K.E. Society's Rajarambapu College of Pharmacy Kasegaon.
Thyroid diseases are common worldwide. In India too, there is a significant burden of thyroid diseases. According to a projection from various studies on thyroid disease, it has been estimated that about 42 million people in India suffer from thyroid diseases. This review will focus on the epidemiology of five common thyroid diseases in India: hyperthyroidism, (goiter and iodine deficiency disorders, Hashimoto's thyroiditis, and thyroid cancer. Thyroid disorders are among the most common diseases of the endocrine system and may be divided into the groups of hypothyroidism, hyperthyroidism, and thyroid nodules/cancer. Hypothyroidism is usually due to surgical thyroidectomy or autoimmune destruction of the gland; it is reliably diagnosed and monitored through measures of thyroid-stimulating hormone (TSH). Hyperthyroidism is commonly caused by auto-antibody driven thyroid hormone over-production or excessive thyroid secretion by a functional thyroid nodule. Hyperthyroidism is diagnosed and managed through use of TSH, free thyroxine, and free tri-iodothyronine measures. Severe thyroid auto-antibodies may be measured but are specific to the disease in question. Thyroglobulin and calcitonin are two common biochemical tumor markers useful in the follow up of thyroid cancer.
Thyroid diseases are, arguably, among the commonest endocrine disorders worldwide. India too, is no exception. According to a projection from various studies on thyroid disease, it has been estimated that about 42 million people in India suffer from thyroid diseases. (1) Thyroid diseases are different from other diseases in terms of their ease of diagnosis, accessibility of medical treatment, and the relative visibility that even a small swelling of the thyroid offers to the treating physician. Early this diagnosis and treatment remains the cornerstone of management. Thyroid disorders affect a substantial proportion of the general population, but most have a remarkably higher incidence in women. Worldwide, the most common cause of thyroid disorders is iodine deficiency. Although eradicated in many parts of the world, it is still a major health problem affecting almost a third of the world's population. About twenty million people are believed to be significantly mentally handicapped as a result of iodine deficiency. In iodine-sufficient regions, the autoimmune thyroid diseases, Hashimoto's thyroiditis and Graves’ disease are the most common clinical entities affecting the thyroid. The prevalence of thyroid disorders depends on the diagnostic criteria used and the surveyed population's age and sex. The prevalence of overt hypothyroidism is ∼ 3–20 per 1000 females and ∼ 1–7 per 1000 males. The most common cause of hypothyroidism is Hashimoto's thyroiditis. The prevalence of hyperthyroidism is ∼ 2–19 per 1000 females and ∼ 1–2 per 1000 males. Graves’ disease is its most frequent cause. The differences in the prevalence of hypo- and hyperthyroidism in men and women are most commonly explained by influences of sex steroids on immune regulatory mechanisms. Thyroid carcinomas are relatively rare neoplasms that account for 0.6–1.6% of all malignancies. The annual incidence of papillary, follicular, and differentiated thyroid carcinomas cancer is 1–10 per 100,000 people. They are about three times more common in women than men. (2) The thyroid hormone axis is an endocrine system with many important actions, including growth and development. As a result, the thyroid hormone axis is also a potential cause of myriad signs and symptoms. Thyroid function is routinely checked as part of the annual physical examination despite the lack of clinical evidence for this practice and the resultant increase in health-care costs. Concern for thyroid dysfunction is one of the most common reasons for referral to apediatric endocrinologist. As with other endocrine measures, age and clinical status strongly influence what are considered normal values with testing .Although thyroid dysfunction. (2) Problems with the thyroid gland are extremely common. It has been estimated that as many as one and a half billion people in the world are at risk for thyroid problems. Hypo-thyroidism the most common thyroid malfuntion but it is possible to have hyperactive thyroid gland. Subclinical hypo-thyroidism is also an important condition, affecting upto20 % of persons beyond 60 years of age. (3).
