1,2 General Physician, University of Sinú, Cartagena
3 General Physician, University of La Sabana, Bogotá
4,9 General Physician, Rafael Nuñez University Corporation, Cartagena
5,6 General Physician, University of Sucre, Sincelejo
7 General Physician, Metropolitan University, Barranquilla
8 General Physician, University of Tolima
The neutrophil-to-lymphocyte ratio (NLR) is an inflammatory biomarker derived from the complete blood count that reflects the dynamic balance between innate and adaptive immunity. In recent years, multiple studies have demonstrated its prognostic utility in systemic infections, particularly in sepsis, community-acquired pneumonia, and COVID-19. Its low cost, wide availability, and rapid assessment make it an attractive tool in both high- and low-resource settings. This review analyzes the pathophysiological basis of NLR, available clinical evidence, reported cutoff values, comparison with other biomarkers, and its main limitations. NLR represents a complementary prognostic marker with independent value in predicting severity and mortality in systemic infections.
Systemic infections continue to be one of the leading causes of morbidity and mortality worldwide. Sepsis, defined as life-threatening organ dysfunction secondary to a dysregulated host response to infection, represents a significant diagnostic and therapeutic challenge. In this context, early identification of patients at high risk of clinical deterioration is essential. The neutrophil-lymphocyte ratio has emerged as a simple inflammatory marker that integrates two key components of the immune response: reactive neutrophilia and lymphopenia induced by systemic stress. Several studies have demonstrated its association with hospital mortality and clinical severity (1,3).
DEVELOPMENT
The neutrophil-lymphocyte ratio (NLR) has established itself as an inflammatory biomarker of growing interest in the prognostic stratification of patients with systemic infections. Its basis lies in the quantitative integration of two complementary immunological phenomena: the exacerbated activation of innate immunity, reflected by neutrophilia, and the relative suppression of adaptive immunity, evidenced by lymphopenia. In the context of sepsis and other severe systemic infections, this immunological dysregulation occurs simultaneously and dynamically, creating a biological environment characterized by initial hyperinflammation followed by compensatory immunoparalysis. Several observational studies have shown that INL at hospital admission is significantly associated with higher in-hospital mortality, the need for vasopressor support, and the development of multiple organ dysfunction (1,3).
From a pathophysiological point of view, neutrophilia in systemic infections is caused by bone marrow stimulation mediated by proinflammatory cytokines such as IL-6 and TNF-α, as well as by demargination secondary to endogenous catecholamines. Excessive neutrophil activation promotes the release of reactive oxygen species, proteolytic enzymes, and the formation of neutrophil extracellular traps (NETs), which contribute to endothelial injury, microthrombosis, and microcirculatory disturbance. At the same time, lymphopenia develops as a result of systemic stress-induced apoptosis, lymphocyte redistribution, and functional suppression of the adaptive response. It has been documented that the persistence of lymphopenia during the first days of hospitalization is an independent predictor of mortality in septic patients (4). By integrating both processes into a single metric, the INL provides a more complete view of the immune status than the isolated total leukocyte count.
In patients with sepsis, multiple analyses have shown that elevated INL values correlate with higher scores on severity scales such as SOFA and APACHE II, as well as with elevated serum lactate concentrations (5). The reported cutoff points vary between 5 and 10, depending on the cohort and methodological design, but consistently show an association with adverse outcomes (1,6). In this context, Figure 1 illustrates the increasing relationship between the INL value and the relative risk of mortality in sepsis, graphically representing the trend observed in clinical studies: as the index increases, the risk of a fatal outcome increases progressively. This behavior suggests that the INL not only acts as a dichotomous marker but also has a proportional prognostic gradient.
In community-acquired pneumonia, the INL has also proven to be significantly useful. Research has shown a correlation between high index values and a higher probability of admission to intensive care units, the need for mechanical ventilation, and 30-day mortality (4,5). In some comparative analyses, the INL showed similar or superior discriminatory capacity to C-reactive protein in identifying patients with severe forms of the disease. This advantage is particularly relevant in settings where advanced biomarkers are not available, as the complete blood count is a universally accessible tool.
During the SARS-CoV-2 pandemic, the INL was extensively studied as a predictor of clinical severity. COVID-19 infection is characterized by cytokine storm, marked neutrophilia, and profound lymphopenia, conditions that significantly increase the index. Meta-analyses have confirmed that LNI values above 6–8 at hospital admission are associated with a higher probability of acute respiratory distress syndrome, ICU admission, and mortality (7,8). Figure 2 graphically represents this relationship, showing the progressive increase in the probability of admission to intensive care as the index value increases. This representation reinforces the concept that the LNI acts as a continuous risk marker rather than a binary variable.
