
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy Practice Sri Adichunchanagiri College of Pharmacy
Background: Saroglitazar is a novel anti-diabetic drug with combined PPAR-?/-? agonistic activity. It was developed domestically by an Indian company called Zydus Cadila in 2001, and after numerous preclinical and clinical trials, it received regulatory approval from the Indian drug controller and regulatory authority called DCGI, India in June 2013. Non-alcoholic Fatty Liver Disease, diabetes, obesity, dyslipidemia, and cardiovascular disease are all grouped together as metabolic syndrome, and these conditions are caused by a sedentary and western lifestyle. Type 2 diabetes mellitus (T2DM) with dyslipidemia and non-alcoholic fatty liver disease (NAFLD) can be treated with this medication, which is marketed under the trade name LipaglynTM. Almost every year, various pharmaceutical companies create thousands of new medications, but nearly all of them fail either in the preclinical or clinical stages. However, Saroglitazar, which was designed, synthesized, and manufactured 20 years ago, became a successful medication with numerous positive effects on patients with type 2 diabetes and metabolic syndrome that no other commercially available medication can match. Another advantage of this medication is that it was the first of the glitazar family to receive permission worldwide, not just in India. We have covered the history of the medication Saroglitazar, which was made in India, in brief in this article.
The prevalence of metabolic syndrome and non-alcoholic fatty liver disease (NAFLD) is rising globally, accounting for 25% to 30% of the total burden. [1] The clinical and economic burden of non-alcoholic fatty liver disease (NAFLD) has increased significantly due to the global obesity epidemic, which is a primary cause of metabolic disorders. [1,2] Obesity, Type 2 DM, CVDs, and NAFLD are all on the rise due to fast food consumption, sedentary work, and the western lifestyle; yet, there are currently no authorized pharmaceutical medications available to treat NAFLD. (3) A low-calorie diet, weight loss, and increased physical activity and exercise are examples of lifestyle modifications that may assist to ameliorate NAFLD and the metabolic syndrome. [2, 3, 4] There aren't many medications on the market to treat CVDs and Type 2 diabetes, however there are one or two approved pharmaceutical medications for NAFLD. [4]
NAFLD -
Patients with non-alcoholic fatty liver disease (NAFLD) or those who do not use large amounts of alcohol should have fat deposition in more than 5% of their hepatocytes. [1] It is a prevalent cause of chronic liver disease that is becoming more widespread and can lead to liver failure and cirrhosis.[1,5] Non-alcoholic steatohepatitis (NASH) and isolated fatty liver are included in the natural history of non-alcoholic fatty liver disease (NAFLD). [5,6] Compared to the general population, isolated fatty liver is not linked to an elevated risk of death and seldom, if ever, develops into cirrhosis. [6] NASH is linked to a higher chance of dying from cirrhosis, cancer, cardiovascular disease, and its aftereffects. [6,7] Diabetes mellitus, severe insulin resistance, elevated BMI, weight increase greater than 5 kg, cigarette smoking, and elevated serum aminotransferase levels are all linked to the progression of fibrosis in NASH. Biopsies are the most effective way to distinguish NASH from isolated fatty liver.[7] However, in clinical practice, ALT and AST levels are utilized to distinguish between NASH and isolated fatty liver; in the former, ALT/AST ratios are normal, while in the latter, ALT>AST levels. 8. About 10–15% of NASH patients that last longer than 15 years progress to cirrhosis. [1, 7].
METABOLIC SYNDROME- is defined as cluster of factors that directly or indirectly increase the risk of cardiovascular diseases and type 2 DM. The main components are dyslipidaemia (increased triglycerides, increased LDL, decreased HDL, increased BP) and dysregulated glucose metabolism, recently abdominal circumference (obese) and insulin resistance have been considered as a core manifestation of the syndrome.[8] One of the main features of metabolic syndrome is its higher incidence in children and young people, as well as its additional effects on the burden of disease worldwide. [8,9] Metabolic syndrome affects roughly 46% of adults worldwide, but it is significantly more common in India, where it affects 25% of adults. [2] The prevalence of metabolic syndrome rises with age; by the age of 60, over half of people have it [9, 10]. 10% of adolescents and 5% of youngsters worldwide suffer from metabolic syndrome. [9] The two main pathophysiological factors of metabolic syndrome are obesity and insulin resistance. Other factors that have been implicated in the pathogenesis include morning stress, dysregulation of the hypothalamic pituitary adrenal axis (HPA) and ANS, an increase in cellular oxidative stress, an increase in the production of glucocorticoids, and the recently identified miRNA (micro-RNA). [11]
Criteria to define metabolic syndrome[12,13]
|
Measure |
Categorical threshold |
|
Waist circumference |
Whites, African Americans, Latin Americans: Men ≥ 

Asians: Men, ≥35 in.;women,≥32 in. 