Literature Review:
The thyroid gland consists of two lobe connected by a thin isthmus, usually located below and anterior to the larynx. Each lobe is divided into lobules, each containing 20 to 40 evenly dispersed follicles. The follicles are lined by cuboidal to low columnar epithelial cells that synthesize thyroglobulin, the iodinated precursor protein active thyroid hormone. Thyroglobulin is stored in the lumen of follicles as a homogeneous suspension called colloid. In response to trophic factors from the hypothalamus, TSH (also called thyrotropin) is released by thyrotrophs in the anterior pituitary into the circulation. TSH binds to its receptor on thyroid follicular epithelial cells, activating a stimulatory G-protein, and this signaling pathway induces the synthesis and release of thyroid hormone. (4)
The thyroid is a butterfly-shaped gland located in the front of the neck just above the trachea. It weighs approximately 15 to 20 grams in the adult human. The thyroid gland is divided into two lobes connected by the isthmus, which crosses the midline of the upper trachea at the second and third tracheal rings. In its anatomic position, the thyroid gland lies posterior to the sternothyroid and sternohyoid muscles, wrapping around the cricoid cartilage and tracheal rings. It is located inferior to the laryngeal thyroid cartilage, typically corresponding to the vertebral levels C5-T1. The thyroid attaches to the trachea via a consolidation of connective tissue, referred to as the lateral suspensory ligament or Berry’s ligament. This ligament connects each of the thyroid lobes to the trachea. The thyroid gland, along with the esophagus, pharynx, and trachea, is found within the visceral compartment of the neck, which is bound by pre tracheal fascia.(5) The thyroid gland, anterior pituitary gland, and hypothalamus comprise a self-regulatory circuit called the hypothalamic-pituitary-thyroid axis. The main hormones produced by the thyroid gland are thyroxine or tetraiodothyronine (T4) and triiodothyronine (T3). Thyrotropin-releasing hormone (TRH) from the hypothalamus, thyroid-stimulating hormone (TSH) from the anterior pituitary gland, and T4 work in synchronous harmony to maintain proper feedback mechanisms and homeostasis. Hypothyroidism, caused by an underactive thyroid gland, typically manifests as bradycardia, cold intolerance, constipation, fatigue, and weight gain. In contrast, hyperthyroidism caused by increased thyroid gland function manifests as weight loss, heat intolerance, diarrhea, fine tremor, and muscle weakness. (6) Regulation of thyroid hormone starts at the hypothalamus. The hypothalamus releases thyrotropin-releasing hormone (TRH) into the hypothalamic-hypophyseal portal system to the anterior pituitary gland. TRH stimulates thyrotropin cells in the anterior pituitary to release thyroid-stimulating hormone (TSH). TRH is a peptide hormone created by the cell bodies in the periventricular nucleus (PVN) of the hypothalamus. These cell bodies project their neurosecretory neurons down to the hypophyseal portal circulation, where TRH can concentrate before reaching the anterior pituitary. (6)
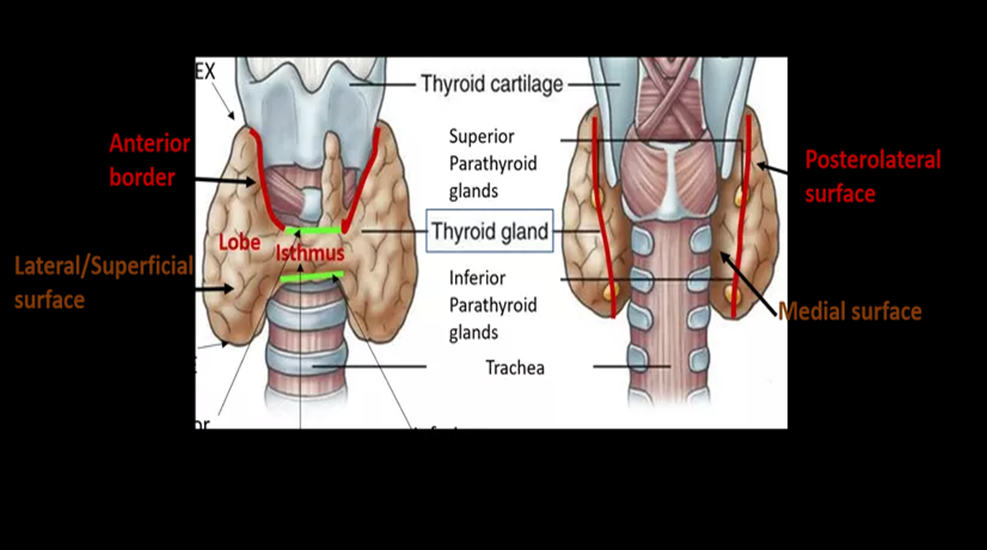
Fig (1). Anatomy of thyroid gland (7)
The thyroid hormoes are synthesized and stored in the thyroid follicles as part of thyroglobulin molecule—which is a glycoprotein synthesized by thyroid cells, MW 660 KDa, contains 10% sugar. The synthesis, storage and release of T4 and T3 is summarized in Fig. (2) and involves the following processes.
(1) Inorganic iodide is transported into the gland
(2) Intra thyroidal iodide is oxidized to iodine under the influence of h2o2 and peroxidase
(3) Iodine is bound in thyroglobulin to tyrosine, forming monoiodotyrosine and diiodotyrosine
(4) Iodotyrosines are enzymatically coupled to form thyroxine (t4) and triiodothyronine (t3)
(5) Iodothyronines, t4 and t3, are stored in thyroglobulin until released into the circulation; and
(6) Unused iodotyrosines are deiodinated and the iodide is recycled.
1. Iodide Uptake
The total body content of I2, obtained from food and water, is 30–50 mg, out of which about 1/5 is present in the thyroid. Concentration of iodide in blood is low (0.2–0.4 μg/dl) but thyroid cells have an active transport process (Na+: I¯ symporter or NIS) to concentrate this anion; this trapping is stimulated by TSH to exceed a gradient of more than 100 fold. The I2 content of thyroid gland somehow regulates the uptake mechanism: meagre store activating and large store inhibiting it. The iodide concentrating mechanism is not peculiar to thyroid; skin, salivary glands, gastric mucosa, intestine, mammary glands and placenta also possess it, but uptake in these organs is not stimulated by TSH.
2. Oxidation And Iodination
Iodide trapped by follicular cells is carried across the apical membrane by another transporter termed ‘pendrin’ and oxidized by the membrane bound thyroid peroxidase enzyme to iodinium (I+) ions or hypoiodous acid (HOI) or enzyme linked hypoiodate (EOI) with the help of H2O2. These forms of iodine combine avidly with tyrosil residues of thyroglobulin, apparently without any enzymatic intervention, to form monoiodotyrosine (MIT) and diiodotyrosine (DIT) while the residues are still attached to the thyroglobulin chains.