A particularly relevant aspect of the INL is its dynamic behavior during clinical evolution. Not only does the initial value have prognostic significance, but so does its temporal trend. Patients in whom the index increases progressively during the first 48–72 hours are more likely to experience hemodynamic deterioration and therapeutic failure, while a sustained reduction is associated with a better response to antimicrobial treatment and clinical stabilization. Figure 3 illustrates the dynamic evolution of the INL during the first days of hospitalization for systemic infection, showing how an upward trajectory is related to greater severity. This temporal behavior suggests that the INL could be used as a tool for monitoring evolution in addition to an initial prognostic marker (9,10).
In complicated intra-abdominal and urinary infections, the INL has also been useful in differentiating mild cases from complicated forms, particularly in perforated appendicitis and secondary peritonitis. Elevated values have been associated with a higher probability of surgical intervention and postoperative complications. Although cut-off points vary, they generally exceed 8–10 in complicated forms, reinforcing their role as an indicator of inflammatory severity (11).
Compared to other biomarkers, the NLIN has clear logistical advantages: low cost, immediate availability, and no additional technological requirements. However, it lacks etiological specificity and should not replace markers such as procalcitonin in the identification of invasive bacterial infection. Its true strength lies in its integration into combined predictive models, where it can increase overall discriminatory power (12).
Overall, the available evidence supports the neutrophil-lymphocyte ratio as a robust prognostic marker in systemic infections, with the ability to reflect both the intensity of the inflammatory response and the degree of adaptive immune dysfunction. The incorporation of dynamic analysis of the count, as shown in Figures 1, 2, and 3, extends its clinical utility by allowing not only initial risk stratification but also follow-up of the critically ill patient (12).
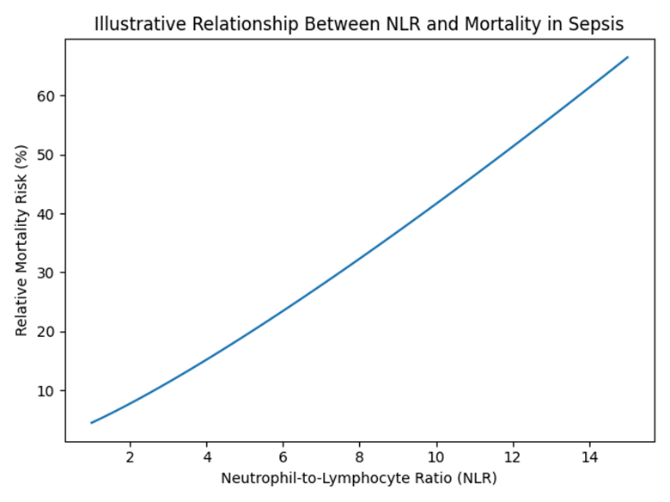
Figure 1. Illustrative relationship between INL and mortality in sepsis.
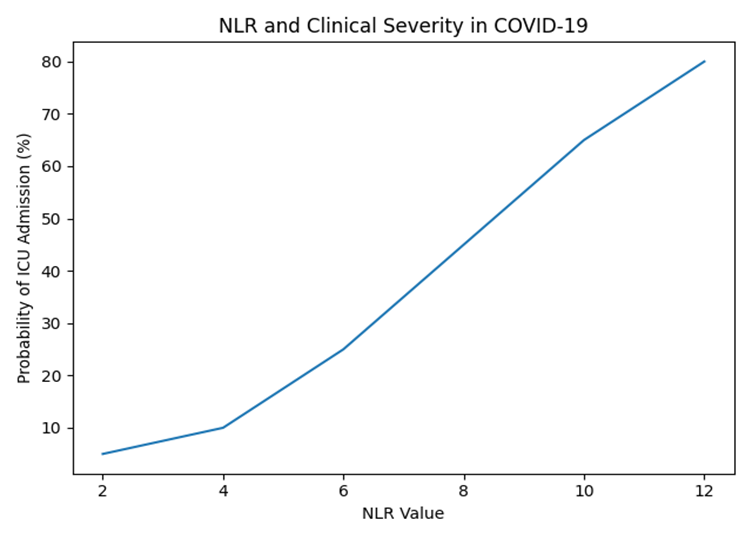
Figure 2. INL and probability of ICU admission in COVID-19.
