (NO). In hypertension, this protective function is compromised due to oxidative stress and inflammation, leading to increased vascular tone and stiffness. Additionally, renal abnormalities—including impaired sodium excretion and altered pressure-natriuresis relationship—contribute to volume overload. Structural changes in the kidneys can further promote vasoconstriction and resistance to antihypertensive mechanisms. Inflammatory markers, oxidative damage, and genetic mutations affecting ion channels and vascular reactivity have also been identified in many hypertensive individuals. These mechanisms often overlap, making hypertension not a single disease entity but a multifactorial condition with individualized pathophysiology. Understanding these underlying pathways is essential not only for pharmacological treatment but also for exploring how natural remedies—many of which exert antioxidant, diuretic, vasodilatory, or anti-inflammatory actions—can complement conventional approaches in managing blood pressure effectively.
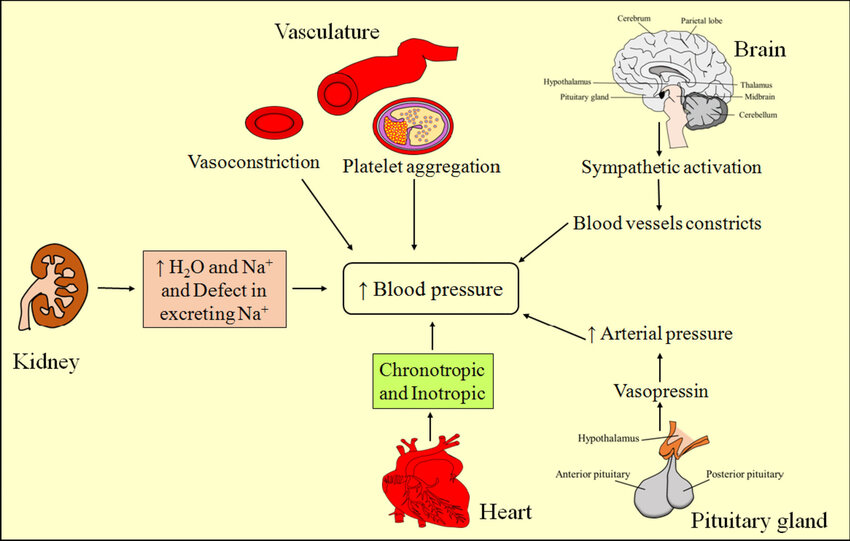
Fig 1: Pathophysiology of Hypertension Ref: Bionanoscience
4. Limitations of Conventional Antihypertensive Therapies
Over the past several decades, the pharmaceutical industry has developed a wide array of antihypertensive drugs—ranging from diuretics and beta-blockers to calcium channel blockers, ACE inhibitors, and angiotensin receptor blockers. These agents have proven effective in reducing elevated blood pressure and lowering the risk of complications such as stroke and heart failure. However, despite these advances, conventional antihypertensive therapy is not without its shortcomings. One of the most prominent issues is adverse effects. Many patients report fatigue, dizziness, electrolyte imbalances, sexual dysfunction, and mood changes associated with long-term drug use. These side effects often lead to poor adherence, which in turn diminishes the effectiveness of treatment. In fact, non-compliance remains one of the major barriers to successful hypertension control globally. Another concern is individual variability in drug response. Not all patients respond uniformly to standard antihypertensive medications. Genetic differences, coexisting conditions like diabetes or kidney disease, and even lifestyle factors can affect how a drug performs in the body. As a result, trial-and-error approaches are commonly used, prolonging the time needed to achieve stable blood pressure control. Polypharmacy, particularly among elderly patients or those with multiple chronic illnesses, introduces the risk of drug–drug interactions. The need to manage coexisting diseases often results in a complicated medication regimen, which can overwhelm patients and increase the likelihood of missed doses or dosing errors. Furthermore, long-term dependency on synthetic medications without addressing underlying lifestyle causes has raised questions about sustainability. While pharmacological treatment remains essential in many cases, it is reactive rather than preventive in nature. It often manages symptoms without necessarily reversing the root causes of high blood pressure, such as chronic inflammation, oxidative stress, or endothelial dysfunction. Lastly, economic burden cannot be ignored. In low-income communities and developing nations, the cost of lifelong medication, coupled with inadequate access to regular health check-ups, poses a serious obstacle. This gap between need and availability underlines the importance of exploring cost-effective, culturally acceptable, and safer alternatives. In this context, herbal and traditional therapies—many of which have been used for centuries—are receiving renewed interest. Their multifaceted mechanisms, affordability, and relatively lower risk of adverse effects suggest that they may play a valuable role either as standalone treatments in mild cases or as adjuncts in more complex therapeutic plans.
5. Role of Herbal Medicines in Blood Pressure Regulation
Herbal medicines have long been used in traditional systems of healthcare across the world, including Ayurveda, Traditional Chinese Medicine (TCM), and Unani. With the rising limitations of conventional antihypertensive drugs—ranging from adverse effects to poor compliance—there is increasing interest in botanicals as complementary or alternative therapies for managing elevated blood pressure. Several plant-derived compounds have demonstrated vasodilatory, diuretic, anti-inflammatory, and antioxidant properties, all of which contribute to blood pressure reduction. These effects are often achieved through multiple mechanisms of action, which may include inhibition of the renin-angiotensin-aldosterone system (RAAS), calcium channel blocking, modulation of nitric oxide (NO) pathways, and improved endothelial function. For example, Rauwolfia serpentina, a well-known antihypertensive herb in Ayurveda, contains the alkaloid reserpine, which reduces sympathetic nerve activity by depleting catecholamines. Similarly, Allium sativum (garlic) is rich in sulfur-containing compounds like allicin, which promote vasodilation and improve lipid profiles, contributing to lower blood pressure. Hibiscus sabdariffa has gained attention for its anthocyanin content, which is believed to inhibit ACE activity and promote urinary sodium excretion. A major advantage of herbal interventions is their multi-targeted approach, offering not just blood pressure control but also protection against complications such as oxidative stress and vascular inflammation—factors that are often overlooked by conventional drugs. Moreover, herbal preparations tend to have a favorable safety profile when used appropriately, making them suitable for long-term use in mild to moderate cases of hypertension, or as adjunct therapy in more severe cases. However, their effectiveness is highly dependent on quality control, dosage standardization, and the presence of bioactive constituents, which remain challenges in the absence of regulatory frameworks. Another key strength lies in cultural familiarity and affordability, especially in resource-limited settings. In rural populations, where modern healthcare facilities may be inaccessible or unaffordable, the use of locally available medicinal plants remains a viable and sustainable option. Despite their promising role, herbal medicines should not be viewed as replacements for clinically indicated pharmaceuticals, especially in patients with severe or complicated hypertension. Rather, they offer a complementary pathway that can enhance the overall therapeutic outcome when integrated into a broader, patient-centered treatment strategy.
6. Promising Herbal Drugs for Hypertension: A Scientific Overview
Several herbal drugs have shown substantial promise in the management of hypertension through diverse pharmacological mechanisms. While their clinical acceptance is still evolving, a growing body of research has confirmed the therapeutic potential of various plant-derived bioactive compounds in regulating blood pressure. Below is an overview of some widely studied medicinal plants:
6.1 Rauwolfia serpentina (Sarpagandha)