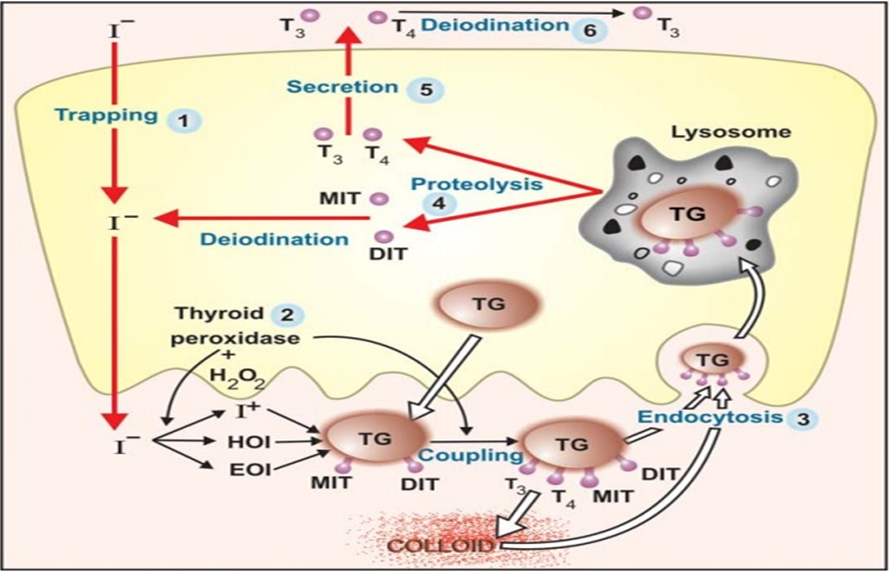
Fig. (2) Synthesis, storage and secretion of thyroid hormone (9)
3. Coupling
Pairs of iodinated tyrosil residues couple together (Fig. 18.2) to form T3 and T4. Normally much more T4 than T3 is formed, but during I2 deficiency relatively more MIT is available and a greater proportion of T3 is formed. Thus, more active hormone is generated with lesser amount of I2.Coupling is an oxidative reaction and is catalysed by the same thyroid peroxidase. Thyroglobulin is the most efficient protein in supporting coupling by providing favourable spatial configuration to facilitate the reaction. Oxidation of iodide and coupling are both stimulated by TSH.
4. Storage and Release
Thyroglobulin containing iodinated tyrosil and thyronil residues is transported to the interior of the follicles and remains stored as thyroid colloid till it is taken back into the cells by endocytosis and broken down by lysosomal proteases. The T4 and T3 so released is secreted into circulation while MIT and DIT residues are de-iodinated and the iodide released is reutilized. The uptake of colloid and proteolysis are stimulated by TSH: the quiscent gland has follicles distended with colloid and cells are flat or cubical, while the TSH stimulated gland has columnar cells and colloid virtually disappears. Normal human thyroid secretes 60-90 µg of T4 and 10-30 µg of T3 daily.
5. Peripheral Conversion of T4 To T3
Peripheral tissues, especially liver and kidney, convert T4 to T3. About 1/3 of T4 secreted by thyroid undergoes this change and most of the T3 in plasma is derived from liver. Target tissues take up T3 from circulation for their metabolic need, except brain and pituitary which take up T4 and convert it to T3 within their own cells. Almost equal amounts of 3, 5, 3' triiodothyronine (normal T3: active) and 3, 3?, 5′ triiodothyronine (reverse T3: inactive) are produced in the periphery. Propylthiouracil (but not carbimazole), propranolol (high doses), amiodarone and glucocorticoids inhibit peripheral conversion of T4 to T3 (except in brain and pituitary).
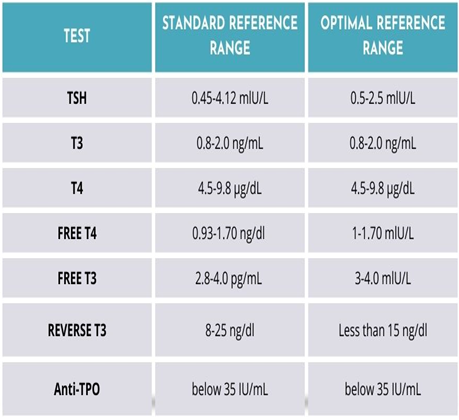
Fig. (3) Normal Ranges of thyroid functioning test (9)
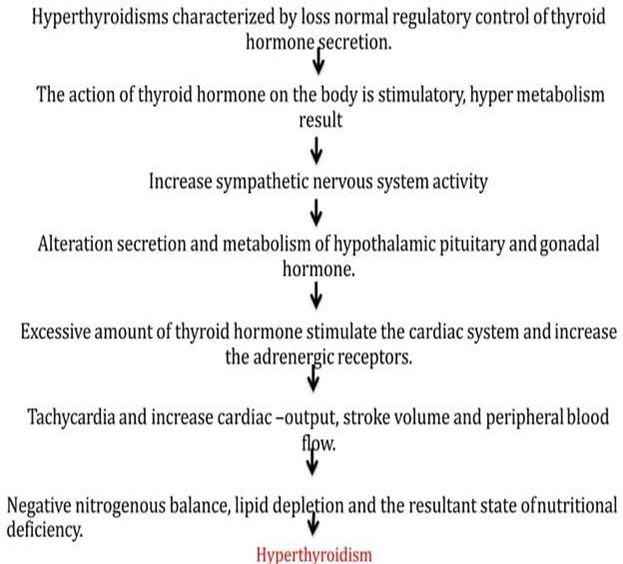
Flow chart (1) of Pathophysiology of Thyroid (10)
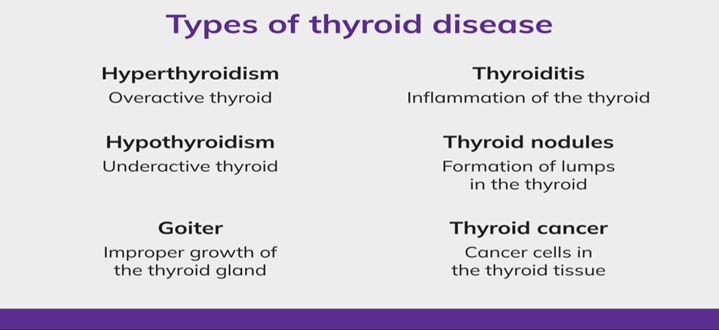
Fig. (4) Types of thyroid diseases (11)
Hypothyroidism
Hypothyroidism is a disorder that occurs when the thyroid gland does not make enough thyroid hormone to meet the body’s needs. Thyroid hormone regulates metabolism—the way the body uses energy and affects nearly every organ in the body. Without enough thyroid hormone, many of the body’s functions slow down. About 4.6 percent of the U.S. population age 12 and older has hypothyroidism. (12) Among the various varieties of hypothyroidism, congenital hypothyroidism is probably the most important, as it is requires an early diagnosis, which is usually followed by appropriate therapy that can prevent the onset of brain damage. Studies from Mumbai have suggested that congenital hypothyroidism is common in India, the disease occurring in 1 out of 2640 neonates, when compared with the worldwide average value of 1 in 3800 subjects. There is often a delay in the diagnosis of congenital hypothyroidism in the country. This delay is attributable to the lack of awareness about the illness, as well as the lack of facilities available or screening program in placeto comprehensively screen and test newborns for this illness. In childhood too, hypothyroidism can occur. In a clinic-based study from Mumbai, out of 800 children with thyroid disease, 79% had hypothyroidism. Common causes of