|
|
Elevated triglycerides |
≥ 150mg/dl or on drug treatment for elevated levels of triglycerides. |
|
Reduce HDL |
Men<40mg/dl; women < 50mg/dl Or on drug treatment for reduced HDL level |
|
Elevated blood pressure |
≥130mm Hg systolic or ≥85 mm Hg diastolic or on antihypertensive drugs |
|
Elevated fasting glucose |
≥100mg/dl Or On drug treatment for elevated glucose level |
|
|
A low-calorie diet, weight loss, and increased physical activity and exercise are examples of lifestyle modifications that may assist to ameliorate NAFLD and the metabolic syndrome. [12,13] The latest developments in Saroglitazar, one of the potentially effective medications to treat Type-2 DM, NAFLD, and metabolic syndrome, are outlined in this article. [14]
APPROACHES IN NOVEL DRUG DESIGN AND DEVELOPMENT-
A recently approved anti-diabetic, anti-fibrotic, anti-inflammatory, and anti-NAFLD medication, saroglitazar is a novel chemical molecule that was first developed domestically by an Indian pharmaceutical company. Since it acts on both PPAR α and γ receptors and activates both receptors in a single hit, it has quickly gained international attention [14,15]. The ligand-activated nuclear receptor family includes PPAR α and γ, which control gene activity by binding to particular DNA sequences and forming a complex with RXR proteins. This α complex can activate or block gene expression depending on the presence of certain molecules. RXRs (α, β, γ) and are activated by 9-cis retinoic acid.[16] While their exact roles in the PPAR – RXR complex are unclear, synthetic RXR activators can mimic PPAR effects and may help in managing type 2 diabetes. [15,16] PPAR – α and γ is widely found in liver cells, intestinal cells, various types of vascular and immune cells, as well as specific brain cells. It plays a vital role in breaking down fatty acids in the liver, supplying energy to different tissues, and increasing fat oxidation in the liver, heart, kidneys, muscles, and brown fat. [15,17]. PPAR α contributes to the management of oxidative stress. These receptors play an important role in glucose metabolism and homeostasis, insulin sensitivity, lipid oxidation and prevent cellular oxidative damage[17].It is important for regulating lipid levels and can help lower abnormal blood fats related to metabolic syndrome. [16,17]
SAROGLITAZAR HISTORY-
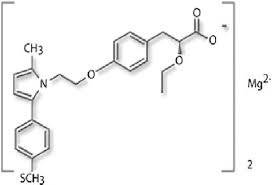
For a once-daily oral dosage of metabolic disorders, such as diabetic dyslipidemia and hypertriglyceridemia, Zydus-Cadila has developed saroglitazar (ZYH-1; Lipaglyn; structure shown), which controls lipid metabolism and is an insulin sensitizer with strong PPAR-alpha agonist activity and comparatively weak PPAR-gamma agonist activity. [18] Additionally, the company has created saroglitazar to potentially treat type II diabetes, lipodystrophy, and non-alcoholic steatohepatitis (NASH). [17, 18]
The ZYDUS company started a research program in 2000, and after numerous preclinical studies, an IND (investigation new drug) was submitted in 2004. The drug was developed and marketed as Lipaglyn® by Zydus Cadila, and in May 2014, a phase III trial for lipodystrophy was started, followed by a phase III study for NASH in January 2015, and in February of the same year, phase III development for type II diabetes was underway [20,21]. In November of 2015, a phase II trial was scheduled in the US. The company's plan to start a phase II trial of saroglitazar in NASH patients was approved by the US FDA in June 2016. [21]
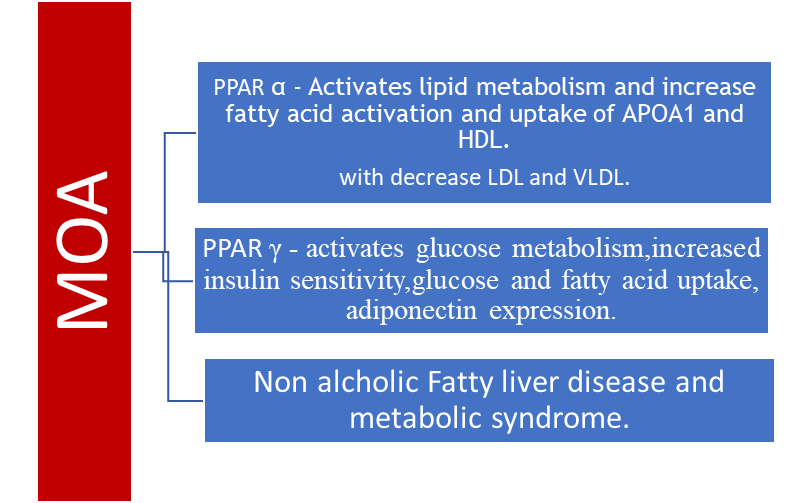
MODE OF ACTION OF SAROGLITAZAR
The new and first medication in the class known as glitazars, saroglitazar, functions as a dual PPAR agonist at the weak agonist γ (gamma) and α (alpha) subtypes of the peroxisome proliferator-activated receptor (PPAR). [19] High blood triglycerides are reduced by agonist action at PPAR α, while insulin resistance is improved and blood sugar is subsequently lowered by agonist action on PPARγ. It is recommended for the management of hypertriglyceridemia and diabetic dyslipidemia in type 2 diabetes mellitus that is not under control with statin therapy. [22] Compared to pioglitazone, the medication lowers HbA1C levels and controls cholesterol levels. The medication has been demonstrated to alleviate hepatocyte steatosis, inflammation, hepatocyte ballooning, and the formation of hepatic fibrosis. It has also been found to improve NAFLD (metabolic associated fatty liver disease) and NASH (metabolic associated steato hepatitis). [22, 23] The first medication for NASH to be licensed globally is presently saroglitazar. [23, 24] Lipaglyn® comes as an oral tablet that contains 4 mg of saroglitazar. 4 milligrams taken orally once a day is the dosage. [24]