Fig 6.1: Rauwolfia serpentina (Sarpagandha)
Family:Apocynaceae
Rauwolfia serpentina is one of the earliest plants used in the treatment of hypertension, particularly in Ayurvedic medicine. Its principal alkaloid, reserpine, acts by depleting catecholamines from peripheral sympathetic nerve endings, thereby reducing peripheral vascular resistance and lowering blood pressure. Although its use has declined due to CNS side effects, it remains a historical cornerstone in herbal antihypertensive therapy.
6.2 Allium sativum (Garlic)

Fig 6.2 : Allium sativum (Garlic)
Family:Amaryllidaceae
Garlic is known for its vasodilatory and lipid-lowering effects. Its key active compound, allicin, improves nitric oxide (NO) availability, leading to relaxation of vascular smooth muscle. Clinical trials have suggested that regular intake of garlic can significantly reduce both systolic and diastolic blood pressure, particularly in patients with mild to moderate hypertension.
6.3 Hibiscus sabdariffa (Roselle)

Fig 6.3: Allium sativum (Garlic)
Family:Malvaceae
The calyces of Hibiscus sabdariffa are rich in anthocyanins and hibiscus acid, both of which have shown ACE inhibitory activity. Several randomized clinical trials have reported modest but statistically significant reductions in blood pressure with hibiscus tea consumption, with added antioxidant and diuretic benefits.
6.4 Terminalia arjuna (Arjuna)

Fig 6.4: Terminalia arjuna (Arjuna)
Family:Combretaceae
Traditionally used in the management of cardiovascular disorders, Terminalia arjuna exhibits antihypertensive activity due to its flavonoids, tannins, and coenzyme Q10-like constituents. These phytoconstituents help improve myocardial function and vascular compliance, leading to reduced systolic blood pressure in clinical settings.
6.5 Camellia sinensis (Green Tea)

Fig 6.5 Camellia sinensis (Green Tea)
Family:Theaceae
Green tea polyphenols, particularly epigallocatechin gallate (EGCG), have been studied for their vasorelaxant and antioxidant properties. By improving endothelial function and reducing oxidative stress, green tea contributes to blood pressure regulation, although results across studies are somewhat variable.
6. 6 Withania somnifera (Ashwagandha)