hypothyroidism in these children were thyroid dysgenesis, dyshormonogenesis, and thyroiditis. (1) Among adult people in India, the prevalence of hypothyroidism has been recently studied. In this population base study done in Cochin on 971 adult subjects, the prevalence of hypothyroidism was 3.9%. The prevalence of subclinical hypothyroidism was also high in this study, the value being 9.4%. In women, the prevalence was higher, at 11.4%, when compared with men, in whom the prevalence was 6.2%. The prevalence of subclinical hypothyroidism increased with age. About 53% of subjects with subclinical hypothyroidism were positive for anti-TPO antibodies. This was a population-based study, which used cluster sampling strategy. In this study, Urinary Iodine Status was studied in 954 subjects from the same population sampled, and the median value was 211μg/l. (1)
Hyperthyroidism, also called overactive thyroid, is when the thyroid gland makes more thyroid hormones than your body needs. The thyroid is a small, butterfly-shaped gland in the front of our neck. Thyroid hormones control the way the body uses energy, so they affect nearly every organ in our body, even the way your heart beats. With too much thyroid hormone, many of your body’s functions speed up. (1). The prevalence of hyperthyroidism has been studied in several studies. In an epidemiological study from Cochin, subclinical and overt hyperthyroidism were present in 1.6% and 1.3% of subjects participating in a community survey. In a hospital-based study of women from Pondicherry, subclinical and overt hyperthyroidism were present in 0.6% and 1.2% of subjects.[4] More than a third of community-detected hyperthyroid cases have positive anti-TPO antibodies, and about39% of these subjects are goiter. (1).
Fig. (5) Hyperthyroidism and Hypothyroidism (13)
Goiter means enlargement of the thyroid gland and is a general term that conveys the information that the volume of the thyroid gland is larger than normal. The presence of goiter can be determined by inspection, palpation, or by an imaging study. Normal thyroid gland measures 4 to 4.8 cm in sagittal, 1 to 1.8 cm in transverse, and 0.8 to 1.6 cm in anteroposterior dimensions. This corresponds to a volume of 7 to 10 mL on ultrasonography calculations and 10-20 grams in weight. Thyroid size increases with age and body size. It is larger in males as opposed to females. The size decreases with higher iodine intake.
A thyroid nodule is a lump in or on the thyroid gland. Thyroid nodules are detected in about 6 percent of women and 1-2 percent of men; they occur 10 times as often in older individuals, but are usually not diagnosed. Any time a lump is discovered in thyroid tissue, the possibility of malignancy (cancer) must be considered. More than 95 percent of thyroid nodules are benign (noncancerous), but tests are needed to determine if a nodule is cancerous. (15)
Most thyroid cancers are differentiated cancers. The cells in these cancers look a lot like normal thyroid tissue when seen in the lab. These cancers develop from thyroid follicular cells.
Conditions that can cause hypothyroidism include:
Sometimes, the thyroid gland doesn’t work correctly from birth. This affects about 1 in 4,000 newborns. If left untreated, the child could have both physical and mental issues in the future. All newborns are given a screening blood test in the hospital to check their thyroid function (16).
Conditions that can cause hyperthyroidism include:
1. Graves’ Disease: In this condition the entire thyroid gland might be overactive and produce too much hormone .This problem is also called diffuse toxic goiter (enlarged thyroid gland).