Molecular analysis confirmed reduced oxidative stress, unfold protein response and reduced fibro genic signalling.[25] The anti-inflammatory activity of saroglitazar and PPAR target expression were further validated by transcriptomic analysis. Lipidomic study verified that utilizing saroglitazar resulted in decreased triglycerides, diglycerides, sphingomyelin, and ceramides. [25]
DISCUSSION:
Through its PPAR-α and γ agonist effects, saroglitazar, a new dual peroxisome proliferator activated receptor (PPAR) agonist, has improved lipid and glycaemic markers in clinical trials. [19] In 2013, it received marketing permission for diabetic dyslipidemia in India. [18, 19] Dual peroxisome proliferator activated receptor (PPAR) α/γ agonists have garnered international attention as promising new treatment options for diabetic dyslipidemia due to their unique mechanism of action in improving lipid and glucose profile simultaneously. This review was conducted to summarize the effects of Saroglitazar in patients with diabetic dyslipidemia in real world clinical studies conducted after marketing authorization in recent years. [22.23] In patients with diabetic dyslipidemia, PPAR-α agonist action improves the lipid profile while PPAR-γ agonist action improves the glucose profile. [22, 23]
Saroglitazar, a novel dual PPAR α/γ agonist (predominant PPAR-α and moderate PPAR-γ actions), was developed by Zydus with the goal of improving lipid and glucose profiles without causing weight gain or oedema, which are common side effects of PPAR-γ agonists like thiazolidinediones. Many other dual PPAR α/γ agonists were developed but failed during the preclinical or clinical development stages due to lack of efficacy or safety concerns. [18,19] Phase 1 and Phase 2 clinical trials as well as preclinical research showed that saroglitazar had positive effects on glycaemic and lipid markers. In patients with diabetic dyslipidemia, saroglitazar 2 mg and 4 mg significantly decreased TG from baseline to week 24 by 26% and 45%, respectively, in a Phase-3 clinical trial (PRESS V). Saroglitazar 2 mg and 4 mg dramatically decreased TG from baseline to week 12 by 45% in individuals with diabetic dyslipidemia not managed with atorvastatin 10 mg in another Phase-3 clinical trial (PRESS VI). Saroglitazar also improved hyperglycemia and other lipid markers in both Phase 3 clinical studies. [16, 26] In 2013, Saroglitazar received marketing authorization in India after completing successful clinical trials. [26] For almost 40 years, fibrates have been used as lipid-modifying drugs; nevertheless, their potency and selectivity for PPAR-α are low. However, fibrates have been linked to a higher risk of myopathy, cholelithiasis, venous thrombosis, and a deterioration in renal function. Thiazolidinediones, which are structural analogues of fibrates, use PPAR-γ agonists to lower insulin resistance and raise blood glucose levels. [27] On the other hand, peripheral oedema and weight gain have been linked to thiazolidinediones. Furthermore, rosiglitazone has been removed from the European market due to its association with an elevated risk of myocardial infarction. Pioglitazone use has raised concerns around the world since it may increase the risk of bladder cancer and heart failure [27, 28]. The idea of a pan-PPAR/dual-PPAR therapeutic approach for diabetic dyslipidemia was supported by clinical evidence from Bezafibrate, a pan-PPAR [α, β/δ, γ] activator. Over the past 20 years, Glitazars, dual PPAR α/γ agonists, have gained international attention due to their unique lipid and glycemic modifying actions. Several Glitazars, including Muraglitazar, Ragaglitazar, Tesaglitazar, Naveglitazar, Farglitazar, and Aleglitazar, were developed, but failed during the preclinical or clinical development stage due to lack of efficacy or safety issues; the clinical development of Muraglitazar was stopped because of cardiovascular adverse events, such as myocardial infarction, stroke, and heart failure; the clinical development of Aleglitazar was stopped because of cardiovascular AEs, such as heart failure, gastrointestinal bleeding, and renal dysfunction.