Fig 6. 6 Withania somnifera (Ashwagandha)
Family:Solanaceae
Ashwagandha is considered an adaptogen with mild antihypertensive effects. It reduces stress-induced hypertension by modulating cortisol levels and enhancing parasympathetic activity. Some studies also report its ability to lower blood pressure by reducing systemic inflammation and improving vascular tone.
6.7 Moringa oleifera (Drumstick Tree)

Fig 6.7 Moringa oleifera (Drumstick Tree)
Family:Moringaceae
Leaves of Moringa oleifera contain high levels of quercetin, which has demonstrated blood pressure-lowering effects in experimental models. Its diuretic and calcium channel blocking properties make it a candidate for adjunctive hypertension therapy.
6.8 acopa monnieri (Brahmi)

Fig 6.8 acopa monnieri (Brahmi)
Family:Plantaginaceae
Primarily known for its cognitive-enhancing effects, Bacopa also exhibits vasodilatory and anxiolytic properties. It helps reduce stress-related hypertension and has shown promise in experimental models for lowering systolic blood pressure.
6.9 Coleus forskohlii (Makandi)
Fig 6. 9 Coleus forskohlii (Makandi)
Family:Lamiaceae
The root contains forskolin, a compound that directly activates adenylate cyclase, increasing cAMP levels. This leads to vasodilation and a reduction in blood pressure. Coleus is often used in traditional Indian medicine for managing high blood pressure and heart conditions.
6.10 Nigella sativa (Black Seed)