2. Nodules: Hyperthyroidism can be caused by nodules that are overactive within the thyroid. A single nodule is called toxic autonomously functioning thyroid nodule, while a gland with several nodules is called a toxic multi-nodular goiter.
3. Thyroiditis: This disorder can be either painfull or not felt at all .In thyroiditis ,the thyroid releases hormones that were stored there .This can last for a few weeks or onths.
4. Excessive Iodine: When you have too much iodine (the mineral that is used to make thyroid hormones) in your body, the thyroid makes more thyroid hormones than it needs. Excessive iodine can be found in some medications (amiodarone, a heart medication) (15)
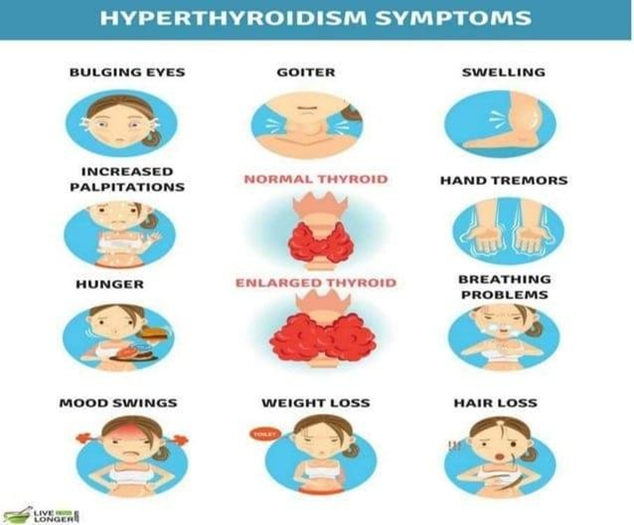
Fig. (6) Symptoms of Hyperthyroidism (15)
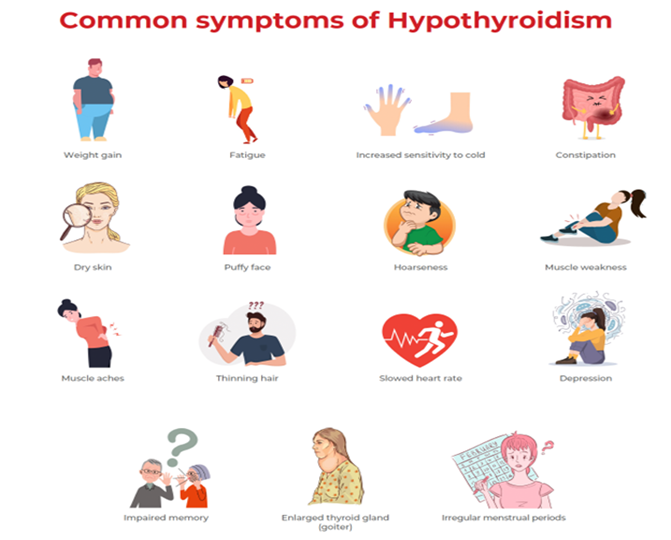
Fig. (7) Symptoms ofHypothyroidism (15)
Hypothyroidism is a hypo-metabolic state that results from a deficiency in T4 and T3. Its major clinical manifestations are fatigue, lethargy, cold intolerance, slowed speech and intellectual function, slowed reflexes, hair loss, dry skin, weight gain, and constipation. It is more prevalent in women than men. The most common cause of hypothyroidism is disease of the thyroid itself primary hypothyroidism. The most common cause of primary hypothyroidism is chronic autoimmune thyroiditis (Hashimoto's disease), in which the thyroid is destroyed by antibodies or lymphocytes that attack the gland. Other causes are radioactive iodine and surgical therapy for hyperthyroidism or thyroid cancer, thyroid inflammatory disease, iodine deficiency, and several drugs that interfere with the synthesis or availability of thyroid hormone. Hypothyroidism may also occur rarely (<1percent of cases) as a result of deficiency of TRH or impaired TSH secretion due to hypothalamic or pituitary disease, respectively.
The most common cause of hyperthyroidism is Graves' disease, an autoimmune disease characterized by the production of antibodies that activate the TSH receptor, resulting in stimulation of T4 and T3 production and enlargement of the thyroid. Other caused of hyperthyroidism area multinodular goiter, solitary thyroid adenoma, thyroiditis, iodide-or drug-induced hyperthyroidism, and, very rarely, a TSH secreting pituitary tumor. The diagnosis of hyperthyroidism is based on the findings of a high serum free T4 level and a low serum TSH concentration. Occasionally, people with hyperthyroidism have a normal serum free T4 and high serum free T3 concentrations. These patients have what is called T3-hyperthyroidism. An increase in serum thyroid hormone binding protein will raise the serum total T4 level but not free T4 concentrations. In these patients the serum TSH remains normal. Patients with a low serum TSH concentration and normal serum free T4 and free T3 levels have, by definition, subclinical hyperthyroidism. (13-13/01/2024)
Screening can be defined as “the application of a test to detect a potential disease or condition in a person who has no known signs or symptoms of that condition at the time the test is done.” By this definition, screening with thyroid function tests may identify asymptomatic individuals as well as patients who have mild, nonspecific symptoms such as cold intolerance or feeling. When many of these symptoms and signs occur together, the clinician may have a strong suspicion that the patient has thyroid disease. However, patients who complain of one or two of the symptoms in may be no more likely to have abnormal thyroid function tests than those who have no complaints. In older patients 7and in pregnant women, such symptoms are so common that it becomes meaningless to try to distinguish between “asymptomatic” patients and those who have symptoms that may or may not be related to thyroid state. (16)
A. Blood test
Tests for thyroid include blood tests to assess thyroid function. They primarily include the following:
1) TSH: It is one of the most useful tests for assessing thyroid function. Over past few years, three generation of assay tests have come up. All the 3 generation assays can pick up elevated levels of TSH and hence aid in diagnosing primary hypothyroidism (low thyroid hormones due to thyroid gland disease).Second generation immunemetric assays for TSH have detection limits of 0.1mU/Landarehelpfulinscreeningforhyperthyroidism.Thirdgenerationchemiluminescentassays (with detection limits of0.01 m U/L) can distinguish more accurately between hyperthyroidism and hypothyroidism. Normal level so TSH are* 0.4- 4.2mu*U /L.