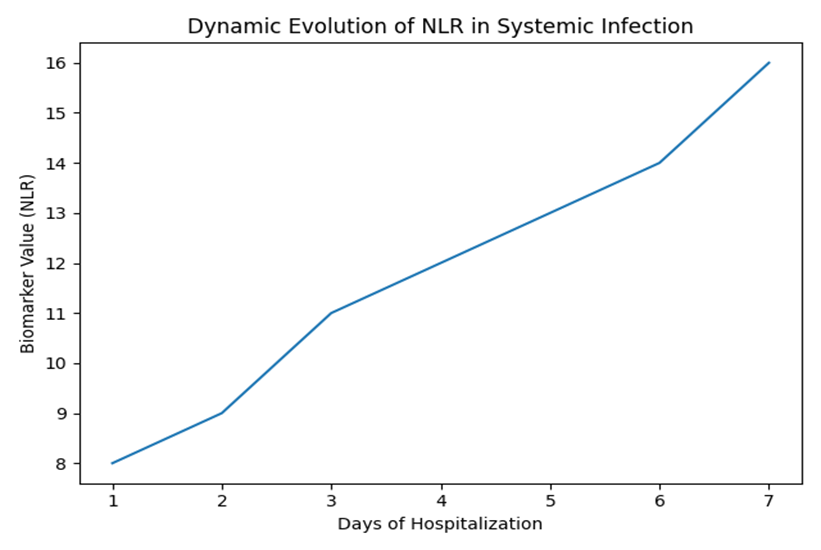
Figure 3. Dynamic evolution of INL during hospitalization.
DISCUSSION
The neutrophil-lymphocyte ratio (NLR) has emerged as an inflammatory biomarker with significant prognostic value in multiple scenarios of systemic infection. Its main strength lies in its methodological simplicity, low cost, and universal availability, as it is derived from a complete blood count, a routine test at any level of care. In contrast, biomarkers such as procalcitonin require specific analytical platforms and generate additional costs that may limit their implementation in health systems with limited resources (13, 14).
However, it is essential to emphasize that the INL should not be interpreted as an absolute substitute for specific biomarkers of bacterial infection. Procalcitonin retains greater etiological specificity in invasive bacterial infections, while serum lactate remains a robust marker of tissue hypoperfusion and organ dysfunction. In this context, the clinical value of INL does not lie in replacing existing tools, but in complementing the initial assessment and strengthening multi-marker predictive models (15).
A relevant aspect is its integration into prognostic scales. Several studies have shown that incorporating INL improves the discriminatory capacity of models such as SOFA or CURB-65, increasing the area under the curve in ROC analysis when added as an independent variable. This suggests that INL could be part of structured clinical algorithms aimed at early risk stratification, especially in emergency departments (16, 17).
From a pathophysiological perspective, the INL has a conceptual advantage over isolated biomarkers, as it simultaneously integrates two dimensions of the immune spectrum: neutrophilic hyperinflammation and adaptive immunosuppression. This dynamic balance is particularly relevant in sepsis, where the coexistence of inflammatory storm and immunoparalysis explains the progression to multiple organ dysfunction. Persistent lymphopenia, indirectly reflected in increased INL, has been associated with increased susceptibility to secondary infections and late mortality (18).
However, heterogeneity in cut-off points is a significant methodological limitation. In sepsis, the proposed values range from 5 to 10; in COVID-19, from 6 to 8; while in intra-abdominal infections, they may exceed 8–10. This variability is due to differences in population, diagnostic criteria, baseline severity, and statistical methodologies used. The lack of standardization limits its universal applicability and makes it difficult to compare studies (19).
Another critical aspect is the influence of confounding variables. The use of systemic corticosteroids, common in critically ill patients, can induce relative neutrophilia and lymphopenia, altering the LNI regardless of the infectious burden. Likewise, hematological diseases, autoimmune processes, surgical stress, or trauma can modify the index without the presence of active infection. Therefore, its interpretation must be made within the overall clinical context (20,21).
From a methodological point of view, most of the available studies are observational, retrospective, and have variable sample sizes. Although several meta-analyses support its independent prognostic value, prospective multicenter studies are still needed to validate specific cut-off points and evaluate its real impact on clinical decision-making (22).
Finally, a promising line of research is the integration of the INL into predictive models based on artificial intelligence and machine learning. When combined with clinical, hemodynamic, and biochemical variables, the INL could contribute to automated early warning systems in patients with systemic infection.
In summary, INL represents an accessible, reproducible, and pathophysiologically consistent prognostic marker. Its greatest utility lies in its use as a complementary tool within a comprehensive assessment strategy, rather than as an isolated biomarker.
CONCLUSION
The neutrophil-lymphocyte ratio is an accessible and reproducible inflammatory biomarker with proven prognostic value in multiple systemic infections. Its incorporation into clinical algorithms can improve early risk stratification, especially in resource-limited settings. Future research should establish population-specific cutoff points and validate its integration into standardized prognostic scales.
REFERENCES

Andrea Martinez Garay, Julian Pereañez Martinez, Valentina Leon Monsalvo, Luis Navarro Falx, Natalia Lucia Garrido, Xiomara Fadul Buelvas, Luisa Donado Polo, Lizeth Josa Vela, Andres Arrieta Soto, Usefulness of the Neutrophil-Lymphocyte Ratio as a Prognostic Marker in Systemic Infections, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1476-1482. https://doi.org/10.5281/zenodo.19008207
 10.5281/zenodo.19008207
10.5281/zenodo.19008207