Fig 6. 10 Nigella sativa (Black Seed)
Family: Ranunculaceae
Nigella seeds contain thymoquinone, which has both antihypertensive and cardioprotective effects. It reduces blood pressure through calcium channel blocking and diuretic actions, along with anti-inflammatory benefits. These herbs, when appropriately prepared and administered, offer a multi-targeted approach to managing hypertension. However, variability in bioactive content, dosage standardization, and lack of large-scale clinical trials continue to be barriers to their mainstream acceptance. Integrating these herbal options within modern therapeutic frameworks requires stringent pharmacological and clinical evaluations.
7. Mechanisms of Action of Herbal Antihypertensive Agents
The antihypertensive effects of herbal medicines are largely attributed to their ability to modulate various physiological pathways involved in blood pressure regulation. Unlike conventional drugs that often target a single mechanism, herbs exert multifaceted actions through a combination of phytochemicals that influence vascular tone, fluid balance, and neurohormonal regulation. The major mechanisms are discussed below:
7.1 Renin-Angiotensin-Aldosterone System (RAAS) Inhibition
Many plant-based compounds exhibit ACE (angiotensin-converting enzyme) inhibitory activity, which prevents the conversion of angiotensin I to the potent vasoconstrictor angiotensin II. By reducing angiotensin II levels, these herbs lower peripheral resistance and blood pressure.
7.2 Calcium Channel Blockade
Calcium ions play a critical role in vascular smooth muscle contraction. Some herbal constituents act as natural calcium channel blockers, preventing calcium influx into the cells, leading to vasodilation.
7.3 Nitric Oxide (NO) Modulation and Endothelial Function
Nitric oxide is a key vasodilator synthesized by endothelial cells. Certain herbal extracts enhance NO bioavailability, leading to improved endothelial relaxation and reduced arterial stiffness.
7.4 Diuretic Effects
Diuresis reduces plasma volume and subsequently lowers blood pressure. Some herbs naturally promote fluid excretion from the kidneys, acting as mild diuretics.
7.5 Antioxidant and Anti-inflammatory Activity
Oxidative stress and chronic inflammation contribute to vascular dysfunction and hypertension. Numerous herbs contain flavonoids, polyphenols, and alkaloids with strong antioxidant properties that protect vascular endothelium.
7.6 Sympathetic Nervous System Modulation
Stress-induced activation of the sympathetic nervous system increases heart rate and vascular resistance. Some herbal adaptogens reduce sympathetic tone and normalize the hypothalamic-pituitary-adrenal (HPA) axis.
7.7 Potassium Channel Activation
Few herbal compounds may facilitate potassium efflux by opening ATP-sensitive potassium channels in vascular smooth muscle, promoting vasodilation.
7.8 Lipid Profile and Metabolic Regulation
Table: 7.8 Lipid Profile and Metabolic Regulation
|
Herb |
Mechanism |
Key Bioactive Compound |
|
Hibiscus sabdariffa |
ACE inhibition, diuretic, antioxidant |
Anthocyanins, hibiscus acid |
|
Allium sativum |
NO modulation, RAAS inhibition, antioxidant |
Allicin |
|
Coleus forskohlii |
Adenylate cyclase activation, calcium channel block |
Forskolin |
|
Withania somnifera |
Sympathetic inhibition, anti-inflammatory |
Withanolides |
|
Moringa oleifera |
Calcium channel block, antioxidant |
Quercetin |
|
Camellia sinensis |
Endothelial function improvement, antioxidant |
EGCG |
|
Nigella sativa |
Diuretic, calcium channel block, anti-inflammatory |
Thymoquinone |
Dyslipidemia and insulin resistance often coexist with hypertension. Some herbs have shown benefits in regulating lipid metabolism and glucose homeostasis, indirectly contributing to blood pressure control.
8. Advantages of Herbal Therapies over Conventional Drugs in Hypertension Management
The increasing interest in herbal medicines for hypertension is largely driven by the limitations associated with conventional pharmacological treatments and the broader appeal of plant-based therapies. A significant number of hypertensive individuals either experience adverse effects from standard medications or develop resistance, leading to poor compliance. In this context, herbal therapies have emerged as a complementary or alternative solution, offering several distinct advantages. One of the foremost benefits of herbal antihypertensive agents is their multifaceted mode of action. Unlike synthetic drugs that often target a single physiological pathway, herbal remedies typically contain a variety of bioactive compounds capable of acting on multiple mechanisms simultaneously. This includes vasodilation, diuretic activity, calcium channel modulation, antioxidant action, and inhibition of the renin-angiotensin system—all of which collectively contribute to better blood pressure regulation. Another major advantage lies in the minimal side effect profile associated with many herbal preparations. While no treatment is entirely devoid of risks, properly prepared herbal products tend to have fewer and less severe adverse reactions compared to conventional drugs, particularly when used at therapeutic doses under professional guidance. Additionally, long-term safety is often cited as a strength of herbal interventions. Many of these plants have been used in traditional medicine for centuries, with a history of safe and sustained use, especially in cultures where herbal knowledge is deeply rooted. Cost-effectiveness is another compelling factor, especially in low-income or resource-limited settings. Herbal medicines are often locally available and affordable, reducing the economic burden on patients and healthcare systems. This accessibility also enhances treatment adherence in rural populations, where modern pharmaceuticals may be too costly or difficult to obtain. Furthermore, there is a growing body of scientific evidence supporting the efficacy of several herbal antihypertensives, such as Rauwolfia serpentina, Allium sativum, and Hibiscus sabdariffa. These herbs not only lower blood pressure but may also improve lipid profiles and reduce oxidative stress, providing broader cardiovascular protection. Importantly, herbal therapies may offer better patient acceptance due to their natural origin, especially among individuals who prefer holistic or integrative treatment models. The perception of "natural" often equates to "safer" in public opinion, leading to higher confidence in and adherence to treatment plans involving botanicals. Despite these advantages, it is essential to recognize that herbal medicines are not free from concerns. Variability in composition, lack of standardization, and potential herb-drug interactions underscore the need for regulation and professional oversight. Nonetheless, when properly formulated and administered, herbal therapies hold a promising place in the integrated management of hypertension.
CONCLUSION
Hypertension continues to be one of the most pressing global health challenges, contributing significantly to cardiovascular morbidity and mortality. Despite the availability of various conventional antihypertensive drugs, issues such as side effects, drug resistance, economic burden, and patient non-compliance highlight the limitations of current pharmacotherapy. In this context, herbal medicines offer a promising complementary or alternative approach for the management of high blood pressure. Drawing from centuries of traditional medical practices and an increasing volume of modern scientific evidence, several herbal drugs—such as Rauwolfia serpentina, Allium sativum, Terminalia arjuna, Hibiscus sabdariffa, and Withania somnifera—have demonstrated potential antihypertensive effects through diverse mechanisms. These include modulation of the renin-angiotensin system, antioxidant activity, calcium channel blocking, diuresis, and endothelial function improvement. Importantly, many of these herbs offer added benefits such as improved lipid profiles, reduced oxidative stress, and anti-inflammatory action, making them suitable for holistic cardiovascular care. Moreover, the generally favorable safety profiles, affordability, and cultural acceptability of herbal therapies make them particularly valuable in low-resource settings. However, challenges remain regarding standardization, dosage optimization, potential herb-drug interactions, and regulatory oversight. For herbal medicines to be fully integrated into mainstream hypertension management, there is an urgent need for well-designed clinical trials, strict quality control, and public health policy support. Future research should focus not only on validating efficacy but also on understanding long-term safety and synergistic interactions with conventional drugs. In conclusion, herbal antihypertensive agents represent a valuable and underutilized resource in the fight against hypertension. When combined with modern pharmacology and clinical practice, these time-tested remedies have the potential to offer safer, more effective, and more accessible hypertension care worldwide.
REFERENCES


Dr. Girendra Kumar Gautam, KM. Sweta* Jyoti Jain, Therapeutic Potential of Herbal Remedies in the Management of Hypertension: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2049-2061 https://doi.org/10.5281/zenodo.16908660
 10.5281/zenodo.16908660
10.5281/zenodo.16908660