2) Serum T3, and T4 levels are estimated by radioimmunoassay (RIA), or immunometric techniques like chemiluminescence. Normal levels of T3:70-204ng/dl Normal levels of T4:6-11µg/dl More than 99.9% of thyroid hormones are bound to proteins but it is only the free hormone that is the active form. Hence assays have been developed to measure free T_{y} and free T, hormones.
The normal levels of free T.: 210 - 440pg / d l The normal levels of free T?: 0.8 - 2.7ng / dl
3) Thyroglobulin:
Thyroglobulin levels can be estimated as part of thyroid function tests along with T y 'T_{4} and TSH levels. It is synthesised by the follicular cells thyroid gland and its levels increase in the blood benign or malignant tumors of the thyroid gland.
4) Autoimmune markers:
Tests for TSH receptor antibodies (TRAB, TSH-Ab) can detect both types of antibodies-stimulatory as well as those blocking the TSH receptor. In Graves' disease both stimulating and blocking antibody assays will be positive in more than 70% patients. Chronic lymphocytic thyroiditis (Hashimoto's thyroiditis) is characterized by production of antibodies which lead to decreased production of thyroid hormone by the gland. The thyroidperoxidase (TPO) antibody is seen in more than 80% of these patients. Another test involves the measurement of antibodies produced against thyroglobuline
B. Tests-based on use of Nuclear Medicine
Radioactive iodine (RAI) uptake studies by the thyroid gland are assessed along with measurement of TSH levels. In Graves' disease, the uptake is high in spite of very low or undetectable TSH levels. In cases of subacute thyroiditis, the RAI uptake is low along with undetectableTSH.Technetiumpertechnetateorradioactiveiodinescanningcanbeusedtodetect"hot" nodules (not likely to be cancerous) or "cold" nodules which can be cancerous though some dare benign . Radioactive scanning also helps to detect thyroid metastasis or ectopic thyroid tissue. The perchlorate discharge test can be used to pick up defective iodide oxidation or defects in iodination of thyroglobuline.
C. Thyroid Ultrasound
This can pick up very small nodules that may not be picked up clinically.
D. Fine Needle Aspiration Biopsy
This is helpful in assessment of thyroid nodules. It can help in diagnosing and early treatment of thyroid malignancies, while at the same time helps avoid unnecessary surgery in patients with Benign nodules Ultrasound imaging can be used to assist biopsy in cases of nodules that are not palpable.
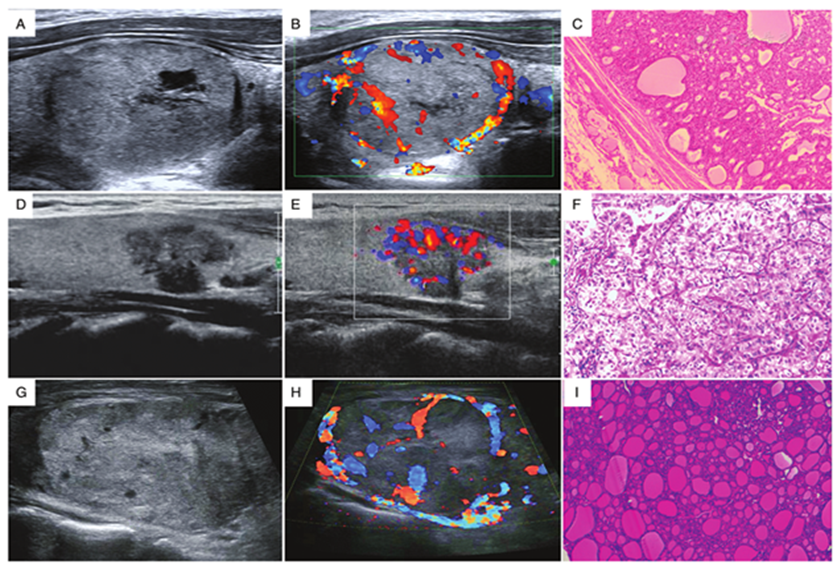
Fig (7). Thyroid Ultrasound (17)
E. Thyrotropin Releasing Hormone (TRH) Response Test
The patient if administered with thyrotropin releasing hormone, and the variation in secretion of TSH, T3, and T4 is observed (the normal response is increased TSH, TyT1 secretion with increased T3, T4, levels). In patients of hypopituitarism in which pituitary response to TRH is deranged, it leads to abnormal 'thyrotropin releasing hormone test' results. Similarly, the physiological response of TRH (i.e. increased TSH and thereby Ty T?) does not occur and is attributed to the fact that the negative feedback effect of high levels of T, overrides the stimulatory physiological response of TRH.