(29,30) Saroglitazar is the only dual PPAR α/γ agonist (Glitazar) that has been authorized and prescribed for use in clinical settings worldwide. Saroglitazar received marketing permission in Mexico in 2017 after receiving it in India in 2013. The effects of saroglitazar in patients with diabetic dyslipidemia in real-world clinical trials following its 2013 marketing clearance in India are compiled for the first time in this study. [29] Patients with diabetic dyslipidemia with NAFLD were included in three investigations. In the Joshi et al. investigation, transient elastography (Fibro ScanTM) was used to identify NAFLD in 221 patients with diabetic dyslipidemia. They discovered that Saroglitazar improved fatty liver (as determined by transient elastography (Fibro ScanTM)) in 39% (86/221) of patients and significantly decreased TG (baseline: 321.0 mg/dL to week-24: 129.0 mg/dL) and ALT (baseline: 89.0 IU/L to week-24: 21.0 IU/L). Likewise, Saboo et al. found that in 31 NAFLD patients with diabetic dyslipidemia, saroglitazar significantly reduced ALT (baseline: 64.1 ± 6.2 IU/L to week-24: 28.7 ± 3.2 IU/L) and TG (baseline: 259.3 ± 37.9 mg/dL to week-24: 151.5 ± 53.6 mg/dL). Additionally, Goyal et al. discovered that Saroglitazar substantially reduced ALT (baseline: 98.0 ± 32.0 IU/L to week-24: 34.0 ± 14.0 IU/L) and TG (baseline: 334.7 ± 74.0 mg/dL to week-24: 158.5 ± 46.0 mg/dL) in 84 patients with diabetic dyslipidemia (78.5% of these 84 patients were diagnosed with NAFLD by transient elastography (FibroScan™). [24].
The most common side effects (≥2% of patients) associated with using Saroglitazar 4 mg in phase-3 clinical trials were asthenia, gastritis, dizziness, and tremors in the PRESS V study, and gastritis and pain in the PRESS VI study. Saroglitazar was also found effective in lowering ALT and improving fatty liver (evaluated by sonographic (FibroScan™) investigation) in NAFLD patients with diabetic dyslipidemia. These results are also supported by a preclinical study conducted by Jain et al. [. In experimental non-alcoholic steatohepatitis (NASH) model (animal model of mice with choline-deficient high-fat diet-induced NASH), the authors found that Saroglitazar reduced ALT, hepatic steatosis, inflammation, ballooning, and prevented fibrosis development at present, there are no medications approved for NAFLD/NASH. Saroglitazar could become a promising treatment option for NAFLD/NASH. However, the efficacy and safety of Saroglitazar in patients with NAFLD/NASH must be examined in RCTs. [30,31,32]
CONCLUSION-
Saroglitazar is a dual PPAR ? + γ agonist that reduces elevated TG, HbA1c, and stiffness of the liver as reflected by the reduction in the SWE (Shear wave elastography) score of the liver. This indicates that Saroglitazar is a dual agonist with triple benefits.[31] Saroglitazar is a novel drug, with unique mechanism of action, which has established its efficacy and safety in diabetic dyslipidemia in clinical trials. It not only corrects lipid abnormalities, but also helps to achieve glycaemic targets in T2DM. Use of saroglitazar will help clinicians to better manage metabolic abnormalities in T2DM patients. [31,32,33] Now, Saroglitazar is a huge successful drug not only for diabetes mellitus also for the obesity associated with Non-alcoholic Fatty liver disease patients. Treatment with 4 mg saroglitazar could significantly improve liver enzymes, reduce liver stiffness, and improve metabolic parameters (serum glucose and lipid profile) in patients with NAFLD or NASH.[31,32,33,34].
REFERENCES



Varsha*, Robin George, Shashank D., Saroglitazar's Therapeutic Use in Metabolic Syndrome and Nafld, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 3200-3207. https://doi.org/10.5281/zenodo.15111106
 10.5281/zenodo.15111106
10.5281/zenodo.15111106