Classification of thyroid inhibitors
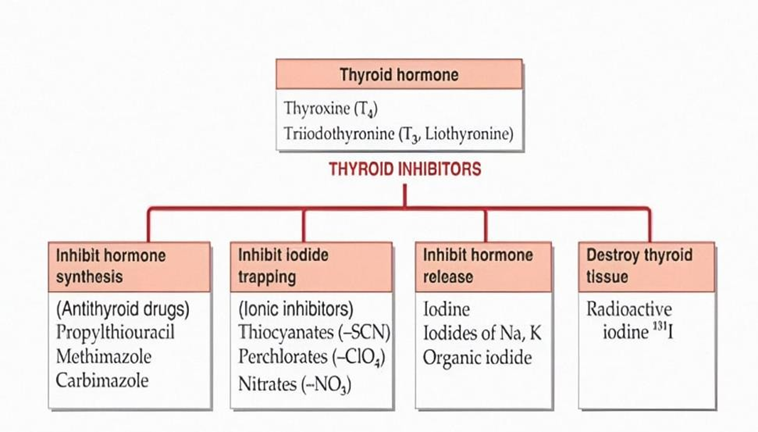
Fig. (8) Classification of Antithyroid Drugs (18)
A) Antithyroid drugs: (Thioamides)
Hormone synthesis inhibitors called Anti-thyroid drugs.
Mechanism of action:
Thiocarbamide (S-C-N) group essential for activity. Antithyroid drugs bind to thyroid peroxidase and prevent oxidation of iodide/iodotyrosyl residues;
1)Inhibit iodination of tyrosine residues in thyroglobuline.
2) Inhibit coupling of iodotyrosine residues to form T3 and T4 which occurs as low concentration.
Simply this class drug decreases the output of thyroid hormone from the gland so decreases the sign and symptoms of thyrotoxicosis. Propyl Thiouracil- Inhibit conversion of T4-T3- Mostly in type 1st diabetes mellitus- but metamizole & Carbamazole not have this action.
B) Iodine/Iodide
Even if the iodine is one of the constitute of thyroid hormone but still it acts as faster acting thyroid inhibitor (Antithyroid). In the process of thyroid hormone release in one step iodine is covered in to on vivo iodide (1-) and due to negative feedback mechanism iodide inhibit release of thyroid hormone. Within 1-2 days of starting of treatment causes inhibition of secretion of thyroid hormone while 10-14 days causes marked reduction in vascularity of gland & which causes decreases the size of gland. Iodine mostly orally in solution with potassium Iodide (Lugols iodine).Effect seen in 15-15 days. But further treatment causes thyroid escape & thyrotoxicosis or hyperthyroidism mostly occurs in multinodular goiter.
Mechanism of action:
Actual mechanism is unknown; It inhibits own transport in to thyroid cell (Step 1 in thyroid synthesis) by acting on NIS (Sodium Iodide symporter) It attenuates TSH & cAMP & causes thyroid inhibition. Also excess iodide rapidly interferes with tyrosil (lodination step2) Inhibit thyroid (Wolff chaikoff effect) Inhibition of hormone release causes thyroid constipation.
C) Radioactive Iodine:
Ex-II31, II23 ,II25.
The stable form of isotope of iodine is II 27 but medically useful isotope is I I31 which having half-life 8 days available as sodium salt; given as oral dose. But one of the advantages of radioactive iodine is it produce necrosis of cell (affected thyroid follicular cell) without damaging neighboring tissue Radioactive iodine administration as sodium salt of 1 131 dissolve in water & take orally.
Diagnostic:25-100µg given scanning is done at interval (No damage to thyroid cell occurs with this dose).
Mechanism of Action:
Isotope emits both beta (β) & gama (8) radiation. Beta Have shorter range. Penetrate tissue (up to 0.5-2 mm) Pyknosis & necrosis with fibrosis and gama Pass through tissue without damage.
D) B- Adrenergic blocker:
Nonselective B blockers- propranolol used for treatment of thyrotoxicosis because in hyperthyroidism activity of sympathetic nervous system was observed i.e. palpitation, tremor, nervousness, myopath, swelling.Very little effect on thyroid function & hyper metabolic state.B blockers used for tretment of hyperthyroidism in following situation;
1) While response to carbimazole, propylthiouracil orII31 is low. 2) B blockers given along with iodide for preoperative preparation before subtotal thyroidectomy. 3) Thyroid storm (thyrotoxic crisis-It is an emergency due to decompensate hyperthyroidism.) In above condition emergency treatment with B blockers are given.
2. Radioactive iodine
Administered as sodium salt of dissolved in water & taken orally.
3. Ionic inhibitors
4. β-Blockers
Findings and analysis (21)
Many people are raising awareness about the thyroid gland. Yes, you’ve heard of it, but can you tell exactly where it is and what it does? The condition of your thyroid affects various critical body functions. But surprisingly, up to 60% of people with thyroid dysfunction are completely unaware of their condition. Thyroid abnormalities are also becoming more closely linked to an increased risk of acquiring other ailments. Examples of these are:
• Metabolic syndrome
• Cardiovascular disease
• Obesity
• Renal disease
• Depression
Lifestyle Habits That Can Change to Keep Thyroid Healthy
Poor Sleeping Pattern
Sleeping well has a direct impact on your mental and physical well-being. If you don’t get enough sleep, it may negatively affect your energy, productivity, emotional balance, and even weight. Sleep and your circadian components are fundamental to achieving optimum thyroid functions. Sleeping patterns may influence your susceptibility to illnesses. According to one study, those who get less sleep—less than seven hours—are more likely to develop hyperthyroidism. Those who sleep more than eight hours may be more susceptible to overactive and underactive thyroid function.Sleep also keeps cortisol, the stress hormone, in check. Additionally, getting enough sleep helps maintain a strong immune system. Thyroid dysfunction is more likely to occur in persons with weakened immune systems. To sleep better, stay away from bright screens 1-2 hours before bedtime. Regular exercise, avoiding caffeine, and deep breathwork can help you relax more. Setting up a healthy sleeping environment in a comfortable way enables you to stay asleep for more extended periods of time. Keeping it cool and dark will also make your brain secrete more melatonin to make you fall asleep faster.
Unhealthy Eating Habits
Foods with low nutritional value are one of the primary root causes of thyroid disorders since it is a nutrient-dependent gland. And the deficiency in these nutrients will negatively affect thyroid hormone production. A well-balanced diet is essential for lifelong thyroid health. You can achieve this by increasing your intake of the following:
Sedentary Lifestyle
A sedentary lifestyle with low physical movement results in people having low thyroxine. Take note that it’s the hormone responsible for essential body functions like heart rate and energy levels. The lack of physical activity is unhealthy and puts people at risk of an underactive thyroid.
Several benefits of regular exercise include:
Smoking
Every single organ system in the body is affected by the consequences of cigarette smoking. The thyroid gland also suffers just as much as the lungs and heart from the damaging effects of tobacco.Tobacco smoke includes chemicals affecting the thyroid gland’s function and the thyroid gland itself. Tobacco contains cyanide, which, when smoked, transforms into the chemical thiocyanate. Thiocyanate hinders the absorption of iodine, reducing the production of hormones T4 and T3. It causes a rise in iodine excretion from the kidneys. This raises the risk of inflammation of the thyroid gland and has constitutional symptoms, including fever, nausea, and stomach discomfort. The apparent benefits of smoking pales in comparison to the advantages quitting. Because the bottom line remains—smoking won’t do anything but exacerbate thyroid symptoms, speed up the progression of thyroid illness, and reduce the efficiency of thyroid treatment.
CONCLUSION:
The thyroid gland maintains the level of metabolism in the tissues that is optimal for their normal function. Thyroid hormone stimulates the O2 consumption of most of the cells in the body, regulates lipid and carbohydrate metabolism, and is also necessary for normal growth and maturation. The main function of the gland is to synthesize and secrete the thyroid hormones, namely, thyroxine (T4), triiodothyronine (T3) and calcetonine. The thyroid gland plays an important role in the normal metabolic rate and that is why a precise control system is operating to provide the right amounts of thyroid hormones at different conditions, both suprathyroid and autoregulatory mechanisms are involved in this control system. The secretion of thyrotropin (TSH), which is the major modulator of thyroid function, is regulated at the level of the pituitary thyrotroph by the antagonistic effects of thyroid hormones and the TSH releasing hormone (TRH), the former inhibits and the latter stimulates the synthesis and secretion of (TSH ). Therefore, excess thyroid hormone leads to decreased secretion of (TSH), and thyroid hormone insufficiency is associated with (TSH) hypersecretion, TSH stimulates all steps of thyroid hormone synthesis and secretion. Ischemic heart disease is defined by world health organization as : myocardial impairment due to imbalance between coronary blood flow and myocardial requirement, caused by changes in the coronary circulation. In the last 20 years, epidemiolgic and experimental studies have provided considerable evidence linking certain risk factors for coronaryatherosclerotic heart disease (CAHD), among many factors that have been shown to be important as risk factors of ischemic heart disease are hyperlipidemia, hypertension, cigarette smoking, sex, obesity, psychosocial tension, and diabetes mellitus. When risk factors coexist, they multiply the risk of chronic atherosclerotic heart disease (CAHD). The most frequently recognized cause of myocardial ischemia is occlusive coronary artery atherosclerosis, which either causes direct arterial narrowing or thrombous formation. Patients with ischemic heart disease fall into two large groups: patients with stable angina secondary to chronic coronary artery disease and patients with acute coronary syndromes (ACS). The latter group, in turn, is composed of patients with acute myocardial infarction (MI) with ST-segment elevation on their presenting electrocardiogram and those with unstable angina (UA) and non ST- segment elevation MI (UA/NSTEMI). The cardiovascular system is one of the most important targets on which thyroid hormones act. More than 80% of the biologically activehormone T3 derives from peripheral conversion of T4 secreted by the thyroid gland. Clinical and experimental evidence has shown that T3 play a major role in modulating heart rate and cardiac contractility as well as arterial peripheral resistance. T3 actions are carried out by binding with specific nuclear receptors that regulate responsive genes encoding for structural and functional cardiac proteins, direct , extranuclear, non transcriptional effects, have also been described. In severe illnesses of non-thyrodial origin including myocardial infarction and chronic heart failure, down regulation of thyroid hormone system and changes in thyroid homeostasis may occur. This condition which has been called “euthyroid sick syndrome” or “ Low T3 syndrome”.
REFERENCES


Pratiksha Chavan*, Sangram Patil, Sangram Madane, A Brief Review on Thyroid Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 3228-3247. https://doi.org/10.5281/zenodo.16406011
 10.5281/zenodo.16406011
10.5281/zenodo.16406011
